Chapter 29 STRUCTURAL FAT GRAFTING IN THE NECK
A full, taut neck is one of the signs of youth and beauty. Even though deep transverse cervical creases may be present in youth, deep horizontal folds in the neck are usually considered undesirable at any age. With age the cervical subdermal fullness disappears and the skin texture gradually deteriorates, leaving behind unsupported, crepey skin. When structural fullness is added to the neck, it provides underlying support to the skin to restore a more youthful fullness. Recontouring of the neck with structural fat can provide further enhancement by disguising prominent neck cartilages.
Aesthetic Considerations

Photographs of the patient at a younger age are almost always revealing. In these photographs, the transverse cervical crease is present in the younger photo, but as the woman aged, this became more prominent and could be accentuated by a facelift.
Anatomic Considerations
In the neck the potential for damage to underlying structures is minimal if only a Coleman type I cannula (the most blunt) is used at all times. With purposeful placement in the subdermal layer between the platysma and skin, few anatomic structures are exposed to trauma. The trauma to even the veins is so minimal using this technique that I have rarely seen dramatic bruising after structural fat grafting to the isolated neck. As in the hands, the primary potential anatomic problems can be created by manipulation of fat after placement. Strong digital pressure on a lump of fat might push the newly grafted tissue deep to the platysma.
The key to structural fat grafting of the dorsum of the neck, as in the hands, is purposeful placement of a smooth layer of tissue against the undersurface of the dermis. Placement of much more under the neck creases will help to diminish them also. In persons with prominent neck cartilages, extra placement around the neck cartilages to soften the Adam’s apple may be appropriate.
Indications and Patient Selection
Typically, patients who present for fat grafting of the neck have complaints similar to patients who request hand rejuvenation. They complain that their necks make them appear older than their faces would suggest. Individuals with noticeable loss of subcutaneous fullness of the neck and apparent crêpiness and thinning of the skin are the best candidates for neck rejuvenation with fat grafts. Unfortunately, the change that occurs with restoring structure to the supporting matrix of the neck is not as dramatic as in the face or even the hands, and the patient should not expect dramatic changes—only subtle improvement in texture and contours.
Many patients are bothered by prominent neck cartilages, either as a result of aging or because they feel that their Adam’s apple makes them look too masculine, even at a younger age. These patients usually seek softening of the prominent cartilages with three-dimensional volume placement around the cartilages. Another indication in younger patients is deep transverse neck creases.

This 48-year-old woman presented for augmentation of her lip. She was also interested in correcting her jawline and neck, especially the creases of her neck.
In comparing her youthful photographs to recent ones, the transverse neck creases clearly visible in both old photos have deepened with age and are interrupted by the inferior extensions of vertical platysma bands. In addition, there has been a remarkable diminution in the size of her lower lip, much more than in her upper lip.
MARKINGS

This patient’s neck was marked with borders of placement as delineated by the yellow marks. The places where I planned to place more tissue, such as lateral to the neck cartilages, were marked in green, and the incision sites in red.
The neck should be approached in a similar fashion to the dorsum of the hand: primarily with placement of a diffuse thin layer of tissue immediately subdermal over the entire surface to be treated. Like the hand, specific deficiencies or depressions should be treated differently, with a thicker placement. These are usually deep horizontal neck creases and depressions caused by particularly obvious neck cartilages.
Material and Methods
TECHNICAL GUIDELINES
Anesthesia
A solution of 0.5% lidocaine with 1:200,000 epinephrine of infiltration is placed with a type I cannula. I also use intravenous sedation administered by an anesthesiologist. The infiltration is performed at a ratio of about ½ cc of local anesthetic for every 1 cc of fat to be placed.
Incisions
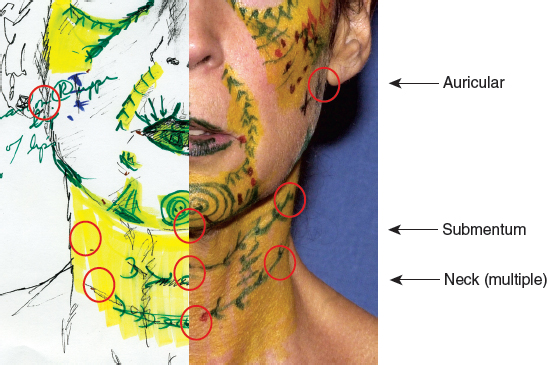
Primary access to the neck is from incisions made in the neck creases. They are usually in the midline and over the area of the sternocleidomastoid muscle. Because I try to place tissue from several different directions, access to the upper neck from a different direction can be obtained by the mandibular and auricular incisions commonly used in jawline placement.
Infiltration Cannulas
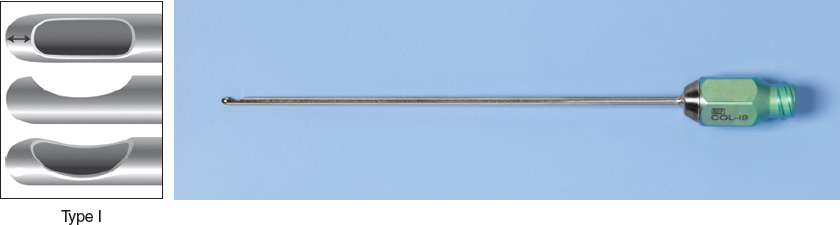
A blunt 17-gauge Coleman type I cannula is used for placement to avoid damage to underlying structures, particularly the neck veins. This blunt infiltration cannula is completely capped on the tip with a lip that extends 180 degrees over a solitary distal aperture. For fat placement into the neck I use both straight and curved cannulas that are 7 or 9 cm long with a 17-gauge lumen.
Related posts:
 Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
 Chapter 27 STRUCTURAL FAT GRAFTING IN THE LIPS
Chapter 27 STRUCTURAL FAT GRAFTING IN THE LIPS
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
 Chapter 26 STRUCTURAL FAT GRAFTING IN THE NASOLABIAL FOLD
Chapter 26 STRUCTURAL FAT GRAFTING IN THE NASOLABIAL FOLD
 Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
 Chapter 24 STRUCTURAL FAT GRAFTING IN THE SUPRAORBITAL AREA
Chapter 24 STRUCTURAL FAT GRAFTING IN THE SUPRAORBITAL AREA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


