Chapter 26 STRUCTURAL FAT GRAFTING IN THE NASOLABIAL FOLD
Aesthetic Considerations
The nasolabial folds and marionette grooves convey powerful emotions. Deepening of the superior nasolabial fold can express anger or disgust, while deepening of the lower nasolabial fold can denote grief, sadness, or joy, depending on the angulations of the fold.

Subtle changes in the depth of a nasolabial fold can project profoundly different emotions. While vertical deepening of the nasolabial folds can project disgust, as in this woman, lateral deepening of a less vertical fold can convey feelings of distress or anguish.
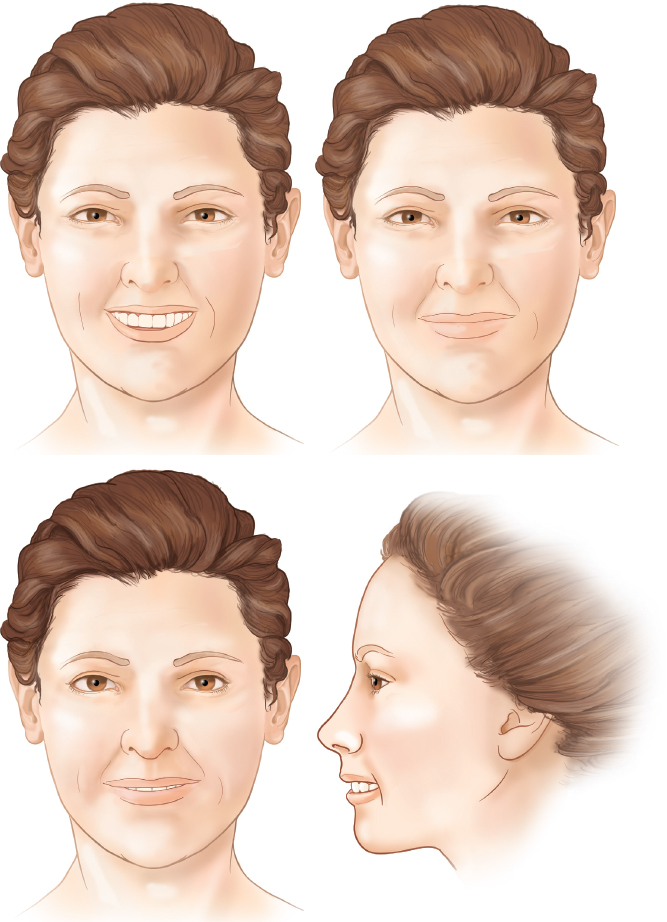
In this young man, the nasolabial fold contributes to an expression of happiness; at the top are two different levels of content, whereas the two drawings at the bottom demonstrate a forced or fake smile.
Expression of these emotions is integral to communication between humans. Likewise, the unintentional projection of emotions can be an impediment to accurate communication. When a person projects anger, sadness, or disgust even though he is feeling happy and rested, he will be misunderstood.
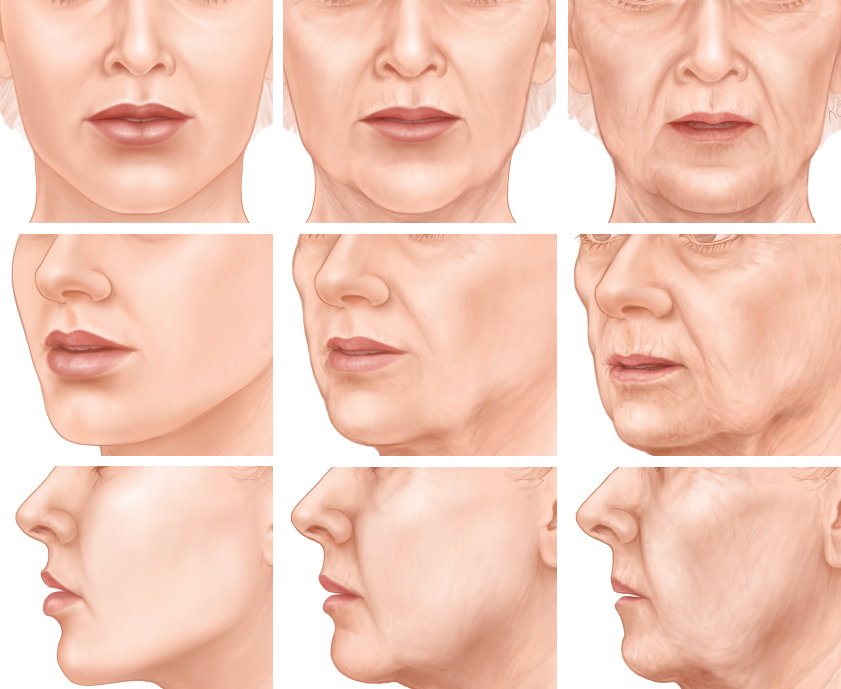
Aging can generate negative and fixed changes in facial expression. As the face ages, it loses the subcutaneous fullness associated with youth. With loss of fullness comes a weakening of the radial vectors that support and thereby tighten the skin around the mouth. As these radial vectors weaken, the now unsupported skin sinks into folds, wrinkles, creases, and even pores. One of the consistent and more obvious folds or wrinkles on the face into which the skin retreats with aging is the nasolabial fold. As these folds become more pronounced, unintentional emotional expressions can become fixed on the face. For example, when the patient is listening calmly, not intending to demonstrate any emotional reaction, the deepening nasolabial folds can convey a very different impression—perhaps that of disdain or even anger. Fortunately, this accentuation of the nasolabial fold is not always negative; the folds can also deepen into a smiling or cheerful countenance.
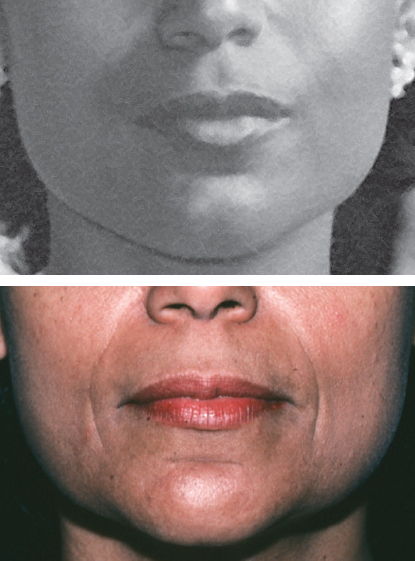
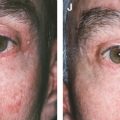
Photographs of the patient’s appearance when young are often helpful in evaluating and planning the treatment of nasolabial folds. This woman demonstrates an obvious vertical fold that extends down well past the level of the oral commissure. A bare hint of a fold can be seen in her younger photograph. It has been my experience that if a person did not have deep nasolabial folds when young, there is a good likelihood that subcutaneous fat placed directly under the fold and feathered into the surrounding area will soften the nasolabial folds back to at least the younger state. It is advisable to avoid overcorrection of the folds, because this can sometimes result in a bizarre appearance and force folds into the surrounding areas. Such overcorrections can make the patient feel that their smile has changed in a negative direction.
The use of old photographs is especially important if a patient had a significant nasolabial fold when he or she was young, and there is now a noteworthy premaxillary deficiency with a full anterior cheek. In such a person, there is little hope of ablating the nasolabial fold.
In many aging faces, the deepening nasolabial fold leaves behind a permanent sneer that can only be erased by smiling. These patients in particular are good candidates for softening of the nasolabial folds. For these individuals the primary goal of fat grafting in the nasolabial fold and marionette region is to soften these folds and thereby reduce the sneer.

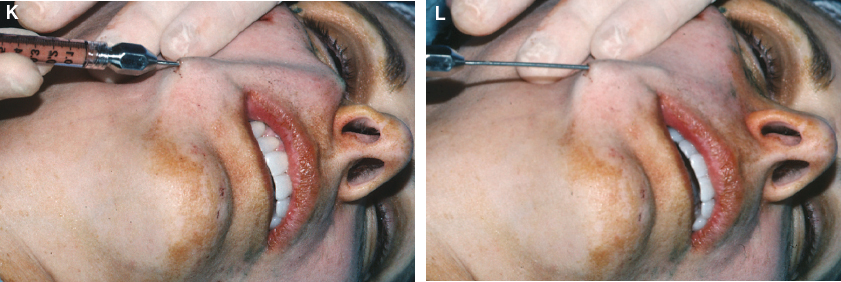
This early patient of mine was one of the cases that first underscored for me the look of disdain that the nasolabial fold can create. Although she was a pleasant lady, when she was not smiling she looked as though she had smelled something bad. Placement of only 2.8 cc into the right and 2.5 cc into the left nasolabial fold with a sharp needle helped relieve this disdainful projection. Although she demonstrated a good correction at her 3-year postoperative follow-up visit, the use of a sharp needle in this early case of mine left behind an isolated linear correction on her right nasolabial fold.
It is important to recognize that an individual’s nasolabial folds are not necessarily bad, and in some faces their elimination will be detrimental to facial harmony. The problem is not the existence of the folds but their depth and prominence and how they affect and alter facial expression.
Anatomic Considerations
The topical anatomy of the nasolabial and marionette folds can vary greatly from individual to individual. At one end of the spectrum, they are almost completely absent or flat. At the other end, there is a prominent fullness lateral to the nasolabial fold with a pronounced premaxillary deficiency. The folds and the surrounding skin should be carefully evaluated when a fat grafting procedure is contemplated.
The nasolabial folds and marionette grooves are strongly influenced by the surrounding structures in the cheeks, lips and chin. In a younger person, the nasolabial folds and marionette grooves may be manifest as deep creases surrounded by fullness. In such situations, the folds may not project any particular negative emotion despite their prominence.
Indications and Patient Selection
As discussed earlier, the primary indication for correction of the nasolabial folds and marionette grooves is aging. Older patients object to the expressions that age seems to have painted in the folds and lines of their faces; these seem to appear more prominent and objectionable with each passing year. Interestingly, younger patients who have deep nasolabial folds have a similar reaction when they perceive that their deeper than usual folds make them appear older than they are. The most important consideration with marionette grooves is to be certain that the patient understands that the grooves will most likely not disappear altogether; improvement in the texture of the marionette grooves is frequently the best improvement possible with subcutaneous placement of fatty tissue. Fat tissue transplanted into an intradermal or immediate subdermal plane may be indicated for additional blunting of both the marionette grooves and nasolabial folds. The results from intradermal injection are quite different from those of subcutaneous filling (see Chapter 1).
Material and Methods
TECHNICAL GUIDELINES
Anesthesia
When treating the nasolabial folds and marionette grooves, infraorbital and mental nerve blocks may be employed. However, I always infiltrate locally 0.5% lidocaine with 1:200,000 epinephrine from both the cheek and inferior incisions. Even if general anesthesia is used, I infiltrate epinephrine for vasoconstriction to lessen the chance of intravascular infiltration of the fat, especially if I plan to use a 22-gauge sharp needle for superficial or intradermal injection of the fat.
Incisions
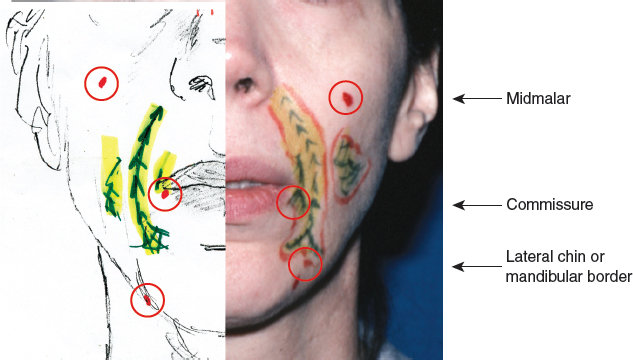
Lower midmalar incisions provide access for the perpendicular placement of tissue, and an incision in the lateral chin or mandibular border provides access for the longitudinal placement of tissue. Frequently an incision near the commissure is used for a different angle of placement.
Infiltration Cannulas

In the nasolablial fold and marionette groove areas, a Coleman type II cannula (7 or 9 cm) or mini-cannula (6 cm) is most commonly used to facilitate dissection while avoiding intravascular placement.
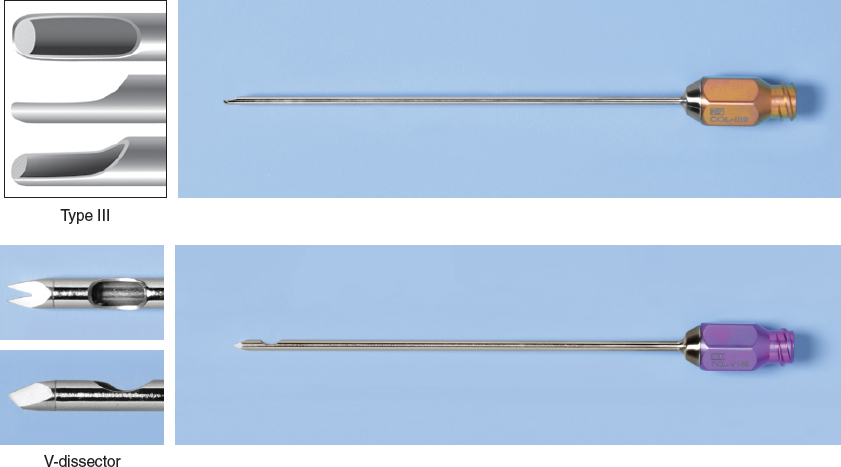
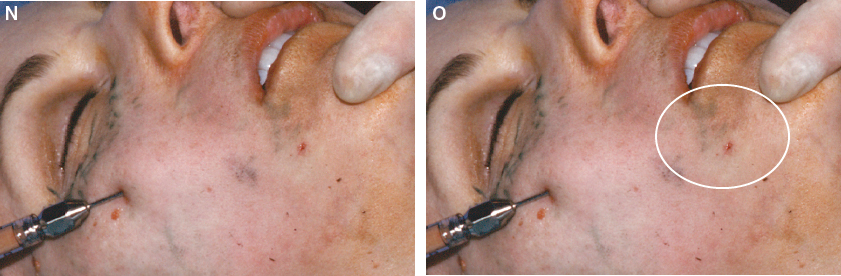
However, I use a Coleman type III cannula or type III mini-cannula in areas of very fibrous adhesions, especially against the skin. If the adhesions are particularly troublesome, a V-dissector cannula is used to disrupt the superficial connections. However, too much disruption of the subdermal connections may result in isolated linear protrusions, so I am frugal with the use of the V-dissector cannula in the nasolabial folds. My experience with sharp instruments such as needles has been disappointing: the grafted fat does not seem to be as stable, and the correction can be visible and circumscribed rather than blending in naturally with the surrounding area.
Level of Infiltration
Although some tissue is placed at every level from submucosal to subcutaneous, the primary level of placement in most cases is immediately subdermal to impart structural integrity to the cutaneous element of the fold and to encourage the improvement in the quality of the skin. In any case this superficial treatment also helps blunt the fold or line better than simply adding volume deep to the fold.
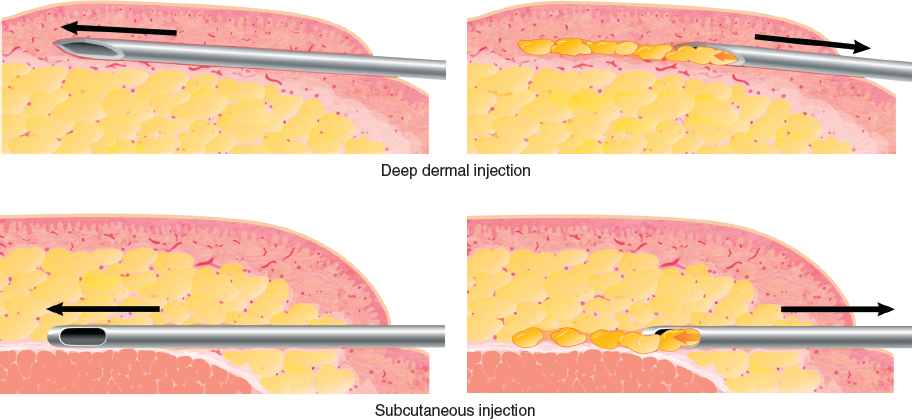
Intradermal or deep dermal infiltration of the fat can be useful to further blunt the nasolabial folds or marionette grooves in the creases.
Volume Ranges
For correcting a minimal line in the nasolabial fold, as little as 2 cc is sometimes needed. However, 2 cc is rarely enough for significant ablation of the folds, and for deep folds that have a significant premaxillary deficiency, infiltration with as much as 10 or 11 cc per side is required to adequately block the reformation of the fold. To blunt a marionette groove, much smaller amounts of tissue are used: from 1 to 3 cc. The surgeon should always prepare the patient for the possibility of a secondary procedure for the marionette and nasolabial folds.
Most Likely Technical Mistake
Isolated placement by injection into the wrinkle of the deepest part of the fold without attention to feathering into the surrounding areas can lead to a visible correction or the re-formation of wrinkles or folds in the areas immediately adjacent to placed fatty tissue.
TECHNIQUE
The key to placement of fatty tissue in the nasolabial fold and marionette groove is subcutaneous infiltration of areas rather than individual lines. However, it is often necessary to soften a distinct line or crease with a combination of deep intradermal injection with a 22-gauge needle or superficial infiltration with a type III Coleman mini-cannula.

The markings are made with arrows pointing to the depth of the nasolabial fold crease and demonstrating filling either on both sides of the crease or in the premaxillary region. In the premaxilla, I usually fill from the medial area to the crease. In the marionette region, again the filling is usually medial to the marionette groove. Therefore I delineate the outer border and show filling on the inner border.
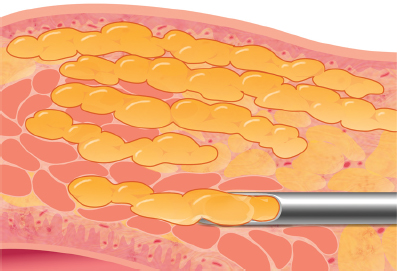
I start the placement perpendicular to the nasolabial folds or creases to feather over the area and for a “stenting” of the nasolabial fold. Structural fat placed perpendicular to a crease creates a structural barrier to the recurrence of the fold. This is important, because placement of the filaments only in a direction parallel to the fold can make the fold worse.
Through the incision in the midcheek, the cannula is inserted and is immediately brought down to a deeper level. Next, the tip of the cannula is advanced past the actual fold.

The syringe plunger is pressed minimally with each retreat of the cannula to express a small line of fatty tissue into the area of the nasolabial fold. The finger of the opposite hand is used to stabilize the area during the advancement. Approximately to cc is expressed with each retreat of the cannula in this area.
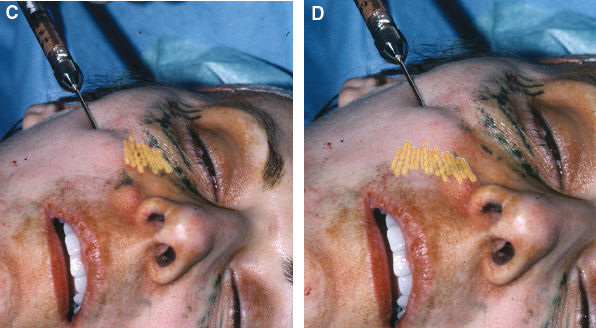
Cephalad, the fat is placed medial to the folds. Only minimal fat is placed lateral to the fold, because the area lateral to this part of the nasolabial fold is usually already fuller than the patient desires.
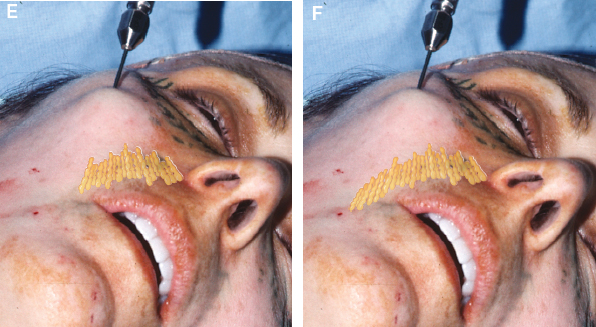
Caudally, more tissue is placed on both sides of the fold, rather than on the medial side of the fold. Particular attention is paid to any fine wrinkles or apparent weakness in the skin, since this can cause new folds to form as support is placed into the current fold.
Occasionally, the surgeon will not be able to manipulate the cannula placed through a cheek incision into a position perpendicular to the fold. This problem occurs when the nasolabial fold curves inward toward the chin rather than downward as it usually does. In this situation, by approaching the lower nasolabial fold from an incision in the border of the mandible, the surgeon can place the fat perpendicular to such a fold.
Initially a layer is placed deeply along the entire surface of the nasolabial fold. Next the cannula is placed at a more superficial level where another layer is positioned. After several intermediate layers are infiltrated, a layer is placed next to the skin. The infiltration is done using a fanlike approach; it becomes more superficial with each level of passes.
A good deal of attention is paid to the creases that are medial and lateral to the existing nasolabial folds and crease. A correction of the fold itself without infiltration of the surrounding tissues will accentuate preexisting minor creases. These will often be viewed as recurrences of the nasolabial fold. At the conclusion of each infiltration, I check for structural integrity by palpating the area.
The opposite hand is used to guide placement, and care is taken to avoid perforation of the mucosa, which is the most common means of introducing bacteria that can lead to infection.
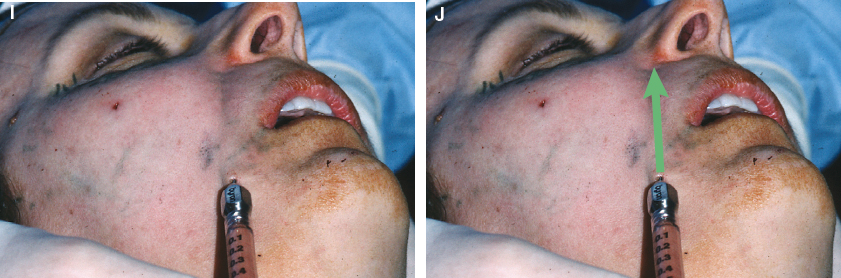
Next the nasolabial fold is infiltrated from below to complement the structural placement of the transverse elements of fatty tissue. Although the cheek approach is the most important direction for placement of fatty tissue, placing fat in a longitudinal direction allows a more precise volume correction immediately against the crease of the fold itself and adds structural integrity. In this situation, only blunt instruments are used: a type II or III cannula. Occasionally it is necessary to use a V-dissector to dissect the adherent connections.
The cannula can be advanced along the entire length of the fold. If the refined fatty tissue is to be placed along the entire length of the path, larger amounts of tissue can be expressed with each pass. Usually from to ⅕ cc can be infiltrated with each of the longer passes.
Again, placement should not be limited to the fold itself. Particular attention should be paid to any small folds or creases lateral or medial to the large fold. The filling of the larger fold may accentuate smaller surrounding folds.
As with the approach from the cheek incision, the cannula tip should be advanced to the desired position longitudinally along the length of the fold. Then, as the cannula is withdrawn, a small amount of fat is expressed into the retreating path. I usually begin deep and progress more superficially. However, for minimal corrections I start superficially in an attempt to primarily ablate the crease, since there is no deep fold to ablate. Blanching of the area of placement into the nasolabial folds and marionette grooves is common, especially with superficial placement of fatty tissue.

After placement, I pinch the area to check for structural integrity. I have found that if the nasolabial fold can be re-created by digital manipulation, the correction has been inadequate. On the other hand, if the crease cannot be forced back in the cheek, an adequate correction has been attained. The endpoint of the procedure in the nasolabial fold is when the nasolabial fold cannot be re-created with digital manipulation.
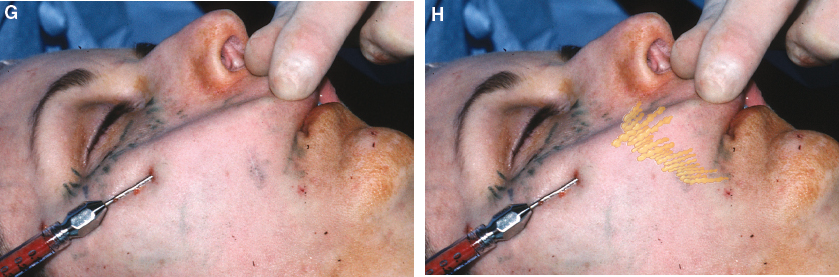
From the same cheek incision site that was used to place the fat perpendicular to the nasolabial folds, I begin the approach to the marionette region. Again, placement is guided with the opposite hand, with care to avoid perforation of the oral mucosa. The longer cannulas are a bit more unwieldy in certain situations but provide better access to this region. From the cheek, the direction of placement is primarily perpendicular to the marionette groove, with multiple passes leaving minuscule amounts with each retreat of the cannula. Often the infiltration of the marionette region is continuous with the lateral mental region. Bridging from the marionette groove down to the caudal chin forms a base, providing more structural integrity to the marionette fold in many instances.

I recommend approaching the marionette area from many directions. It can be infiltrated from the chin, oral commissure, or the lateral mental region as well as the cheek. The purpose of this multidirectional approach is to improve the texture of the region and provide structural integrity to slightly elevate the corners of the mouth. In my experience, the major change will be textural rather than structural. The upward turning of the mouth is a subtle change that may be barely evident, if it occurs at all.

Fat should not be placed into the pouchy area underneath the nasolabial fold, because this can increase the pouch and the jowl. I also do not overfill the marionette region, because the groove can easily be enlarged in some individuals. I am always enthusiastic about improving texture in this region, but efforts to eradicate the marionette grooves have been disappointing.
Although you can often achieve dramatic nasolabial fold changes with only one infiltration, the patient should be told that a secondary infiltration might be necessary. The patient also must understand that while textural changes in the marionette region will be a considerable improvement, structural alteration may be disappointing, even after multiple attempts at fat infiltration into this area. Furthermore, the addition of tissue in this area may even emphasize the downward slant at the corner of the patient’s mouth. Therefore, to avoid creating unrealistic patient expectations, the surgeon should not promise too much improvement of the marionette grooves.
One final note on technique in the nasolabial fold and marionette region. Subcutaneous placement is different from intradermal placement. Intradermal fat can usually be more effective at the elimination of discrete wrinkles or lines. However, it is not always easy to predict how much of a correction will take place with subcutaneous placement.
Related posts:
 Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
 Chapter 29 STRUCTURAL FAT GRAFTING IN THE NECK
Chapter 29 STRUCTURAL FAT GRAFTING IN THE NECK
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
 Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
 Chapter 24 STRUCTURAL FAT GRAFTING IN THE SUPRAORBITAL AREA
Chapter 24 STRUCTURAL FAT GRAFTING IN THE SUPRAORBITAL AREA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


