Introduction
Female genital cosmetic surgery (FGCS) is advertised widely. The rise in uptake of FGCS [1] is paralleled by the rise in medical publications (Chapter 4 by Rodriguez, this volume). A PubMed search on labiaplasty suggests that the number of articles has tripled over the past few years, from 30 publications between 2008 and 2012 and a further 101 publications from 2013 to 2017 (Figure 6.1). However, high-quality studies that offer reliable evidence for such operations, particularly with regards to risks, benefits and long-term outcome, remain scarce. The vast majority of published peer-reviewed reports are small retrospective case reviews, in which patients are followed up for brief periods only and without the inclusion of a no-surgery or alternative treatment group for comparison. Most of the articles are published by the surgeons who are reporting on the results of operations they themselves have performed. In this chapter, I will review the available scientific evidence for labiaplasty and other FGCS procedures, focusing primarily on satisfaction post-surgery and risks of FGCS, especially labiaplasty. I will furthermore outline the benchmarks for good science to which future clinical research in FGCS should aspire.
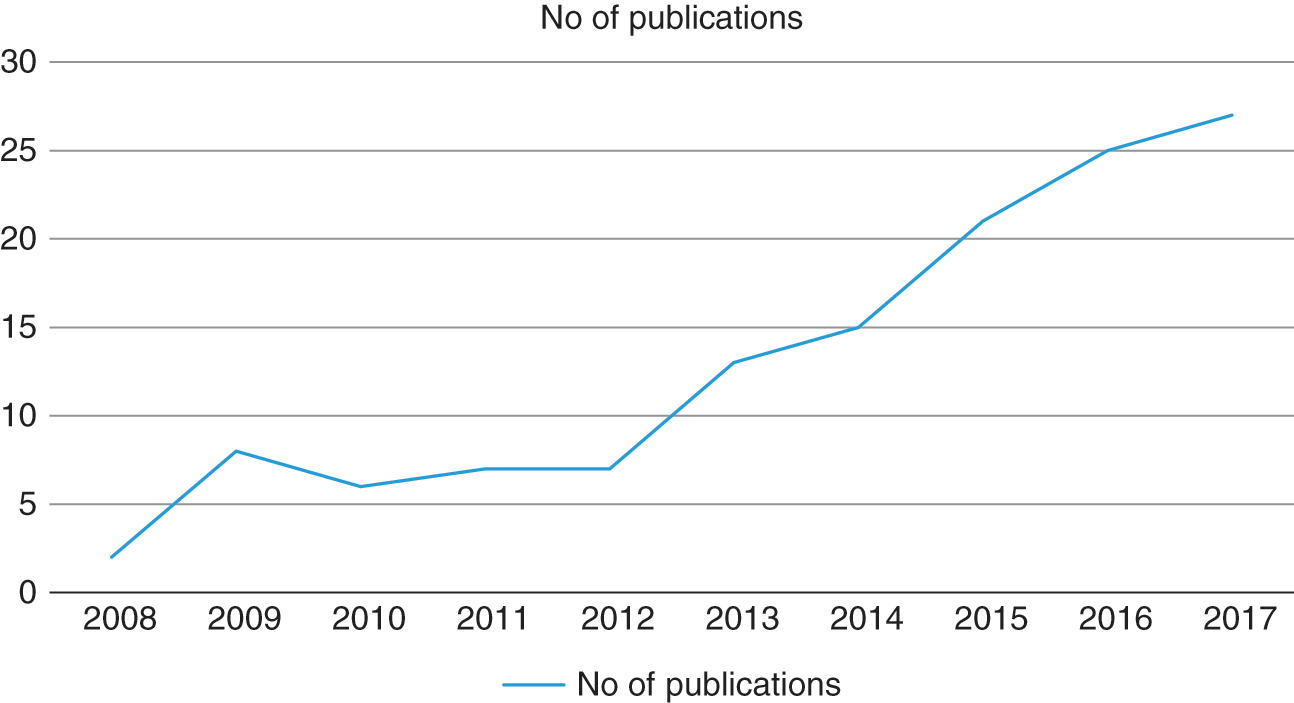
Figure 6.1 Number of publications on labiaplasty, 2008 to 2017.
The ‘Normal’ Vulva
What is positioned (or sold) as ‘normal’ for vulval appearance and function transcends anatomical measurements (Chapter 3 by Braun, this volume). As surgeons, however, anatomy is where we must all begin. This is the first hurdle. Descriptions in anatomy or gynaecology textbooks are at best partial [2] (Chapter 2 by Crouch, this volume). This information has not been developed, for example, by studies that examine the variations in structure and appearance of female genitalia [3]. Aspects of the vagina remain entirely uncharted, not least the existence of the so-called G spot, and if it does exist, where it is located. Equally little has been written or known about the changes during adolescence, nor is there a staging of pubertal development for labial size and form similar to the Tanner staging for breast or pubic hair development. Parents and daughters who come forward with genital appearance concerns may both have been misled by traditional sex education (Chapter 11 by Lundberg, this volume). They rely on paediatricians and general practitioners who may not be in a position to guide them towards a more realistic and sympathetic understanding of their body [4]. All parties are potentially influenced by shared cultural biases.
Implied in most scientific publications aimed at medical professionals or lay people is that there is a standard prototype for female genitalia and it remains static throughout life. This assumption is reproduced in educational materials decade after decade. Myths have morphed into facts that have morphed into common sense, so that few women learn to expect that their genitals can be quite different from each other’s and are, as for the rest of their body, transitional. The variations and usual changes across the lifespan, such as during pregnancy or following a vaginal delivery or menopause, are normal and nothing to fear. Girls and women who undergo FGCS procedures may not realise that the results, even if they were to match expectations exactly, are impermanent, because the body is not a static entity.
Guidelines from Scientific Bodies
In response to the increased demand for FGCS, a number of professional bodies have attempted to provide a framework for medical doctors to work within [5–11], but these are not professional standards that doctors have to adhere to. To put this into perspective, clinical recommendations in evidence-based health care should ideally be established on cumulative evidence leading to at least one randomised controlled trial. This would constitute what clinicians consider Level 1 evidence that makes its way to a Grade A recommendation. In the case of FGCS, guidance provided by professional bodies is at best Grade C recommendations, based usually on non-controlled studies and opinions.
The Society of Obstetricians and Gynaecologists of Canada states that terms such as vaginal rejuvenation, clitoral resurfacing and G-spot enhancement should be recognised as marketing terms only and that misleading advertisements are unethical [11]. In the relevant committee opinion paper, the American College of Obstetricians and Gynaecologists names these procedures ‘not medically indicated’ and stresses that their safety and effectiveness are not documented [7] (Table 6.1).
| Summary of Recommendations | |||||||
|---|---|---|---|---|---|---|---|
| Scientific Body | Type of Paper | Title | Year of Publication | Anatomy | Psychology | Advertising/Financial Conflicts | Complications |
| Society of Obstetricians and Gynaecologists of Canada | Policy Statement | Female Genital Cosmetic Surgery | 2013 | Help women understand anatomy and respect individual variations. | Ascertain the absence of major sexual or psychological dysfunction. Refer for assessment if identified. | Conflicts of interest when advertised. Advertising of FGCS is considered unethical. | Counsel on possible unintended consequences of cosmetic surgery to the genital area. |
| Royal College of Obstetricians and Gynaecologists | Ethical Opinion Paper | Ethical Considerations in Relation to Female Genital Cosmetic Surgery | 2013 | Provide accurate information about normal variations in female genitalia. | Offer counseling and other psychological treatments for body image distress. | Questions advertising practices. Reiterates General Medical Council and Advertising Standards Authority Guidance: publish factual information, encourage honest and trustworthy communication. | Irreversibility of labiaplasty. Inform about risks. Provide accurate written information sheet. |
| The Royal Australian and New Zealand College of Obstetricians and Gynaecologists | Statement | Vaginal ‘Rejuvenation’, Laser Ablation for Benign Conditions and Cosmetic Vaginal Procedures | 2008, Amended 2016 | Educate women on variations in appearance of external genitalia and normal physiological changes over time. | Recommends sexual counseling. Concerns on exploitation of vulnerable women. | Caution in accepting financial incentives from manufacturers of commercial products. | Discuss in detail. Scarring, adhesions, permanent disfigurement, infection, dyspareunia, altered sexual sensation. |
| The Royal Australian College of General Practitioners | Guidance | Female Genital Cosmetic Surgery: A Resource for General Practitioners and Other Health Professionals | 2015 | Use diagrams to educate the patient on normal female external genitalia anatomy; focus on sensorineural and functional aspects. | Take a psychosexual history, consider mental health and relationship or sexual abuse issues and refer accordingly. | Refers to Australian media code of conduct on body image, to place greater emphasis on diversity, positive body image and a focus on health rather than on body shape. | Potential risks associated with FGCS include bleeding, wound dehiscence, infection, scarring, sensorineural complications, dyspareunia, tearing of scar during childbirth, reduced lubrication. |
| American College of Obstetricians and Gynecologists, Committee on Gynecologic Practice | Committee Opinion | Vaginal ‘Rejuvenation’ and Cosmetic Vaginal Procedures | 2007, Reaffirmed 2017 | Engage in frank discussion with women regarding wide range of normal genitalia. | Evaluate for sexual dysfunction, explore non-surgical interventions, counselling. | Ethical concerns regarding marketing and franchising. | Inform regarding complications: infection, altered sensation, dyspareunia, adhesions and scarring. |
| American College of Obstetricians and Gynecologists, Committee on Adolescent Health Care | Committee Opinion | Breast and Labial Surgery in Adolescents | 2017 | Essential to have special knowledge of normal physical and psychosocial growth and development during adolescence. | Screen for body dysmorphic disorder. | Serious complications can occur (pain, painful scarring, dyspareunia, hematoma, edema and infection). | |
| Swiss Society of Gynecology and Obstetrics | Letter of experts | Intervention Vulvo-vaginales sans Indications Medicale | 2011 | Inform women of individual variations in female external genitalia and changes during life. | Gynaecologists should address psychological concerns in women requesting FGCS. | Cosmetic indications only for FGCS. Caution to avoid fraud against medical insurance. | Document counselling of women regarding risks. |
Scientific Evidence on Immediate Results and Patient Satisfaction
Labiaplasty is the most widely performed FGCS procedure. Scientific publications start to appear in the early 1970s [12]. From then and up to the late 1990s, only a handful of case reports or small case series (including up to four patients) can be identified. These reported on satisfaction on anecdotal grounds. From 2000 onwards, publications including larger numbers of women appeared in the literature with a better defined aim to report on postoperative patient satisfaction. However, most reports were still based on relatively small numbers of patients while larger series were flawed by a short follow-up and ad hoc evaluation of patient satisfaction, such as the operating surgeon asking patients face to face or on the telephone yes/no questions that were important from the surgeons’ perspectives.
One of the first case series to comment on satisfaction and complications following labiaplasty was published in 2000 by Rouzier et al. [13], who reported on 163 patients with an age range from adolescence to menopause. This group assessed patients 1 month after labiaplasty with a simple questionnaire devised by the team and reported that 83% of patients were satisfied and only 4% declared that they would not undergo the procedure, given a second chance. In 2002 Pardo et al. [14] followed up 55 girls and women 2 months after surgery. The patients were assessed by a questionnaire devised by the researchers, who reported high satisfaction rates. In a similar fashion, Alter in 2008 [15], Cao et al. in 2012 [16], Gress in 2013 [17] and Gonzalez et al. in 2013 [18] reported on the satisfactory results of different labioplasty procedures performed in their departments. Although the series were fairly large, ranging from 50 to more than 800 patients, follow-up periods were short and the assessment of patients was non-standardised.
As early as the early 1990s some authors attempted to classify ‘labial hypertrophy’ in categories, and this classification has been used subsequently to offer a different surgical approach according to the degree of ‘deformity’. Ellsworth et al. [19] used the Franco classification to determine whether de-epithelisation or edge or wedge resection should be performed. Based on the results of 12 patients, the authors designed an algorithm for triaging women to a specific type of operation. Later reviews of the literature [20, 21] further promoted the notion of a specific technique application depending on labial size and form.
A study by Goodman et al. [22] attempted to offer a multicentre study of the effects of labiaplasty, vaginal rejuvenation and clitoral hood reduction, alone or in combination. Although the study involved 10 US centres and clarified surgical outcomes from different operators, only 258 out of 473 (55%) eligible patients answered the self-designed survey. A 91.6% satisfaction rate was mentioned. Although an overall significant improvement in sexual function was reported, on looking more closely at the results, 150 out of 237 patients who had undergone a surgical procedure reported either a negative (6 women) or no effect (144 women) as far as sexual satisfaction was concerned.
Veale et al. [23] published a prospective case-comparison study looking specifically at psychosexual outcomes using the Genital Appearance Satisfaction scale (GAS), the Hospital Anxiety and Depression Scale (HADS), the Pelvic Organ Prolapse-Urinary Incontinence Sexual Function Questionnaire (PISQ), the Body Image Quality of Life Inventory (BIQLI) and the Cosmetic Procedures Scale-Labia (COPS-L) that screens for body dysmorphic disorder. The researchers assessed women preoperatively and 3 months post-surgery and reported a significant improvement in genital appearance satisfaction that was maintained during a longer term follow-up. There was also significant improvement in the PISQ, COPS L and HADS anxiety scores, suggesting improved sexual function, relief from body dysmorphic disorder and decreased anxiety, respectively. However, the number of patients in the study was small, with 49 women participating out of 112 potential recruits (44%). Furthermore, the drop-out rate was high, with only just over half of the participating patients remaining in the study at the 3-month follow-up.
Subsequently, Goodman et al. [24] used a set of validated questionnaires to evaluate body image, genital self-image, sexual satisfaction and body esteem prospectively. The number of patients participating was 120. The authors included a control group of 50 women not desiring a labiaplasty. Patients were recruited consecutively and the participation rate was high, as was initial follow-up for body image and genital image. The authors reported a significant improvement for all of the variables assessed, including sexual satisfaction. However, on looking at results more closely, only 65 women completed the sexual satisfaction questionnaire and of these just over a third participated in the 2-year follow-up. The report omitted the number of women contacted for the research and, without knowing the participation rate, it is not possible to determine how generalisable the results area. Although the abstract states that sexual satisfaction values for the operated women ‘surpassed’ control values at 2 years post-surgery, this represents an over-conclusion given the flaws of the study.
More recently, a different type of study by Placik and Arkins [25] attempted to evaluate genital sensitivity after labia minora and clitoral hood reduction. The authors measured sensitivity to pressure using Semmes–Weinstein monofilaments, at five genital locations at baseline and at 3, 6 and 12 months after surgery. They reported a slight drop in pressure threshold at the edge of the labia that reached statistical significance, suggesting improved labial sensitivity at the point of excision. However only 37 out of a potential 120 women participated in the study, making it difficult to determine the generalisability of the results.
A positive improvement in providing evidence regarding labiaplasty is the involvement of psychologists in the independent evaluation of patients. In two recent studies by Sharp et al. [26, 27], patients were assessed, either through questionnaires or interviews, regarding their current satisfaction with a procedure performed in the recent past and whether they acknowledge an improvement, with regards to their previous state of sexual satisfaction or genital appearance satisfaction. Both studies reported improved outcomes after surgery, albeit decreasing, as follow-up time progressed. Interestingly, one in three patients retained their sexual difficulties after surgery. Once more, limitations stemmed from the small number of participants and the retrospective nature of the studies.
Evidence on results of FGCS procedures marketed as G-spot amplification or revirgination does not exist and therefore no scientific comment can be made on their effectiveness. However, a number of papers have recently been published on vaginal rejuvenation, aimed primarily at treating ‘vaginal laxity’. Traditionally, vaginal laxity is treated surgically through colporrhaphy and perineoplasty, which are operations to tighten the vagina. Few studies exist to assess the effectiveness of surgical vaginal rejuvenation, and long-term follow-up beyond 6 months is non-existent. Pardo et al. looked at post-surgical results at 6 months in 53 women who underwent a colporrhaphy to treat vaginal laxity. Sexual function was assessed arbitrarily and was reported as improved in 90% of patients [28]. A later study in which a validated questionnaire was used to measure sexual function postoperatively found that vaginal tightness was achieved at the expense of dyspareunia (pain during sex), thus defeating the purpose of improving sexual function [29]. Recently, an American group assessed 78 women presenting with vaginal laxity post vaginal rejuvenation, using the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire-12 (PISQ-12). The main drawback of the study was the vague definition of vaginal laxity, particularly as some women were as young as 25 years of age. The authors suggested improved postoperative sexual function scores in most domains of the PISQ, except for pain scores, which remained unchanged [30].
Newer non-surgical vaginal rejuvenation techniques, using radio frequency [31], laser [32] or silicone threads [33], aim to improve sexual function while avoiding invasive surgery. All techniques are relatively new, and evidence regarding results is again scanty. Radio frequency vaginal rejuvenation has been assessed in a well-designed multicentre randomised trial with a placebo arm (sham treatment), to assess improvement of vaginal laxity at 6 months after treatment [34]. In the treatment group, 43.5% of women had an improvement in vaginal laxity with improved FSFI scores. However, there was an unexpectedly high improvement, of 20%, in the placebo-treated group, who were blinded to the fact they were not receiving treatment, suggesting a strong placebo effect. The study was sponsored by the company marketing the radio frequency vaginal rejuvenation device. As vaginal rejuvenation is extremely profitable, more such studies are likely to be published in the future but the quality of the research should be even more closely scrutinised.
Related posts:
 Chapter 2 – Female Genital Anatomy
Chapter 2 – Female Genital Anatomy
 Chapter 11 – Can Better Sex Education Tackle the Rise in Female Genital Cosmetic Surgery?
Chapter 4 – The History of Female Genital Cosmetic Surgery in the United States
Chapter 14 – Addressing Female Genital Dissatisfaction and Distress
Chapter 11 – Can Better Sex Education Tackle the Rise in Female Genital Cosmetic Surgery?
Chapter 11 – Can Better Sex Education Tackle the Rise in Female Genital Cosmetic Surgery?
Chapter 4 – The History of Female Genital Cosmetic Surgery in the United States
Chapter 14 – Addressing Female Genital Dissatisfaction and Distress
Chapter 11 – Can Better Sex Education Tackle the Rise in Female Genital Cosmetic Surgery?
 Chapter 2 – Female Genital Anatomy
Chapter 2 – Female Genital Anatomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


