CHAPTER 32 Liposuction
KEY POINTS
Liposuction for lymphedema is indicated when pitting is absent or minimal.
If significant pitting (greater than 8 to10 mm) is present, conservative treatment (combined physical therapy) is indicated to remove the lymph and transfer the lymphedema to a nonpitting state.
This nonpitting state indicates that any remaining excess volume consists of lymphedema-induced adipose tissue.
In these patients, further reduction of the excess volume is not possible with conservative treatment or microsurgical reconstructions; only liposuction can remove this excess volume.
As with conservative treatment, the lifelong 24-hour-a-day use of compression garments is essential to maintain the effects of treatment.
Excess volume without pitting means that the adipose tissue is responsible for the swelling.
Some controversy surrounds the use of liposuction to treat late-stage lymphedemas. Although conservative therapies, such as complex decongestive therapy and controlled compression therapy, should clearly be used initially, the treatment options for late-stage lymphedema that does not respond to therapy are not so clear. Moreover, various microsurgical procedures are often performed without the knowledge of adipose tissue deposition, which cannot be removed with these techniques. In contrast to microsurgical procedures, liposuction enables the complete removal of the deposited adipose tissue, leading to complete reduction in late-stage lymphedemas.
Chronic Lymphedema Leading to Adipose Tissue Deposition
Several possible explanations for adipose tissue hypertrophy in lymphedema have been postulated. One possibility is the physiologic imbalance of blood flow and lymphatic drainage, which results in the impaired clearance of lipids and their uptake by macrophages. 1 – 3 However, support is increasing for the idea that the fat cell is an endocrine organ and a cytokine-activated cell 4 , 5 and that chronic inflammation plays a role. 1 , 6 , 7 Harvey et al 8 and Schneider et al 9 discussed the relationship between slow lymph flow and adiposity and structural changes in the lymphatic system and adiposity.
Other indications for adipose tissue hypertrophy include the following 1 :
The discovery of increased adipose tissue in intestinal segments in patients with inflammatory bowel disease (Crohn’s disease), known as fat wrapping, has clearly demonstrated that inflammation has a key role. 6 , 10 , 11
Consecutive analyses of the content of the aspirate that was removed under bloodless conditions with a tourniquet had a high content of adipose tissue (mean 90%). 12
In Graves’ ophthalmopathy with exophthalmos, adipocyte-related immediate early genes are overexpressed, and cysteine-rich, angiogenic inducer 61 may have a role in both orbital inflammation and adipogenesis. 13
Tonometry can distinguish if a lymphedematous arm is harder or softer than the normal arm. Patients who have a harder arm compared with the healthy arm have excess adipose tissue. 14
Volume-rendered computer tomography in eight patients also showed a significant preoperative increase of 81% in adipose tissue in the swollen arm. This was followed by normalization at 3 months, which paralleled the complete reduction of the excess volume. 15 , 16
Analyses with dual-energy x-ray absorptiometry in 18 women with postmastectomy arm lymphedema showed a significant increase in adipose tissue in the nonpitting swollen arm before surgery. Postoperative analyses showed normalization at 3 months. This effect was also seen at 12 months. These results paralleled the complete reduction of the excess volume (edema volume). 17
A functional inactivation of a single allele of the homeobox gene Prox1 led to adult-onset obesity in mice resulting from abnormal lymph leakage from mispatterned and ruptured lymphatic vessels. 8
Parathyroid hormone–like hormone can inhibit adipogenesis and is downregulated in both active and chronic ophthalmopathy. This indicates the possibility of an increased risk of adipogenesis. 18
Adipogenesis in response to lymphatic fluid stasis is associated with a marked mononuclear cell inflammatory response. 19
Lymphatic fluid stasis potently upregulates the expression of fat differentiation markers both spatially and temporally. 20
Clinicians often think that the swelling of a lymphedematous extremity results only from an accumulation of lymph fluid, which can be removed with noninvasive conservative regimens, such as complete decongestive therapy and controlled compression therapy. 1 These therapies are efficacious if the excess swelling is in fact accumulated lymph, but they do not work if the excess volume is dominated by adipose tissue. 21 The same may apply to microsurgical procedures employing lymphovenous shunts, transplantation of lymph vessels, and transfer of lymph nodes, 22 – 26 which do not remove adipose tissue.
Preoperative Assessment
VOLUME MEASUREMENTS
The volumes of both extremities are always measured at each visit with water plethysmography, and the difference in volumes is designated as the excess volume. 21 , 27 , 28
VENOUS COLOR DOPPLER
Venous color Doppler examination is used to rule out any venous insufficiency, which can influence leg swelling.
LYMPHOSCINTIGRAPHY
Lymphoscintigraphy provides good information not only on the anatomy, but also on the lymphatic function (transport). I use it mostly in patients with primary lymphedema and those with leg swelling of unknown origin, such as when lipedema is suspected. 29
CT AND MRI
CT and MRI can detect enlarged lymph nodes and can show excess fat and edema. These modes can also be used to examine enlarged lymph nodes when primary or secondary malignancy is suspected.
INDICATIONS FOR LIPOSUCTION
A surgical approach to remove the hypertrophied adipose tissue is appropriate when excess volume has not been achieved by conservative treatment and the patient has subjective discomfort from a heavy arm or leg. 1
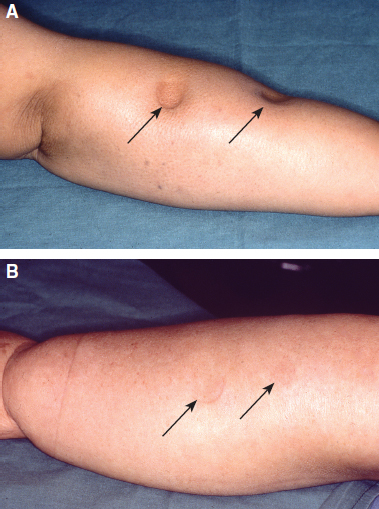
Liposuction should never be performed in a patient with a pitting edema, because it is dominated by accumulated lymph, which can be removed by conservative treatment. 1 The primary and most significant goal is to transform a pitting edema into a nonpitting edema with conservative regimens such as complete decongestive therapy or controlled compression therapy. Pitting can be defined as a depression that is formed after pressure is exerted on the edematous tissue by the fingertip, which results in the squeezing of lymph into the surrounding tissue (Fig. 32-1, A). To standardize the pitting test, the surgeon presses as hard as possible with the thumb for 1 minute on the region under investigation. The amount of depression is estimated in millimeters. Swelling that is dominated by hypertrophied adipose tissue shows little or no pitting 28 (Fig. 32-1, B).
Approximately 4 to 5 mm of pitting in arm lymphedema and 6 to 8 mm of pitting in leg lymphedema are acceptable. Liposuction should not be done if pitting edema is present. This is because liposuction removes fat and not fluid, regardless if it theoretically could remove all of the accumulated fluid in a pitting lymphedema without excess adipose tissue formation. 1 Liposuction also improves patients’ quality of life 21 , 30 and reduces the incidence of erysipelas. 31
Related posts:
 CHAPTER 30 Pharmacologic Treatment of Lymphedema
CHAPTER 30 Pharmacologic Treatment of Lymphedema
 CHAPTER 29 Conservative Treatments for Lymphedema
CHAPTER 29 Conservative Treatments for Lymphedema
 CHAPTER 35 Lymphaticovenular Anastomosis
CHAPTER 35 Lymphaticovenular Anastomosis
 CHAPTER 39 Transverse Myocutaneous Gracilis With Vascularized Lymph Node Transfer
CHAPTER 39 Transverse Myocutaneous Gracilis With Vascularized Lymph Node Transfer
 CHAPTER 37 Reverse Lymphatic Mapping
CHAPTER 37 Reverse Lymphatic Mapping
 CHAPTER 43 Lymphedema Complications and Their Treatment
CHAPTER 43 Lymphedema Complications and Their Treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


