Chapter 44 PERCUTANEOUS APONEUROTOMY AND LIPOFILLING AS A REGENERATIVE TREATMENT ALTERNATIVE FOR DUPUYTREN′S DISEASE
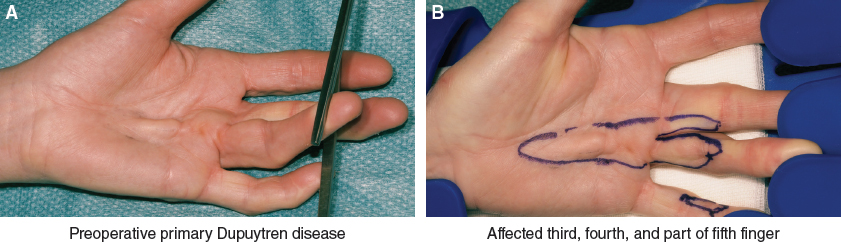
Dupuytren disease is a common progressive fibroproliferative disorder of the palmar fascia leading to digital flexion contractures significantly impairing hand function. 1 It is classically described by the initial appearance of palmar nodules characterized by cell proliferation and high cellularity of contractile myofibroblasts that progress to form fibrotic cords leading to digital contractures. 2 Digital contractures are most commonly treated by surgical excision, limited fasciectomy (LF), or using less-invasive alternatives such as needle aponeurotomy (NA) and collagenase injections. NA was introduced by Lermusiaux in 1972, popularized in the United States, and evaluated by Foucher and van Rijssen. 3 – 5 These less-invasive treatment alternatives are gaining popularity because they promote earlier postoperative recovery, despite their higher recurrence rate. 6 , 7
In an effort to reduce the high recurrence rates associated with NA, our group tested a novel treatment strategy using a more extensive percutaneous aponeurotomy and lipofilling (PALF). 8 The technique disintegrates the fibrous cord through numerous superficial nicks along its course and releases the skin from the subcutaneous layer. The goal is to transform the cord into a loose fibrous recipient matrix into which we inject autologous lipoaspirate. This restores the subdermal fat deficiency and, by being interposed between the transected cord ends, prevents them from scarring back together. 9
In the early twentieth century, fat had already been used to infiltrate the diseased area in an attempt to treat digital contractures. 10 Furthermore, the lipoaspirates contain stem cells and there is now increasing evidence for the role of stem cells as a potential treatment strategy to decrease fibrosis. 11 , 12
We have shown that stem cells derived from adipose tissue inhibit proliferation of contractile myofibroblasts. 13 Myofibroblasts are the key cells leading to fibroproliferation causing flexion contractures. 14 Therefore inhibiting these myofibroblasts using lipofilling containing adipose-derived stem cells (ADSCs) represents a treatment strategy in inhibiting Dupuytren disease.
In this chapter, we will describe the benefit of fat grafting in conjunction with extensive percutaneous aponeurotomy as a treatment strategy for Dupuytren disease. We will discuss the basic scientific research on the effects of ADSCs on Dupuytren myofibroblasts and review the clinical results of our PALF procedure.
BASIC SCIENCE RESEARCH
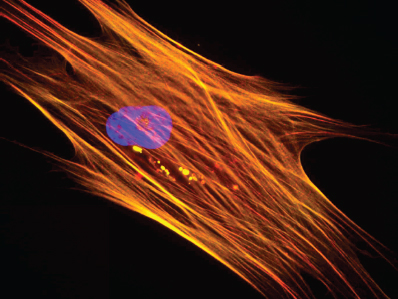
To study the effects of stem cells on Dupuytren myofibroblasts, we obtained tissue samples following informed consent (MEC-2010-294). Dupuytren myofibroblasts were isolated from nodular tissue from patients undergoing surgery, and human dermal fibroblasts were isolated from full-thickness skin samples. This actin cytoskeleton was visualized with a-SMA (red) and F-actin stain using phalloidin (yellow), and the nucleus was stained with DAPI (blue). ADSCs were purchased from Lonza (Berkshire, UK).
Co-cultures of different cell proportions of myofibroblasts (100%, 75%, 25%, 0%) combined with ADSCs or control dermal fibroblasts were cultured for up to 5 days to evaluate proliferation rates. For experiments to examine the effect of soluble factors on proliferation, supernatants of myofibroblasts, ADSCs, and direct contact cultures (50% myofibroblasts combined with 50% ADSCs) were harvested after 24 hours, and myofibroblasts were cultured for up to 5 days in these supernatants.
Cell proliferation was measured using a 5-ethynyl-2?-deoxyuridine microplate assay, which incorporates into DNA during active DNA synthesis, and assessed with a fluorescent microplate reader by measuring excitation/emission at a wavelength of 560 to 585 nm. To assess DNA content for proliferation studies, cultures were stained with Hoechst 33258 dye and analyzed with a fluorescent microplate reader by measuring excitation/emission at a wavelength of 350 to 460 nm.
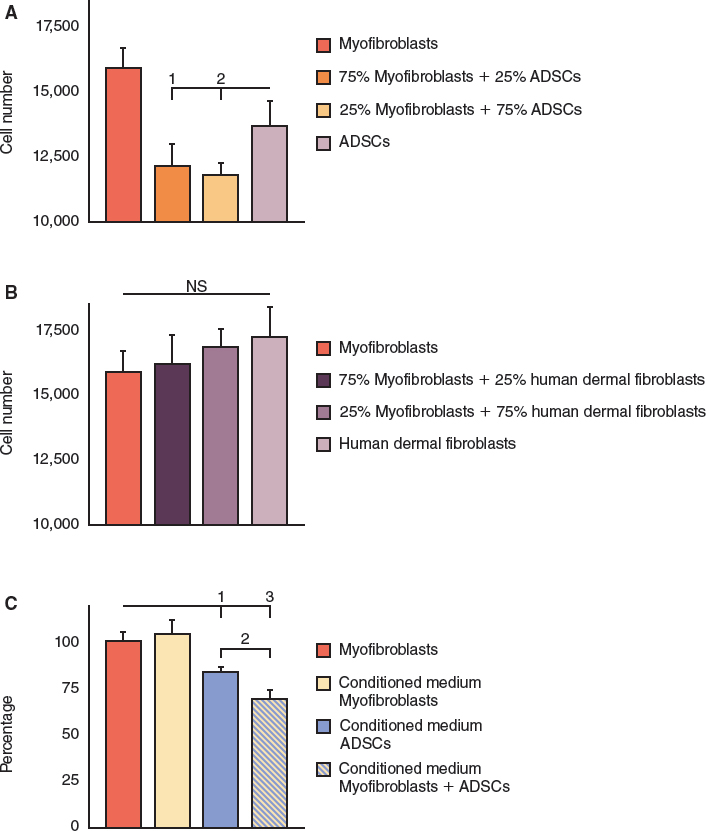
Co-cultures of myofibroblasts combined with ADSCs led to a reduction in cell number at day 5 compared with myofibroblasts cultured without ADSCs (p <0.05) (A), whereas co-cultures of myofibroblasts combined with control dermal fibroblasts demonstrated no difference in proliferation (B).
Supernatants taken from ADSCs led to decreased myofibroblast cell number at day 5 (p <0.05), whereas supernatants taken from myofibroblast cultures had no effect (p = 0.93) (C). Subsequently we tested whether direct contact cultures influenced soluble factors produced by ADSCs by culturing myofibroblasts in supernatants taken from direct contact cultures (50% myofibroblasts combined with 50% ADSCs). Supernatants of direct contact cultures led to decreased myofibroblast cell number at day 5 (p <0.001), a significant decrease compared with supernatants from noncontact ADSC cultures (p <0.05). 13
Patients and Methods
PATIENT SELECTION
Ideal candidates for this technique are patients who want to minimize recovery time and have multiple affected digital rays. Young women with a recurrent proximal interphalangeal (PIP) joint contracture or with severe diathesis are less suited. PIP joint contractures, especially when they are of long-standing, are difficult to fully release because of inherent joint contractures and attenuation of the central slip extensor tendon.
We do not recommend the PALF procedure for treating patients who have undergone previous flap surgery in the affected area, because the scarred neurovascular bundles are no longer loose and therefore as vulnerable to be severed by the needle as the recurrent cord and the surrounding scar tissue.
PALF PROCEDURE
To harvest the fat, the designated donor area (typically the abdomen or flanks) is infiltrated with a mixture of 500 ml 0.9% sodium solution combined with 20 ml of lidocaine and 0.5 mg epinephrine 1:200,000 and sodium bicarbonate. The harvested fat is not centrifuged but is simply processed by gravity sedimentation. The sedimentation takes approximately 10 minutes per 5 ml. The tumescent fluid is drained away, and the fat is not strained and is minimally exposed to air.
The PALF procedure can be performed in an outpatient clinic with proper facilities or in daycare facilities. Patients are placed in the supine position, and the affected arm is placed on an arm board. Several forms of anesthesia may be used:
A locoregional block for the upper extremity, combined with a local anesthetic for the area to be liposuctioned to harvest fat
General anesthesia
Peripheral isolated or combined nerve block, together with a local anesthetic for the area to be liposuctioned
Local superficial anesthesia of the affected fingers, combined with a local anesthetic for the area to be liposuctioned
After complete exsanguination of the affected digital ray, it is placed under maximal forced extension with a rather stiff but still pliable hand retractor.
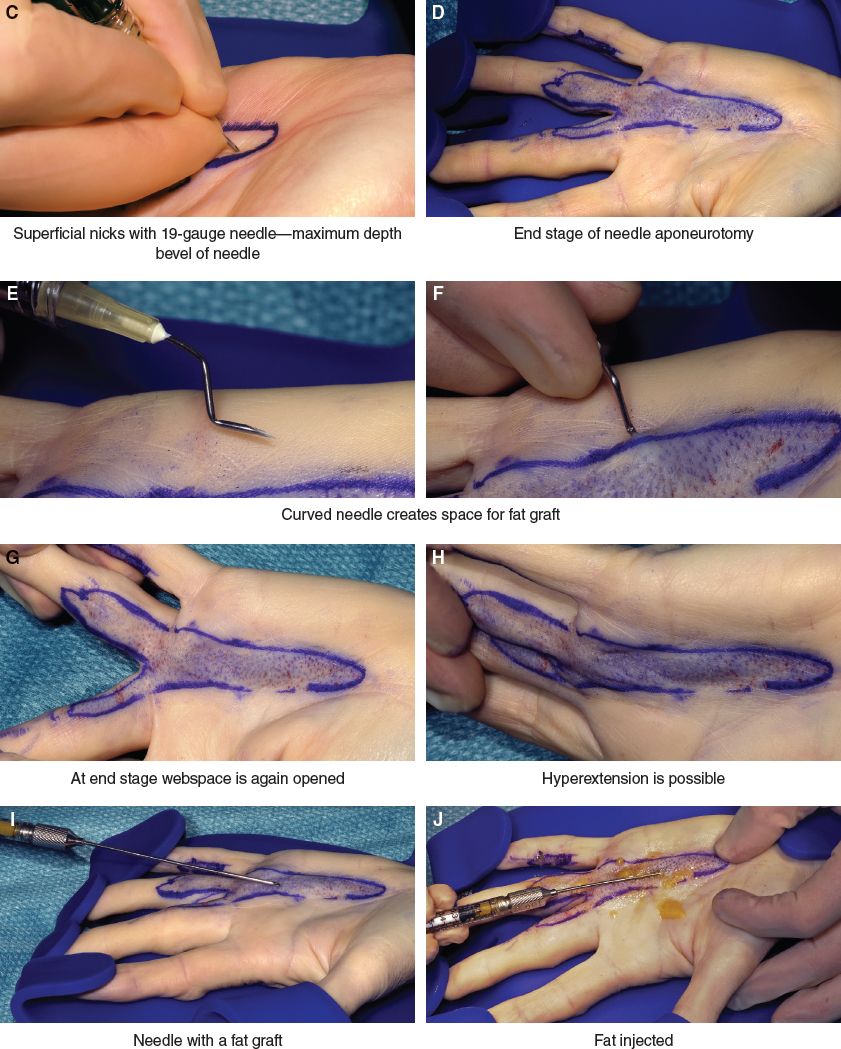
A 19-gauge needle is used to make multiple staggered punctures along the whole cord in an orderly fashion, starting proximally and moving distally as the cord is severed by gentle lateral oscillation of the needle tip. Control of the penetration depth is gauged by the bevel of the needle, since this will prevent damage to the arteries and nerves of the digit. Proximal to the transverse palmar crease, a puncture depth of 2 to 3 mm can be used; beyond that level, a depth 1 to 1.5 mm is appropriate, depending on the thickness of the skin.
A blunt-tipped 14-gauge cannula is used to inject the harvested lipoaspirate into the palm and digits through two or three needle puncture sites. On average, a total of 10 to 15 cc of very loose decanted lipoaspirate per digital ray is injected. Some of the lipoaspirate will escape through the needle release sites. Slight ballooning of the palmar skin is acceptable, because the injected fat is very dilute.
During surgery the contracted fingers should remain under constant strong extension with a lead hand retractor. This tension is necessary to localize residual restricting bands until the contracture is fully released. The surgeon must be aware that the needle will cause the taut restrictive fibers to snap while sparing the looser neurovascular bundles. This constant tension will ensure the selective cutting ability of the needle tip and the safety of this procedure. After longitudinal release of the cord, an angled needle is introduced and with a sweeping windshield-wiper arc of motion in the subdermal plane, the cutaneous insertions of the cord are further released.
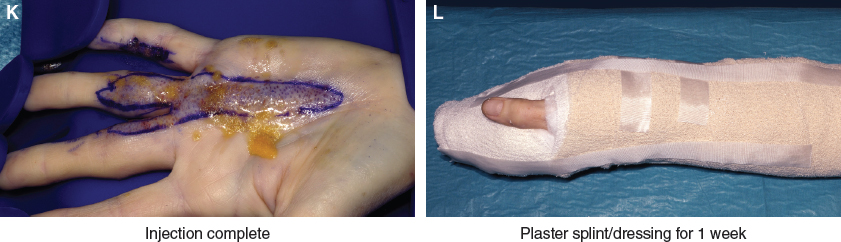
After surgery, a plaster extension splint with an incorporated dressing is applied to the operated hand. The splint is removed in 5 to 7 days in the outpatient clinic, and the patient is allowed to return to his or her normal activities. Patients are advised to wear night extension splints for up to 4 months, but many patients are noncompliant. After open surgery no beneficial effect of a postoperative extension splint has been demonstrated; therefore it could be debated whether a posttreatment splint is necessary for PALF patients.
The duration of a PALF procedure is typically the same time as for an LF surgery; this of course depends on the number of fingers involved and the extent of the disease. A significant advantage of this technique is the ability to treat all rays in one procedure, in contrast to open surgery, where rarely more than two rays can be safely treated in one session. 7
Related posts:
 Chapter 43 HAND AND FOREARM REJUVENATION
Chapter 43 HAND AND FOREARM REJUVENATION
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


