CHAPTER 34 Lymphatic Grafts
KEY POINTS
It has been shown experimentally in different groups that autologous lymphatic vessels are best suited for use as grafts.
One prerequisite for the use of these techniques is an isolated area of injury to the lymphatic transport system that is amenable to bypass from distal to proximal or peripheral to central with the use of a graft.
Reconstruction should be performed as soon as the source of lymphedema is identified.
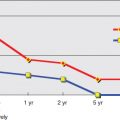
Different follow-up approaches have been used, such as volume measurements, nuclear medicine follow-up studies, and quality of life.
Lymphatic grafting for a patient with a locally interrupted lymphatic vascular system is a direct interventional procedure, with the main lymphatic collector grafts showing long-term patency.
The use of grafts is common in the field of vascular surgery as well as in plastic surgery. In vascular surgery, the bypassing of a regional vascular blockage with the use of vascular grafts is a basic principle with a long tradition, and it allows for the restoration of normal flow. As a result of the pathophysiology of lymphedema, the use of this technique is often indicated in patients with this condition.
In Europe and the United States, most cases of lymphedema are the result of local damage to the lymph transport system, whereas globally filariasis-related lymphedemas are the most frequent ones. During the course of oncologic surgical procedures (especially those involving mammary carcinomas after the removal of lymph nodes in the axilla), diminished lymphatic transport may result, and lymphedema may develop. In addition, lymphedema may occur after surgical procedures in the pelvic and inguinal regions that involve the removal of lymph nodes. Severe trauma or surgery that interferes with “bottleneck” areas of the lymphatic transport system may be the cause of lymphedema distal to the area of destruction. There is also a specific group of patients with primary lymphedema who have locally deficient lymphatic systems in the inguinal and pelvic regions but normal peripheral lymph vessels.
All of these local blockages may be overcome with the use of a vascular bypass procedure. It has been shown experimentally in different groups that autologous lymphatic vessels are best suited for use as grafts.
Graft Harvesting
According to Kubik’s anatomic description, the ventromedial bundle at the inner aspect of the thigh contains up to 16 lymphatic collectors (Fig. 34-1). These spread out and form a network between the two critical lymphatic bottleneck regions of the lower extremity: the knee and the inguinal region.
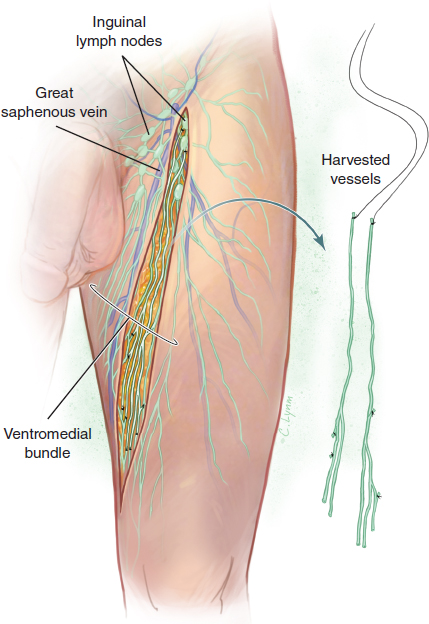
In this area of the medial thigh, lymphatic vessels can be taken out without touching the bottleneck areas for a length of up to approximately 30 cm. To ensure undisturbed lymphatic flow after the removal of the grafts, several specific steps should be taken:
The leg should be free of any preexisting lymphatic disturbances, and preoperative lymphoscintigraphy should confirm this.
During surgery, patent blue V dye is administered subdermally into the first and second web spaces. No sign of dermal backflow should be seen.
The lymphatic vessels will become stained after about 15 minutes.
Stained lymphatic collectors should always be left in place and untouched during the preparation of the grafts, with only two to three collectors taken and the rest left undisturbed.
Lymphatic collectors often show distal branching. Therefore, when using two or three main collectors as grafts, several branches can also be incorporated so that a higher number of peripheral anastomoses can be performed.
The open central ends of the transected vessels distal to the harvested grafts are carefully occluded with either sutures or coagulation to avoid leakage. The grafts can then be used in two different ways: they can be left attached to the inguinal nodes proximally and then “pedicled” to the scrotum or the opposite leg to treat penoscrotal and lower extremity lymphedema, or they can be used as free grafts for the treatment of the upper extremity. When the collectors are to be used as pedicled grafts, they are harvested, occluding them at the distal ends with long sutures; these sutures are used to pull the grafts to the penis, the scrotum, or the opposite leg. After anastomosing, the distal end is then ready for the influx of lymph from the edematous area, and the lymph will then flow in the correct direction back toward the inguinal nodes in the leg from which the collectors were harvested.
Alternatively, the lymphatic collectors can be used as free grafts for the treatment of lymphedema of the upper extremity. For free grafting, the lymphatic vessels are transected distally. Centrally they are occluded with a suture with long threads. Once again, the sutures are used to pull the grafts into the desired position.
Grafting to Bypass an Axillary Blockage
A graft procedure to bypass an axillary blockage is performed with the patient under general anesthesia. The patient’s arm is abducted, his or her neck is somewhat stretched, and the head is turned toward the opposite side (Fig. 34-2).
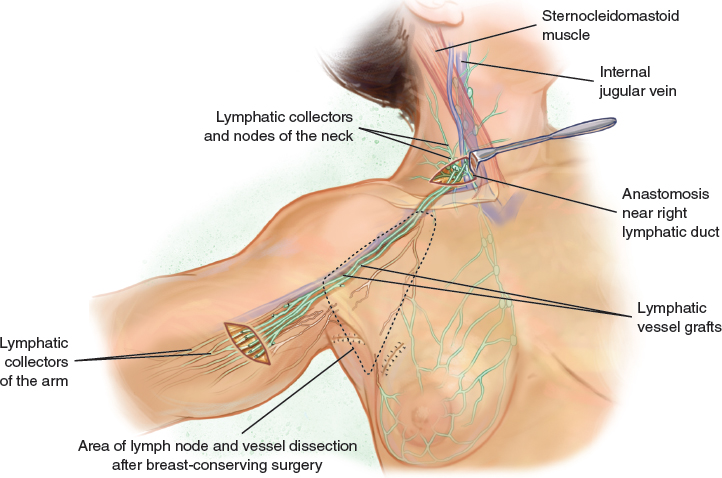
An oblique incision is created in the upper arm distal to the axilla. Because dye would be ineffectively transported within the edematous area and only a definitive area has to be checked, no staining is necessary. The biggest collectors are found above the fascia; they are gray and shiny. Care must be taken to distinguish lymphatic vessels from small veins, nerves, and fibrous cords. In a patient with long-standing lymphedema, the lymphatic vessels often have a thickened wall; however, they do not have oblique stripes like nerves do. The final decision about the quality of the vessel can only be made after transection. The lumen has to be demonstrable, and it should not contain any blood.
A second incision is then created about 3 cm above the clavicle at the lateral border of the sternocleidomastoid muscle. The muscle is shifted medially, and the fatty tissue underneath is inspected toward the internal jugular vein. To facilitate the search for the tiny lymphatic vessels, a small amount of patent blue vital dye may be injected subdermally behind the patient’s ear before the incision is made.
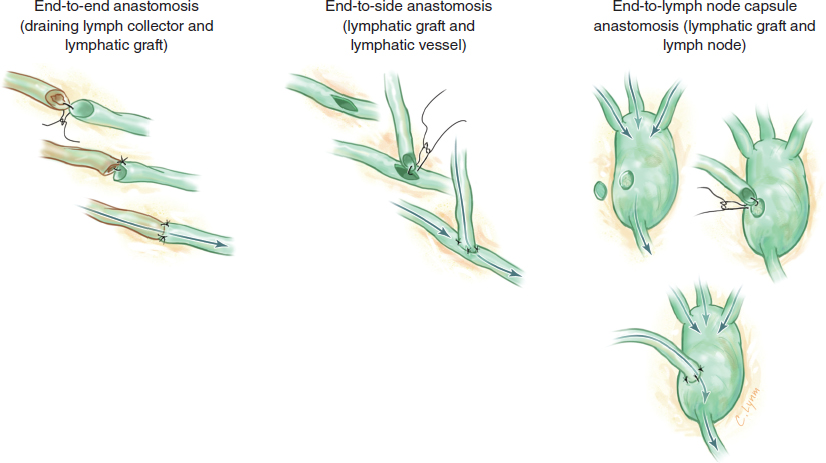
Small lymph nodes can also be found within the fatty tissue beneath the sternocleidomastoid muscle. Sometimes it is easier to connect the grafts to the lymph nodes rather than performing end-to-end or end-to-side anastomoses of the small, fragile lymphatic vessels.
Between the incisions in the upper arm and the neck, a blunt tunnel is created, and an 18 Fr catheter is inserted. A suture is incorporated within the catheter to allow the grafts to be pulled through the tube. To avoid friction, the catheter is filled with Ringer’s lactate solution. After the grafts are pulled through, the cervical end is secured, and the catheter is removed distally. Attention is paid to both incisions. It is important to ensure that the length of the graft is sufficient for a tension-free anastomosis. Tension-free anastomosing means that no tension is applied to the vessel wall in the transverse direction; the fragile wall would be disrupted. Therefore the vessel is not turned, such as in the Cobbett technique. Of course, there should be no tension on the vessels in the longitudinal direction, but this is also clear in the anastomoses of other vessels.
In the upper arm, end-to-end anastomoses are performed using a tension-free anastomosing technique. The first single stitch is placed opposite to the microsurgeon’s position. Subsequent sutures are started at the back wall. For small vessels, as few as three sutures may be sufficient; otherwise, sutures are inserted as necessary (Fig. 34-3).
All of the sutures used are single stitches. Histologic findings in experimental studies have shown only minimal foreign body reactions around tiny vessels with absorbable sutures; this is in contrast with the significant foreign body reactions caused by nonabsorbable suture material. For this reason, only the smallest 10-0 absorbable polyglactin 910 suture is currently used.
Although the nicely stained lymphatic vessels at the thigh can be harvested without magnification, the anastomosing procedure requires the highest magnification possible under the operating microscope. Searching for appropriate lymphatic vessels and discriminating among similar structures such as small nerves also requires magnification; however, medium-range magnification is often sufficient for these purposes.
Related posts:
 CHAPTER 30 Pharmacologic Treatment of Lymphedema
CHAPTER 30 Pharmacologic Treatment of Lymphedema
 CHAPTER 29 Conservative Treatments for Lymphedema
CHAPTER 29 Conservative Treatments for Lymphedema
 CHAPTER 35 Lymphaticovenular Anastomosis
CHAPTER 35 Lymphaticovenular Anastomosis
 CHAPTER 39 Transverse Myocutaneous Gracilis With Vascularized Lymph Node Transfer
CHAPTER 39 Transverse Myocutaneous Gracilis With Vascularized Lymph Node Transfer
 CHAPTER 37 Reverse Lymphatic Mapping
CHAPTER 37 Reverse Lymphatic Mapping
 CHAPTER 43 Lymphedema Complications and Their Treatment
CHAPTER 43 Lymphedema Complications and Their Treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


