Chapter 48 LOWER EXTREMITY RECONSTRUCTION
The surgeon’s therapeutic arsenal for reconstruction of the limbs has recently increased with the advent of a filling technique that is reliable, well codified, and calls for the use of autologous tissue: structural fat grafting. Although this technique owes its rapid development above all to facial aesthetic surgery, it has already found application in reconstructive surgery of the face and breasts. Fat grafting is also a viable option for improving the contours and volumes in lower limb recontouring and reconstruction.
Augmentation of the volume of the calves 1 , 2 and buttocks 3 – 6 with silicone implants was first described in 1979. Descriptions of the use of fat grafting in the limbs were published in 1992 and primarily concerned the hand, 7 , 8 buttocks, and calves. 9 – 17 In this chapter we will present the use of fat grafting in lower extremity reconstructive surgery as described by Coleman, 7 , 18 – 24 and we will discuss the evolution of microfat grafting. 25 – 26
Material and Methods
INDICATIONS
Volume deficits of the lower extremities can be divided into two general categories: (1) those in patients with significant hypotrophy or atrophy of an entire limb or a segment of a limb with asymmetry, and (2) those in patients with localized lesions of a limb involving one or even several regions of the limb but with no comprehensive hypotrophy or atrophy of the limb.
The causes of volume deficits in the soft parts of the lower extremity that can be treated with fat grafting are as follows:
Reconstructive surgery
Traumatic scars 27
Iatrogenic tissue damage, especially after pediatric limb surgery or radiotherapy 28
Congenital deformities, such as clubfoot or unilateral limb hypotrophy 10 , 12
Tumoral tissue damage from resection or radiotherapy
Sequelae of infection
Aesthetic surgery
Fat transfer for aesthetic purposes
Benslimane 29 highlighted the beauty standards of the lower limbs. Changes in fat distribution can be addressed by combining liposuction with reinjection of fatty tissue; for example, suctioning of the ankles and inner aspects of the knees, with augmentation of the calves.
Fat grafting to improve contours after a silicone implant is placed
ANALYSIS
Two principal parameters are analyzed clinically when fat grafting in a limb is being considered:
The volume deficit is compared with that of the contralateral limb. The size of the volume deficit is estimated by measuring the surface and mean depth of the defect and by taking its general shape into account. The degree of asymmetry is assessed in a hypotrophic extremity. This asymmetry is generally caused by hypotrophy of both muscle and subcutaneous tissue. A comparative measurement of limb circumferences at different levels of the limbs is useful in planning the procedure.
The quality of the cutaneous covering and its ability to stretch are decisive. This helps the surgeon to determine the number of procedures required to correct the estimated volume deficit.
TECHNICAL GUIDELINES
Before a procedure can be scheduled, all limb wounds must be healed, the patient must be free of infection, and the skin of the extremity must be prepared with massage or lymphatic drainage to improve its capacity for distention.
The donor and recipient sites are defined and marked before the surgery with the patient in an upright position. The patient can help by showing the surgeon the areas that most concern him or her. When a patient has limb asymmetry, we always use the contralateral limb as the donor site to reduce the asymmetry; both liposuction of the contralateral limb and filling of the hypotrophic limb are performed.
We prefer to use general anesthesia, because it allows us to work on both lower limbs for harvesting and infiltrating. Because the patient is under general anesthesia, we do not infiltrate lidocaine or epinephrine in the donor and recipient sites.
TECHNIQUE
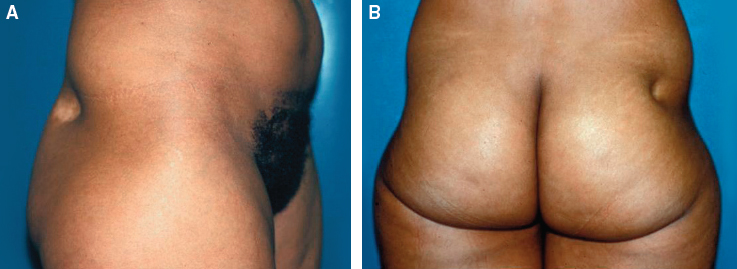
This 39-year-old woman presented with cortisone lipoatrophy of the right buttock after injection of a delayed-action corticoid. The volume deficit was estimated to be 40 cc by measuring the surface (20 cm2) and the mean depth (2 cm) of the defect.
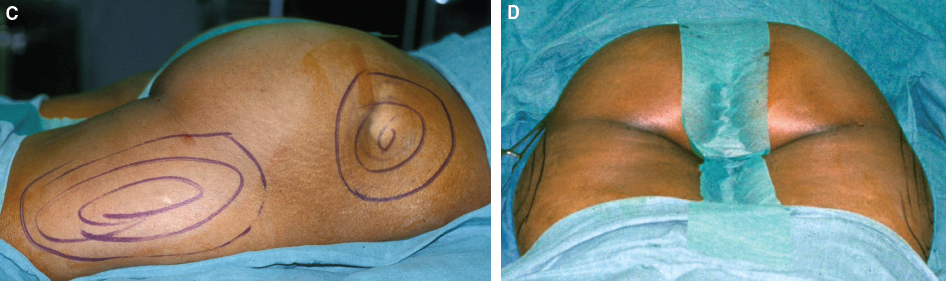
The preoperative markings determine the position of the incisions and the harvesting and grafting areas. The procedure is performed with the patient under general anesthesia.
Incisions
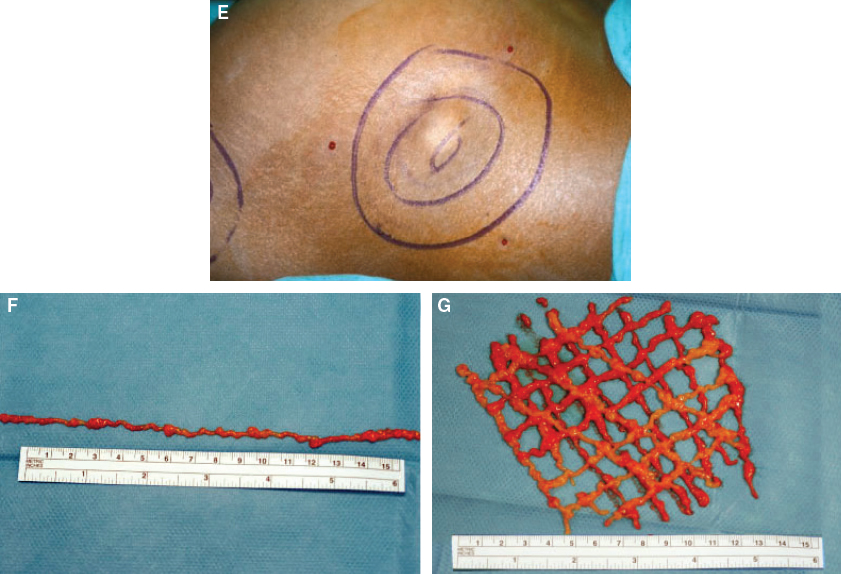
Fat injection is performed through multiple 2 mm incisions distributed in a radiating manner around the area with a volume deficit (E), thus making it possible to crisscross the different injection axes in three spatial planes. The aim of this method is to inject the fat throughout the recipient tissue in three spatial planes with each containing a small quantity of fat (F and G).
Level of Infiltration
In our patients, we always graft fat into subcutaneous tissue. It can also be grafted into the muscle compartment, especially in cases of limb asymmetry with amyotrophy, but during an intramuscular injection, there is a risk of acute compartment syndrome, particularly in the leg. It must be prevented by a surgical fasciotomy, performed with two or three short incisions on the leg. Fasciotomies are performed for each compartment that is injected, only when the grafted fat is placed into the muscular layer. Thus, one fasciotomy is generally performed for the anterior compartment with a 2 cm cutaneous incision, which allows for the performance of a complete vertical fasciotomy of the anteroexternal muscular compartment of the leg. A second fasciotomy is performed for the posterior compartment through a 2 cm posterior approach, with a complete vertical fasciotomy in between the two gastrocnemius muscles. In our experience, postoperative pain and risk of acute compartment syndrome can be decreased by avoiding the muscular placement of the fat and putting it exclusively into the subcutaneous layer, during multiples steps if required.
Volume Ranges
The volume of fat grafted varies, depending on the indication for lower limb reconstruction. In our experience, for limb asymmetry, the mean volume injected is about 80 to 100 cc per session, usually in a two-stage approach. For a localized lesion, the volume depends on the size of the defect and can range from 4 to 180 cc.
Harvest and Surgical Technique
The surgeon must be prepared for the need for more than one procedure to achieve the desired results. In such cases, procedures need to be performed at a minimum interval of 6 months. The key is not operating too quickly on the patient but waiting for the end result. Radiating tunnels are used for fat injection through multiple incisions.
We use the structural fat grafting technique described by Coleman. 7 , 13 – 15 , 17 – 19 Fat is harvested from the lateral part of the thighs to the right buttock with a two-hole Coleman harvesting cannula attached to a 10 cc Luer-Lok syringe. Fatty tissue is obtained through multiple 3 mm incisions around the harvest areas. We select several sites to ensure the best quality of fatty tissue. A quality graft is one with the lowest possible proportions of oil and blood residue after centrifugation. This can be ensured by avoiding mechanical trauma to the tissue and by harvesting moderate quantities at each site.
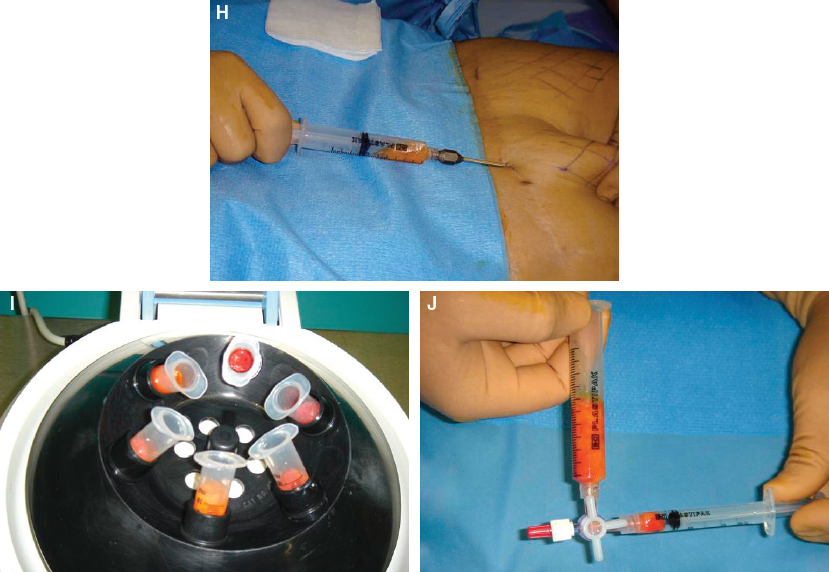
The fat is harvested with a 10 cc Luer-Lok syringe and a Coleman harvesting cannula. The fatty tissue is centrifuged at 3000 rpm for 3 minutes with a MediLite centrifuge; this separates the components into three fractions—oil, fatty tissue, and residue, layered by density. The residual fatty tissue is transferred to smaller cannulas for infiltration using a three-way Luer-Lok.
Related posts:
 Chapter 47 FAT GRAFTING OF THE FEMALE GENITAL AREA
Chapter 47 FAT GRAFTING OF THE FEMALE GENITAL AREA
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


