Chapter 47 FAT GRAFTING OF THE FEMALE GENITAL AREA
There are several indications for fat grafting of the female genital area. Because of the high vascularization and tissue laxity, the resorption rate of grafted fat is low. Fat grafting can be useful in aesthetic gynoplasty, adding volume to the labia majora or vulvar structures, and in functional gynoplasty, for the treatment of scars, radiodermatitis, atrophy, pain, and laxity.
Principles
FEMALE GENITAL ANATOMY
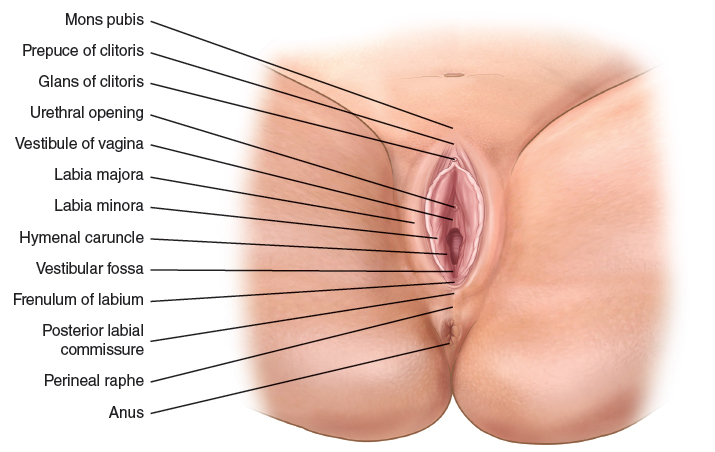
Labia majora

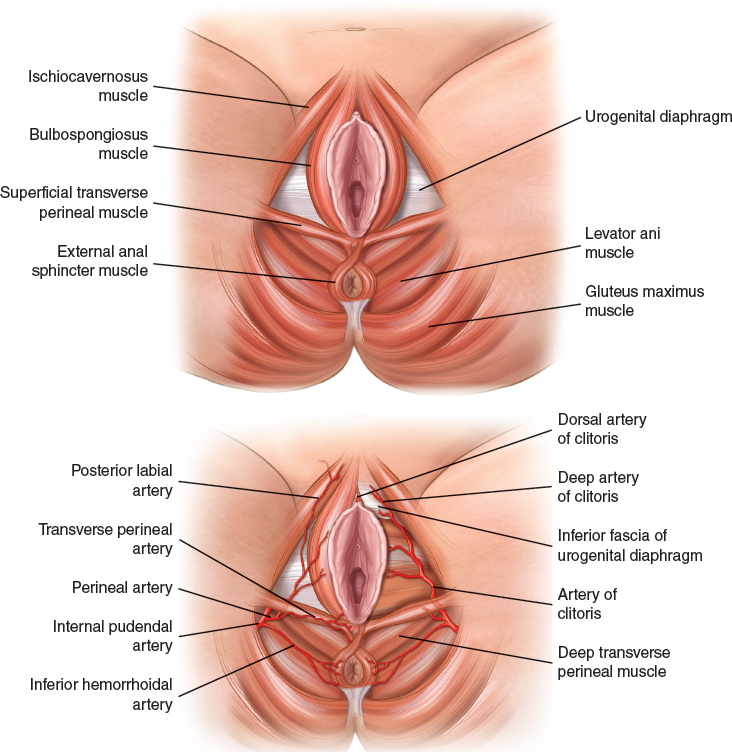
The labia majora are 7 to 8 cm long, 3 to 4 cm wide, and 2 to 5 cm thick; they extend between the pubis and approximately 3 cm from the anus. The subcutaneous tissue consists of loose areolar tissue that is rich in fat, and superficially, sebaceous glands. Vascularization is provided by a rich anastomosis of branches of the internal pudendal artery: posterior labial branches, branches of the pudendal artery, and branches of the perineal artery. No major vessels are found in the labia majora.
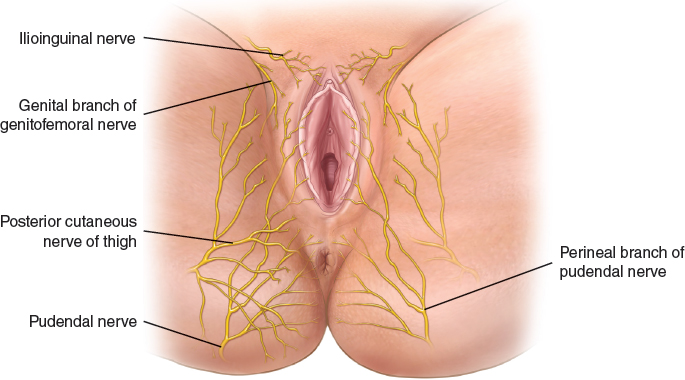
Innervation of the labia majora is from the perineal and labial branches of the perineal nerve. Lymphatic drainage is to the superficial inguinal lymph nodes.
Interlabial Sulcus
The interlabial sulci, left and right, separate the labia minora from the labia majora.
Labia Minora
The labia minora are 4 to 6 cm long and 2 to 4 cm wide; they extend off the vestibule of the clitoris, next to the prepuce of the clitoris. The subcutaneous tissue consists of firm connective tissue, erectile tissue, and elastic fibers, with no adipose tissue. The nervous and vascular fascicle underlies all of the labium. Vascularization is provided by the labial artery and vein, which run at the base of the labia and give branches to the labial crest that anastomizes superiorly with the periclitoral branches of the dorsal artery of the clitoris. 1 Innervation is by the labial nerve, which runs with the vessels and gives terminal branches to the labial crest and the labial walls. 2
Clitoris
The clitoris, a double-arch–shaped erectile organ, is 2 to 3 cm long. The first arch is composed of three parts (three corpora cavernosa, the clitoral crura, and a footing with the suspensory ligament), whereas the second arch is composed of two bulbs (1 to 3 cm long) located in the lateral superior portion of the vagina. Arterial supply to the clitoris is provided by the deep arteries that supply the corpus cavernosum; the arteries of the bulb supply the bulb of the vestibule. The dorsal artery of the clitoris runs on the dorsum of the clitoris to the glans, where it divides into branches that supply the glans and prepuce.
The dorsal veins are the most relevant and drain into the internal pudendal veins. Innervation to the clitoris is provided by the inferior hypogastric plexus and the pudendal nerve. 3
Vagina
The length of the vagina is approximately 7.5 to 9 cm. The vaginal lumen varies in size, with some anatomic variations, and alterations resulting from vaginal delivery of a baby. The vagina is an elastic, muscular tube paved by mucosa with an underlying lamina propria of connective tissue, then a thin layer of smooth muscle, followed by the adventitia, a thin layer of dense connective tissue. The lamina propria of the mucosa contains elastic fibers as well as a dense network of blood vessels, lymphatics, and nerves. Transudate from blood vessels, combined with cervical mucus secreted by glands, provides lubrication during sexual arousal and intercourse.
The vagina is divided into four fornices: one anterior, one posterior, and two lateral. In the anterior fornix, deep to the mucosa, a thin layer of loose areolar tissue can be found in the midline that runs from the urethra and is covered by the urethral sphincter. Posteriorly, the rectovaginal space hosts the rectum muscle and the rectal fascia. In the first 4 to 6 cm, the space is thicker (2 to 5 cm) and progressively becomes thinner. The mucosa of the two lateral fornices is firmly attached to the bulbocavernosus muscle by a network of fibers The bulbocavernosus muscle is thin, 0.5 to 1.5 cm thick. Laterally, the ischiorectalis fossa hosts a fat pad that separates the pubococcygeal muscle from the ischiocavernosus muscle. Inside the fat pad run small branches of the perineal artery, and more posteriorly, of the internal pudendal artery. 4
The arterial supply to the vagina arises from three sources:
Vaginal branches of the uterine artery for the upper vagina
The vaginal arteries, branches of the hypogastric artery, to the middle vagina that penetrate the vaginal tube perpendicularly
The middle hemorrhoidal and clitoral arteries that send branches to the inferior portion of the vagina
The nerve supply to the vagina is from the autonomic nervous system. Sensory fibers arise from the pudendal nerve, and pain fibers are from sacral nerve roots.
Lymphatic drainage of the vagina is generally to the internal and external iliac nodes and the superficial inguinal and perirectal nodes.
PHYSIOLOGY: THE EFFECTS OF HORMONES, SENESCENCE, AND VAGINAL DELIVERIES
Vulvovaginal tissues are highly affected by changes in estroprogestinic levels, resulting in their trophism and imbibition. Poor hormonal levels therefore cause senescence in tissues. 5 The aging process causes a diminished trophism of the vulvovaginal structures: reduction of fat deposits of labia majora, with a “sagging bag” aspect, and reduced trophism of the labia minora; reduction of the fat pad of the ischiorectalis fossa; and reduction of trophicity of the vaginal mucosa and lamina propria. 6 The complex myotendinous system loses power and volume with aging. 7 , 8
IDEAL APPEARANCE OF THE FEMALE GENITALIA
A canon of beauty of the female genitalia has never been defined. However, despite the wide anatomic variation of the vulva, it is still possible to outline an ideal of female genital beauty by referring to the genital features of young women, as for the canon of beauty of the breast, face, eyelids, and so on. The labia majora should appear puffy and turgid; the labia minora must be partially hidden by the labia majora and protrude by 1.5 to 3 cm; the clitoris should not be excessively prominent, and its prepuce should be in continuity with the labia minora. The vaginal ostium should not be exposed.
Methods of Fat Grafting of the Female Genitalia
PREOPERATIVE EVALUATION: GENERAL CONSIDERATIONS
A candidate for fat grafting of the genitalia must demonstrate good general and local health, and the genital area must be in good condition, without signs of inflammation. It is useful to restore the vaginal pH if it is altered.
The least invasive procedures can be carried out under local anesthesia with or without sedation; spinal or general anesthesia is used for the most complex procedures. Most procedures can be performed in 1-day surgical settings.
A solution of saline plus epinephrine plus ropivacaine (Naropin) is infiltrated in a 1:1 ratio to the volume of the area to be treated. The purpose is to obtain vasoconstriction, reducing the caliber of the vessels. Injection is performed with blunt 14-gauge cannulas.
INDICATIONS AND SPECIAL CONSIDERATIONS
Fat grafting is indicated to improve female genitalia in the following cases:
Poor volumes
Retracted scars from surgery
Cutaneous and mucous atrophies and dystrophies
Pain syndromes
A distinction should be made between safe, moderate, and high-risk areas for fat injection to avoid potential complications.
Safe Areas for Injection
Labia majora
Periclitoral area: Superficial layers around the clitoris are safe areas to inject, with care to avoid the nervous-vascular bundle running perpendicular to the clitoris
Lateral-anterior portion of vaginal walls
Inferior rectovaginal space (3 to 5 cm from the introitus)
Moderate-Risk Areas: Injections Must Be Performed With Great Care
Labia minora: The labial artery courses at the base of the labia; the surgeon placing fat grafts in the labia minora should be aware of this vessel and should avoid the use of small cannulas and needle.
Anterior vaginal wall: No fat should be placed close to the urethra, unless treatment of urinary incontinence is considered, to avoid potential perforations and urethral distortions.
Lateral to the bulbocavernosus muscle: The ischiorectalis fossa contains branches of the perineal and internal pudendal artery.
Perineal area close to the rectum: There is a risk of perforations.
High-Risk Areas
Major vessels can be found in the deep layers. The surgeon must avoid fat grafting where major vessels run and exercise special care injecting close to the rectum, urethra, and peritoneum.
Superior vaginal walls can present problems for fat grafting, as a result of the very short distance between the vaginal walls and the bladder and peritoneum; ultrasound-guided injections are recommended.
The superior part of the rectovaginal septum requires caution because of the thinness of the septum itself.
Clinical Applications
GENERAL CONCEPTS
Different indications call for specific techniques of harvesting, processing, and placement of fat grafts.
Volume Enhancement
Harvesting with 2 mm cannulas
Centrifugation at 3000 rpm for 2 minutes
Fat grafting with 1.20 mm (18-gauge) 1.60 mm (16 g) blunt cannulas
Related posts:
 Chapter 48 LOWER EXTREMITY RECONSTRUCTION
Chapter 48 LOWER EXTREMITY RECONSTRUCTION
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


