Chapter 24 STRUCTURAL FAT GRAFTING IN THE SUPRAORBITAL AREA
The aesthetics of the upper third of the face have been poorly understood in modern plastic surgery. A definite fullness of the supraorbital region is essential for a sensual, healthy appearance, yet plastic surgeons have historically ignored the need to restore fullness to achieve the most natural, aesthetic result. Likewise, skeletonization of the upper eyelid, brow, and temple projects sickness and starvation, yet surgeons have focused their “rejuvenation” procedures on removing and tightening in the upper face rather than filling.
Unlike the brow and temples, the frontal region is difficult to rejuvenate with structural fat grafting. Usually the primary problem with the aging forehead is not a contour deformity but the action of the frontalis muscle as it becomes less and less opposed by the diffuse fullness of youth. This results in wrinkles or creases that are created by intrinsic tone of the frontalis and other muscles. With great care, placing a volume of tissue subcutaneously and into the muscle can give a reasonably smooth result when the patient does not move his forehead. However, on motion, the frontalis muscle can create even more creases than were originally present. For that reason I have reduced structural fat grafting of the frontalis region to noticeable frontal deficiencies and deep wrinkles. The deeper wrinkles are approached with combination therapies, including Botox, intradermal injection, V-dissection, and subcision.
Aesthetic Considerations
Fullness characterizes the young brow, cheek, and temple. Young eyebrows have so much fullness beneath them that there is always a distance between the shadow of the supraorbital fold and the eyebrow itself. The intrinsic nature of the brow is that it is inherently more taut than the eyelid skin. The brow fullness expands the skin immediately caudal to the eyebrow, producing a turgidity that extends for a few millimeters cephalad to the supratarsal fold where the skin becomes flaccid. There is at least a hint of loose skin above the supratarsal fold, even in teenagers. 1 – 4
The amount of upper eyelid visible under the brow can be variable in youth; the most frequent presentations are of the skin touching the eyelashes (with no eyelid visible) or with only a millimeter or two of palpebral show. A young, healthy person can occasionally present with deep-set eyes, but rarely with hollow eyes.
The eyebrow is supported laterally by temporal fullness. It is that temporal fullness that allows one to see the lateral quarter of the eyebrow in a youthful face and that supports the eyebrow into its lateral arch. The temporal fullness and lateral frontal fullness also produce the smooth, strong brow essential to a youthful appearance.
Indications and Patient Selection

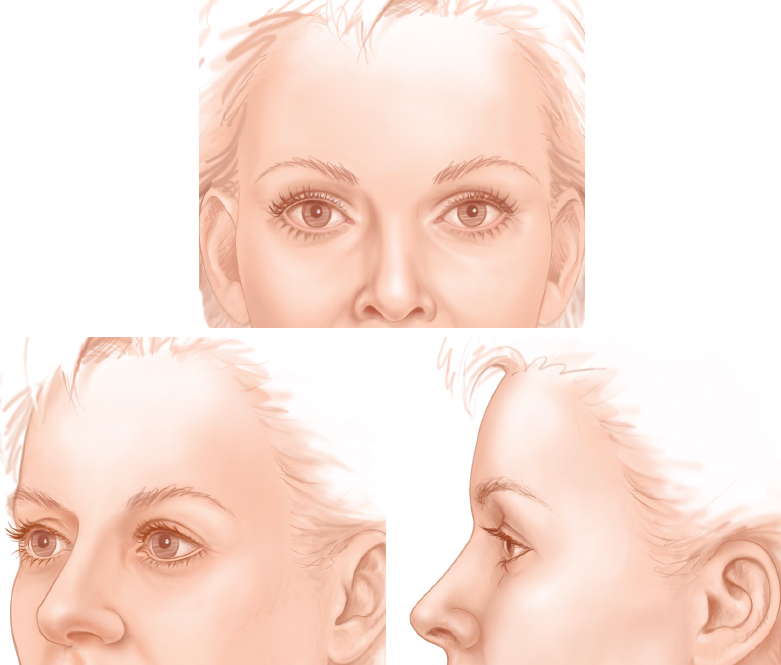
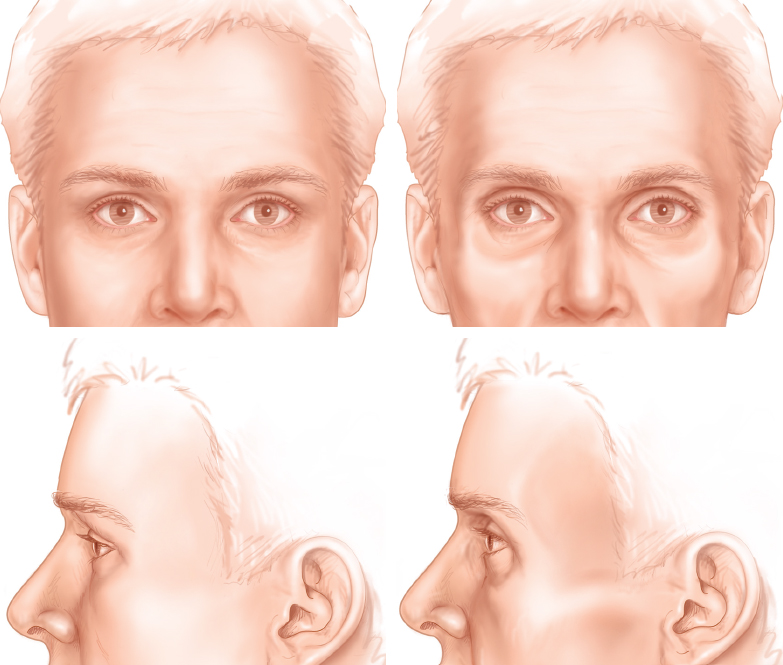
When I returned to Texas to visit my grandmother, Mary Coleman, during my plastic surgery residency, I was struck by how much she looked like one of the patients that I had just recently seen with a history of three upper blepharoplasties. My grandmother never had any facial surgery; she was just simply old. Her photos at 30 years of age and at 99 years demonstrate the aging changes that had taken place over the years.
When I returned to my residency after visiting my grandmother in 1982, the AIDS epidemic had filled San Francisco General Hospital with 20-year-olds with hollow eyes and temples. They had lost their periorbital fullness because they were terminally ill. It was at that point that it became obvious to me that excisional aesthetic procedures of the upper third of the face skeletonize the periorbital region in an unhealthy manner. I began to realize that procedures that skeletonize the upper third of the face make patients appear sick, anorexic, or old.
RESTORATION OF HEALTHY PROPORTIONS
As discussed in Chapter 22, loss of subcutaneous fat or fullness commonly seen with iatrogenic deformities after surgery, with acne, and most recently with lipoatrophy are primary indications for structural fat grafting.
Just as the fullness of youth projects health, the absence of fullness warns the observer of sickness, age, or starvation. The upper eyelid/brow area is one of the first areas to project deteriorating health. Just 1 or 2 mm of hollowness at the upper eyelids and temples can have a dramatic impact on how well a person looks.
In healthy individuals, surgical removal of fat from the upper eyelids or from any part of the face can create the appearance of sickness. Likewise, acne scarring in the temple and glabella can accelerate atrophy of the involved areas and create bizarre proportions. Drug-related lipoatrophy can affect not only the midface, but also the upper face, temples, and upper eyelids.
Skeletal abnormalities of the frontal, parietal, and temporal regions can give a face an unattractive or even unnatural appearance. Significant temporal and lateral frontal deficiencies will make the central parietal or lower frontal skull unattractively prominent. However, the solutions to these problems in plastic surgery have been prohibitively risky: craniofacial procedures or alloplastic implants. Structural fat grafting to the temporal and lateral frontal region (and many other deficient areas) is a safe, predictable way to approach these sometimes difficult problems.
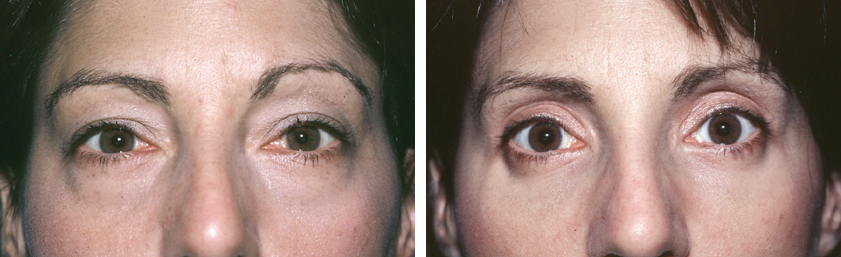
When hanging skin is a component of supraorbital aging, it may need to be excised. However, I rarely see an indication for excising muscle or fat from the upper eyelids. This was done in this patient, seen preoperatively and 7 years after excision of skin, muscle, and fat from her upper eyelids. Although many surgeons think their patients want such a look, this is removing the signs of aging without rejuvenating.
Excision of muscles such as the corrugators, the procerus, and especially the orbicularis oculi needs to be carefully considered in view of the reduction of the underlying supportive tissue and thereby their contribution to the atrophic process of aging.
On the other hand, excision of the eyelid skin alone approaches the radial vector by making the ratio between the overlying skin and the underlying structures more closely approximate the youthful proportions that exist between the two areas. Excising muscle and fat from the underlying structures, on the other hand, always skeletonizes the area.
Adding to the supraorbital region is an extremely complex maneuver, and the biomechanics of this region are poorly understood. Restoring the volume of the forehead or merely adding to the brow itself creates a radial vector with a strong mechanical advantage that elevates the eyelid skin.
The importance of the concept of radial vectors has yet to be recognized for the forehead. By adding tissue over a large surface area to the forehead, one can have a remarkable effect on the brow and upper eyelid: a “lifting” without excision. The traditional elevation of the brow by excising skin or scalp creates a vector in a superior or superolateral direction. This moves tissues away from the orbit, and thereby reduces some of the excess skin or crêpiness of the area. However, a forehead lift of any type can elevate the brow in an often-unattractive fashion and can skeletonize the upper orbit. It does not create the soft, full eyelid of youth. Structural fat grafting provides a tool that finally allows the recreation of a youthful upper eyelid by filling the forehead, brow, and upper eyelids to replace the missing underlying structures.
The filling and supporting of the periorbital region along with judicious skin care to maintain elasticity are the primary tools for maintaining a youthful appearance of the eyes. Excisional and suspensory surgeries should be secondary procedures to be executed after the primary maneuvers are no longer sufficient.
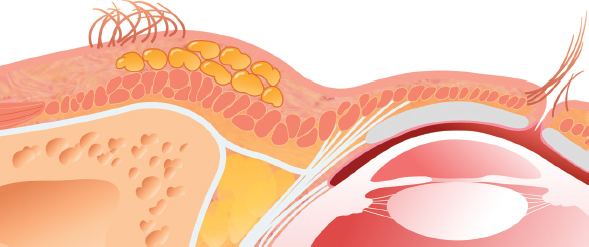
Anatomic Considerations
A thorough knowledge of the anatomy of the upper eyelids, brow, and temple is essential for the surgeon operating on the upper third of the face. Preventing injury to nerves and avoiding inadvertent cannulation of arteries or veins are primary concerns.
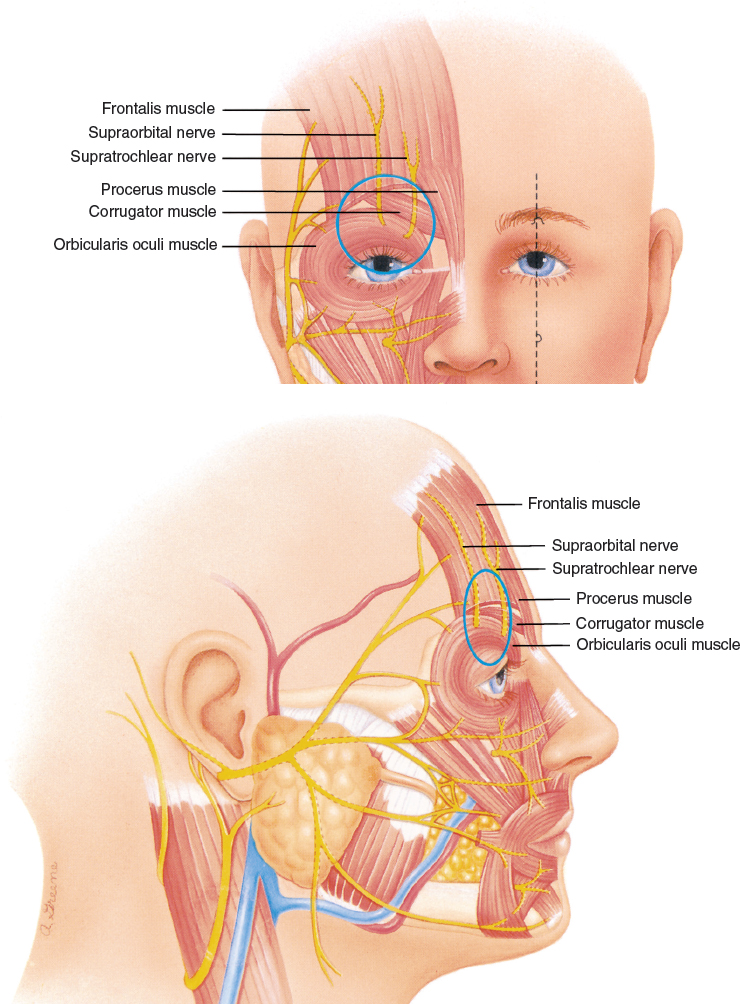
Around the supraorbital foramen, the surgeon should use blunter cannulas to avoid injury to the supraorbital and supratrochlear nerves or cannulation of the vessels. I use a Coleman type I cannula when placing tissue next to the bone in this area, although it has become my common practice to place tissue in a more superficial plane when I am near the supraorbital rim.
However, acne scarring and other types of adherent scars are frequently present in the central forehead, brow, and especially the glabella. Freeing up more deeply adherent scars can damage the supraorbital or supratrochlear nerves.
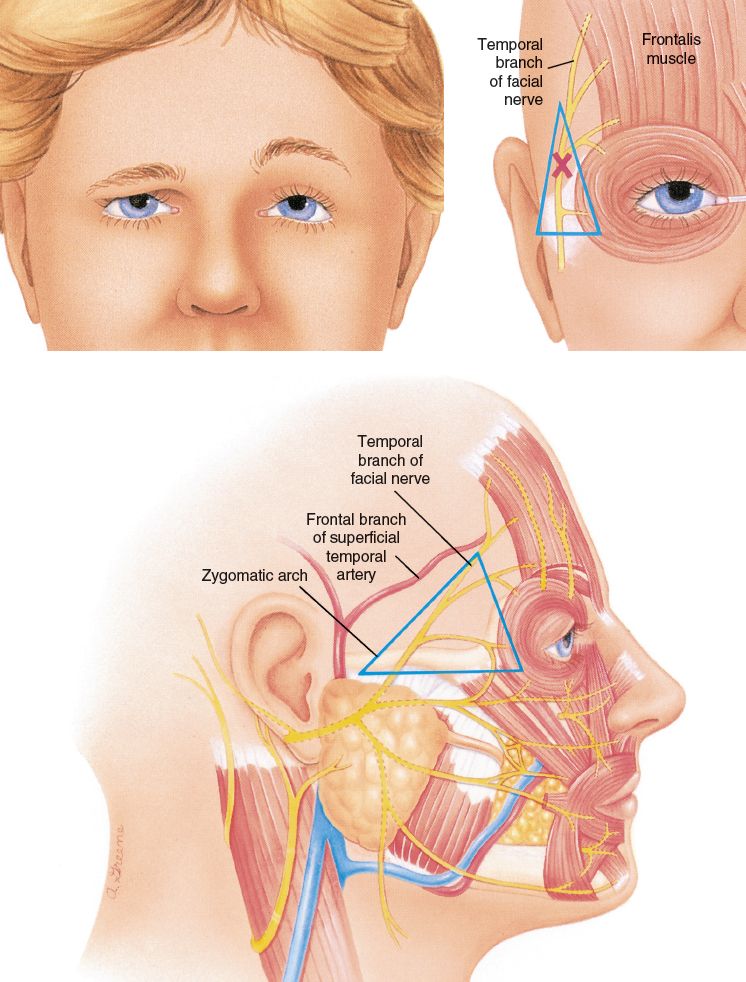
Likewise, in the area of the temporal branch of the facial nerve, the bluntest cannulas should be used for almost any placement. Paralysis of the frontalis muscle with unilateral brow ptosis and asymmetrical lack of animation of the involved forehead will result from damage to the nerve.
As in the glabella, acne scarring is frequently present in the temple; freeing up more deeply adherent scars can damage these nerves. I recommend limiting the release of such adhesions in the temple to the most superficial planes.
Injury to nerves is not the only concern in this area. The rich network of blood vessels in the temporoparietal fascia and around the eyes is easy to disrupt during infiltration of fat or even local anesthetic. In fact, the reason I switched to use of the fat infiltration cannulas for placing the local anesthetic was the high incidence of hematomas that I had with 25-gauge needles in the temple. I now use only type I cannulas for infiltration of local anesthesia in the upper face, since the use of sharper cannulas (especially a type III) will frequently result in large hematoma formation in the temple and brow.
Hematomas are not the only potential vascular phenomenon that can occur. Injecting in these areas with a sharp needle should be avoided because it could cause arterial or venous cannulation and possible embolization (see Chapter 4).
Not only does superficial placement create an aesthetically pleasing result, it eliminates the possibility of damaging the lacrimal gland and the levator mechanisms of the upper eyelids.
Material and Methods
TECHNICAL GUIDELINES
Markings
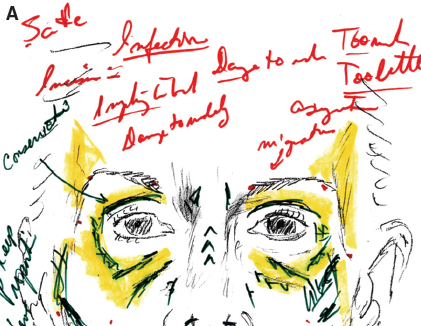
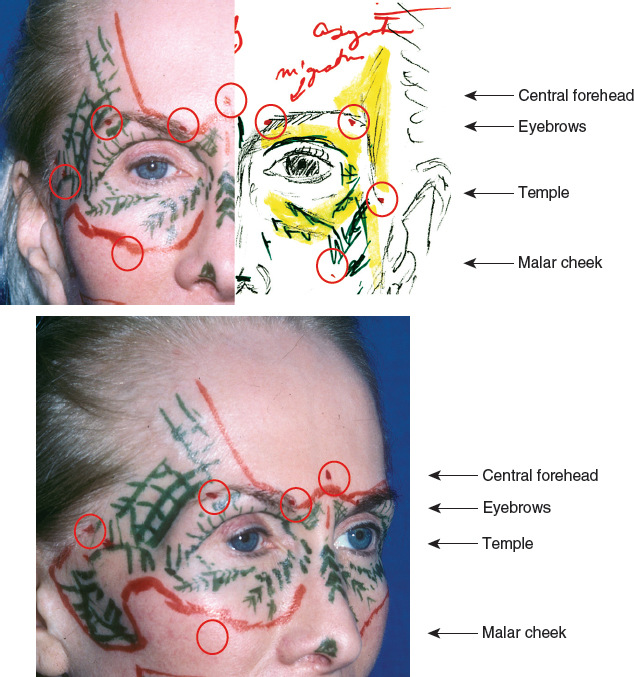
The blueprint is used not only for planning the procedure, but also to help document informed consent. Please note the re-marking in the upper part of the sheet.

The plan for correction is shown. Changes in shape to restore subtle fullness are marked in green, while feathering out to areas is marked in yellow. The planned incision sites are marked in red.
Anesthesia
A solution of 0.5% lidocaine with 1:200,000 epinephrine is infiltrated to provide anesthesia, placing the least amount that is still effective to avoid significant distortion. Local anesthesia should be placed into the periorbital region using only the bluntest style I cannula. This is done to avoid damaging structures, such as nerves and blood vessels, but also to avoid entering the lumen of an artery or vein during the injection of local anesthetic. Damaging an artery or vein that results in a hematoma during infiltration of the local anesthetic will interfere significantly with the surgeon’s ability to judge volumes and distribution of the grafted fat during placement.
The vasoconstriction caused by the infiltration of epinephrine reduces the possibility of the cannula entering an artery or vein during the placement of fat. Epinephrine should be infiltrated into the periorbital region in every case to reduce the possibility of intra-arterial injection. Even if the procedure is performed under general anesthesia, epinephrine should be infiltrated.
Incisions
I make one incision into each far lateral and medial brow, as well as the lateral inferior temple. From these incisions, the entire upper eyelids can be reached (both through the ipsilateral and contralateral incisions) as well as the temple and forehead. I often make an incision in the midline of the forehead above the glabella, especially if I plan to approach the nose or glabella.
On a rare occasion, an incision is made in the hairline of the forehead or temple for better access. This would most often be to access areas that were scarred because of previous procedures.
Infiltration Cannulas
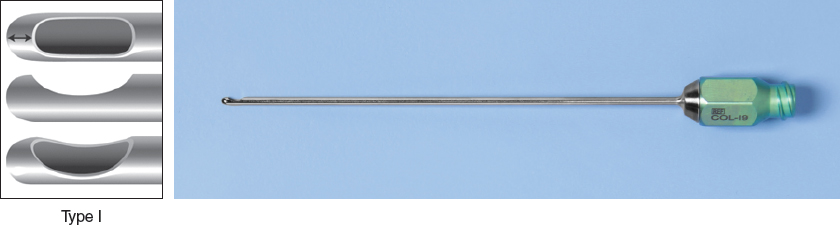
I use the mini-cannulas in the upper face. For the placement of local anesthesia, I always use a Coleman type I cannula in the 5 or 6 cm lengths in the upper face with the exception of using a Coleman mini III cannula in the upper eyelid and nose. When I approach any areas through a temple incision or when I am going to be placing tissue above the brow or in the temple, I use a type I cannula or mini I for placement.
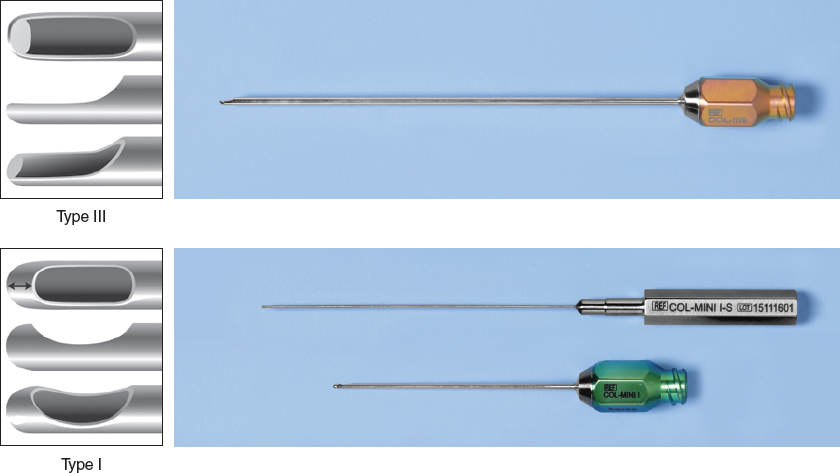
In the upper eyelids below the eyebrow and in the medial nose, I frequently use Coleman type III cannulas, because they give me better control to remain between the orbicularis oculi muscle and the skin in these areas. I can use the 3, 5, or 6 cm, depending on the situation.
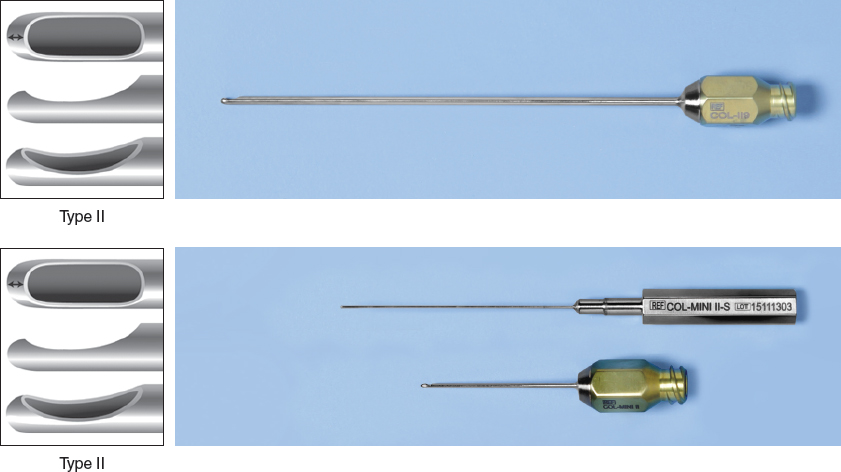
When the temple has acne scarring or scarring from previous procedures, and I find it difficult to push the cannula through the area, I will switch to a Coleman type II cannula. To follow the curvature of the bony forehead, I frequently use a slightly curved cannula of a type II variety when I am trying to place tissue close to the bone.
Level of Infiltration
Into the upper eyelids, I try to remain superficial at all times, remaining immediately subdermal or into the orbicularis oculi muscles. Into the forehead and above the brow, I primarily place tissue superficially. However, I also place a little more tissue into the frontalis muscle than I do into the orbicularis oculi.
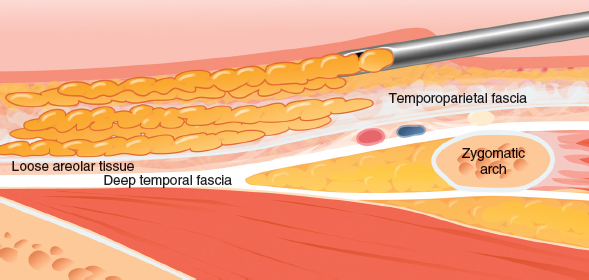
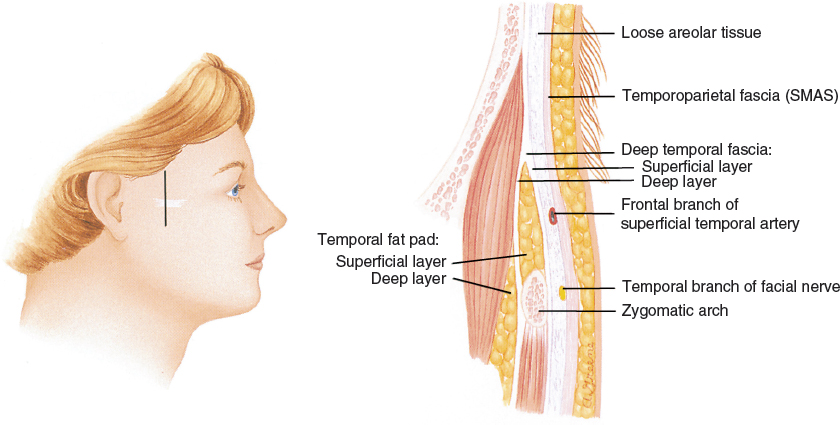
Into the temporal region, I remain in the galea (superficial parietotemporal fascia) as much as I possibly can, with some placement in the immediately subdermal plane as well.
Placement of tissue into the deeper planes is fraught with problems. It is easy to place tissue into the loose areolar plane above the periosteum; however, fat placed at this level is likely to migrate, and there is an increased possibility of irregularities.
Volume Ranges
Upper eyelids: Less than 1.5 cc of fat infiltrated into the upper eyelids on some people can make a dramatic change, especially in younger patients and men. In women more than 50 years of age, 2.5 or 3.5 cc is sometimes needed. Some patients, especially those with upper eyelids skeletonized by surgical means, may need as much as 5 cc. However, I have never placed more than 3.5 cc at one setting and will split an amount larger than that into two procedures.
Temples: Although the temples appear to be a large surface area, I find that surprisingly small amounts are sufficient to produce the subtle changes most patients desire. The usual amounts are from 3 to 7 cc. With particularly wasted temples, I will place up to 10 cc, but rarely.
Medial eyelids (lateral nose): Usually the range is from 0.4 to 0.8 cc.
Frontal forehead: Because of the possibility of irregularities from the activity of the corrugator and frontalis muscles, experience has taught me to be relatively conservative about placing anything at all into the frontal forehead. It is easy to create a circumscribed collection that is easily visible. The motion of the frontalis muscle makes fullness placed into the forehead distressingly visible with bizarre undulations with motion of the muscle. When I do place fat in this area, I keep the volumes down to between 2 cc and 7 cc for the entire forehead.
Nasion: Placing less than 1.5 cc into this area is not enough to produce a discernible change; 2 to 4 cc is a more usual amount, although sometimes atrophy in this area can warrant as much as 5 to 7 cc.
Most Likely Technical Mistakes
The most common mistakes that I have made in the upper eyelids are in areas of slight deficiency. As soon as swelling begins in the upper eyelid, determining an area of slight deficiency becomes extremely difficult. Both visual and tactile clues are difficult to ascertain when swelling is present. This is the most common reason for an additional surgery to be needed in this area.
In the forehead, the most common mistakes are irregularities, especially around the insertion of the corrugators over the mid eyebrow, where slight depressions can be seen. Even on repeated infiltrations, a depression in this area can be extremely difficult to correct. Usually the patient presents with a smooth forehead and cannot see the problem in the postoperative photographs. However, when the patient moves his or her eyebrows in any fashion, a deep depression develops in the area, which is smooth without motion. When the patient looks into the mirror, there is a tendency to contract the corrugator, so the patient thinks the problem is present all of the time.
Related posts:
 Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
 Chapter 29 STRUCTURAL FAT GRAFTING IN THE NECK
Chapter 29 STRUCTURAL FAT GRAFTING IN THE NECK
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
 Chapter 26 STRUCTURAL FAT GRAFTING IN THE NASOLABIAL FOLD
Chapter 26 STRUCTURAL FAT GRAFTING IN THE NASOLABIAL FOLD
 Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


