Chapter 43 HAND AND FOREARM REJUVENATION
Aesthetic Considerations
The hands are visible unclothed areas of the human body and one of the first areas to show signs of aging. Although some physicians believe that because fat is lost with aging, placing fat into the dorsum of the aging hand is justifiable, but it is not fat that is missing from the older hand. The dorsum of the normal hand is not a repository of fat, and an attractive young hand is full, not fat. The key to successful rejuvenation of the aging hand is to create an integrated layer of fat grafts over the dorsal hand that makes the skin look and feel thicker, with a slight subcutaneous fullness.
The dorsum of an attractive, healthy-appearing hand has a slight subcutaneous fullness that obscures veins and tendons but does not hide them. The tendons are more defined when the metacarpophalangeal (MCP) joints of the wrist are extended than when they are flexed or are in repose. The superficial veins are usually discernible, and the more slender and athletic an individual, the larger and more distinct these veins appear. The blue color of the veins can be seen through the skin, but the white tendon color is not usually discernible. There is a generalized fullness of the skin and subcutaneous tissues that adds volume to the nonbony hand and frames the joints with a youthful fullness.
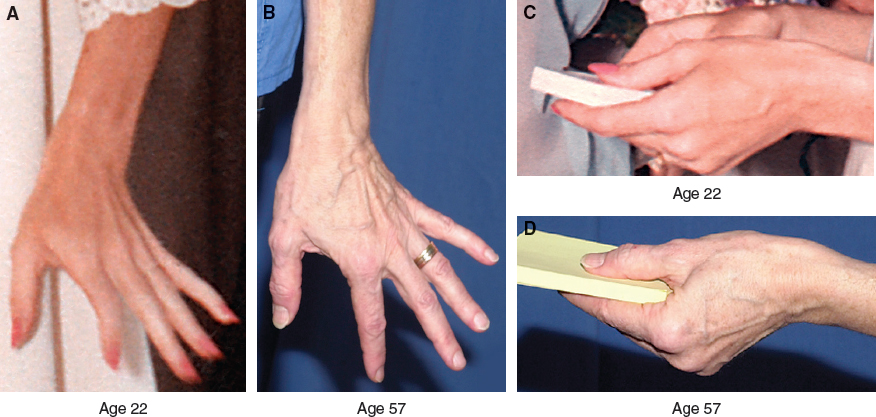
The tendon area is clearly visible in the photos of this patient taken when she was 22 years old. There is a hint of veins visible through the skin, especially around the proximal phalanges and over the index metacarpal. By age 57, the subcutaneous structures of her hand are more visible with the skin of the dorsal hand clinging to the tendons and most of the circumference of the veins protruding from of the confines of the hand. As the fullness is lost, the joints appear larger and become more defined. The thumb MCP and proximal interphalangeal (PIP) joints appear especially large compared with the earlier photo of her hand.
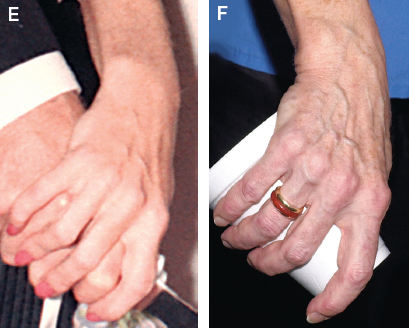
As the fullness of the hand is lost with advancing age, the joints become more isolated. The veins are more obvious both in shape and color and the tendons’ whiteness glistens more through the thinning skin. Subtle fullness over the hands and fingers is the element missing from the older hand.
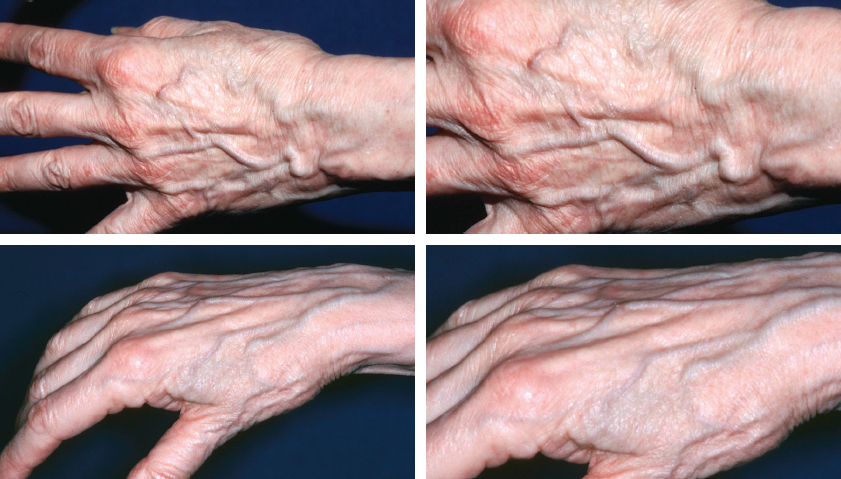
In the aging hand, generalized subcutaneous fullness gradually disappears as the subcutaneous tissues and skin atrophy. With loss of fullness, the veins appear more prominent, their blue color deepens, and the extensor tendons appear whiter and more visible through the thin skin of the dorsal hand. The tendons are prominent even at rest or with flexion of the MCP joints. With the loss of supporting fullness under the dermis and a gradual diminution of elasticity, the skin’s texture becomes more crepey and wrinkled.
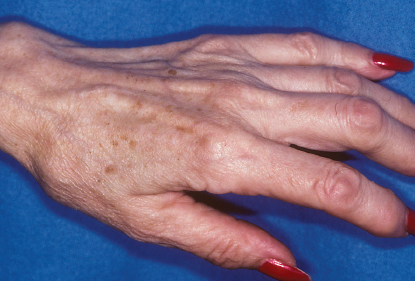
The intermetacarpal spaces deepen, especially between the thumb and the index finger, and there is some loss of intrinsic muscle volume. As the fullness of the hand is lost, the fingers and joints may appear enlarged and arthritic.
The objective of hand rejuvenation with Coleman fat grafting is to restore a youthful fullness to the back of the hand by placing a thin layer of fullness in the subdermal plane and, over time, creating a thickening of the skin.
The simple, reliable technique of autologous structural fat grafting can be used to achieve long-lasting rejuvenation of the dorsum of the hand. With this approach, restoring a slight fullness to atrophic subcutaneous tissue and thickening of the skin rejuvenates the dorsal hand; this also softens the color, masks the exposed extensor tendons and veins, and supports the aging skin.
Anatomic Considerations
The potential for damage to underlying structures is minimal so long as only a type I cannula (the bluntest) is used at all times. With purposeful placement in the subdermal layer between the veins and skin, few anatomic structures are exposed to trauma. Even the trauma to the veins is so minimal with this technique that I have only rarely seen significant bruising after structural fat grafting to the dorsum of the hand. The main potential anatomic problems can be created by the manipulation of fat after placement. Strong digital pressure on a clump of fat might push the newly grafted tissue deep to the tendons or even deeper into the intrinsic muscles of the hand (see Complications).
The key to structural fat grafting of the dorsum of the hand is purposeful placement of a smooth layer of tissue against the undersurface of the dermis, with extra placement into deficient intermetacarpal and web spaces.
Indications and Patient Selection
Typically, patients who present for fat grafting to the hand complain that their hands make them appear older than their faces would suggest. They point to the dorsum of their hands, where the veins and tendons have become more prominent, and request a fuller, more youthful look. Individuals with noticeable loss of subcutaneous fullness of the dorsal hand and apparent thinning of the skin are the best candidates for hand rejuvenation with fat grafts. These patients usually also have prominent underlying veins and tendons along with an increase in the crêpiness of the skin. Patients with intermetacarpal wasting or arthritis are also candidates for this procedure, because adjustment of the volume proportions of the hand will create a much healthier appearance by decreasing the relative size and boniness of the joints.
Material and Methods
TECHNICAL GUIDELINES
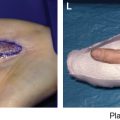
Markings

The patient’s hands are marked; borders of placement are delineated by the orange line running along the fingers and down the ulnar and radial hand, crossing the proximal forearm. Areas where more tissue will be placed are marked in green, and larger veins are marked in blue.
Anesthesia

Heavy sedation and a double-level wrist block without local infiltration are most often used for anesthesia of the hands, as was done for this patient. A solution of 1% lidocaine with 1:100,000 epinephrine is placed superficially with 25-gauge needles at two levels: one just proximal to the planned area of infiltration and another approximately 2 cm proximal to the first block. A local anesthetic is placed at the sites of planned incisions.
Incisions

Incisions are a little longer than 1 mm; they are made with a No. 11 blade in the direction of the wrinkle lines. Seven to nine incisions are spaced around the periphery and in the dorsum of the hand.
The best locations for incision placement include the following:
In the dorsal hand
At the little finger MCP joint
Web space between the ring finger and middle finger
Radial index finger
Radial thumb
Midwrist
Infiltration Cannulas
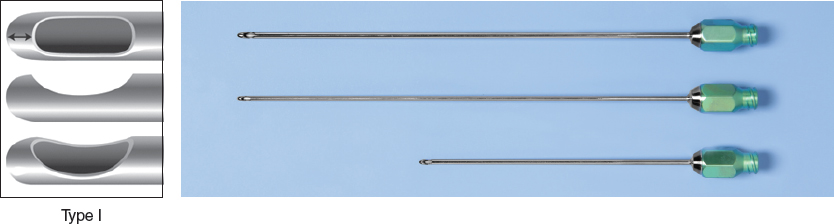
To avoid damage to underlying structures, particularly the veins, a blunt 17-gauge cannula is used for fat placement in the hand. This blunt infiltration cannula is completely capped on the tip with a lip that extends 180 degrees over a solitary distal aperture. I prefer cannulas that are 7 or 9 cm in length.
Level of Infiltration
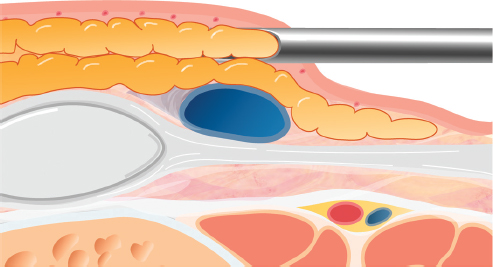
The level of placement is almost entirely in the immediate subdermal plane superficial to the veins, where it can provide support to the skin and thicken the skin.
Placement Volumes
I generally recommend placing at least 20 cc of fat in each hand, and often 30 cc or more. Additional fat will be required for patients desiring significant feathering onto the forearm or correction of intermetacarpal wasting. CAUTION: Overcorrection should be avoided unless specifically requested by the patient. I place only as much tissue as is needed to achieve a specific result based on my previous experience.
Related posts:
 Chapter 44 PERCUTANEOUS APONEUROTOMY AND LIPOFILLING AS A REGENERATIVE TREATMENT ALTERNATIVE FOR DUPUYTREN′S DISEASE
Chapter 44 PERCUTANEOUS APONEUROTOMY AND LIPOFILLING AS A REGENERATIVE TREATMENT ALTERNATIVE FOR DUPUYTREN′S DISEASE
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


