Chapter 27 STRUCTURAL FAT GRAFTING IN THE LIPS
Grafted autologous fat placed structurally can produce long-lasting enhancement of the upper and lower lips. The primary consideration in lip augmentation is structural form. Consistently good results come from placing tissue with careful attention to the impact that injected volume will have on ultimate lip shape. Just as an architect cannot expect to build a structure by merely piling materials on top of one another, a surgeon cannot expect to consistently change a lip into a desirable shape without knowing where the structure is being placed and how that placement will influence lip shape. With the elements of an attractive lip clearly in mind, the surgeon can precisely adjust a lip’s intrinsic composition with structural fat placement to achieve a healthy, youthful, and more sensual appearance.
Aesthetic and Anatomic Considerations
Understanding what an attractive lip looks like is not enough; the surgeon must also understand the repercussions that adding structure in one part of the lip will have on adjacent structures. In people with intrinsically well-shaped lips, volume added almost anywhere in the lip can result in an aesthetically appealing lip. However, in patients whose lips are not as well shaped, placement of volume may not be an improvement and may even deform the lip.
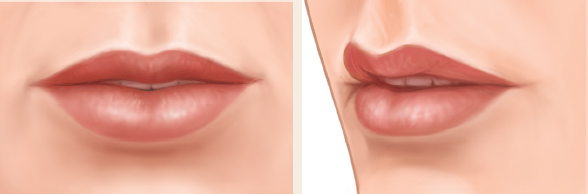
An attractive upper lip, as illustrated above, has a distinctly protuberant and continuous turgid white roll, which is separate from the skin of the lip. The white roll tapers off from peaks on either side of the Cupid’s bow and becomes less obvious laterally. Cephalad to the white roll, the skin drops back from the protuberance of the white roll to begin the slight concave curve of the upper lip. The upper lip has two distinct philtral columns curving in a similar concave fashion from their origin where the white roll hits the peaks of the Cupid’s bow to the columella. That curve is dramatically more concave inferiorly than superiorly. Under the Cupid’s bow, the vermilion of the lip has a well-centered, distinct tubercle that is the most caudal element of an attractive upper lip. Medial to each commissure is a fullness of the upper lip that is significantly less protuberant than the central tubercle in the vermilion. Between the central tubercle and the lateral fullness is a concavity or slight depression.

The lower lip has a slightly protuberant rim like the white roll of the upper lip, but less distinctive in color and turgidity. An attractive lower lip has elements that complement the upper lip following the shape, but the components are opposite those of the upper lip. A distinct central depression, essentially a cleft, is bordered on either side by tubercles significantly larger than the central protuberance of the upper lip. The alignment of the lower lip tubercles is oblique so that they push the central lip out into a distinct pout. The most important difference between the upper and lower lip in a normal, young mouth is that the amount of vermilion visible in the lower lip is much greater.
Placement of fat into the orbicularis oris muscle is not an effective strategy for encouraging eversion of the lip. This will produce a remarkable amount of superficial swelling, which will look as though the lip has everted to a more attractive shape. However, when the superficial swelling dissipates, the lip is permanently thicker without eversion of the mucosa and vermilion. The only change that is seen on photographs is a more protuberant lip without eversion.
Because the goal is eversion of the vermilion of the lip, care should be taken not to place any support into an area that might oppose eversion. For instance, placement of fatty tissue deep to the cutaneous element of the lips will increase the structural support of the skin. This may soften some of the vertical wrinkles cephalic to the white roll or caudal to the rim of the lower lip. However, increasing the structural support of the skin will invert the vermilion of the lips, making them appear smaller, relatively and absolutely.
Indications and Patient Selection
The primary indications for lip augmentation are aging (see Chapter 23) and the patient’s desire for an adjustment of facial proportion; often these two indications can both be present in the same patient.
Material and Methods
TECHNICAL GUIDELINES
Structural fat grafting to the lips can produce long-lasting enhancement of the upper and lower lip with purely autologous material. Structural form is one of the primary considerations with lip augmentation. Consistently good results are obtained by placing tissue with careful attention to the effect that injected volume will have on ultimate lip shape.
Fullness should be placed primarily below the vermilion and mucosa to create a structural expansion of the vermilion and mucosa. This expansion advances the vermilion to evert the lip.
Markings

The green pen markings outline the plan for lip augmentation. The green line below the white roll shows the plan for placement into the vermilion below the white roll, not into the white roll. The placement caudal to the white roll will extend out almost to the commissure but will end approximately 4 mm before the oral commissure. The blueprint on the left and the markings on the right show that placement into the body of the lip will be emphasized centrally and laterally to create a distinct concavity of the area not marked in green.
The beginnings of the philtral columns are marked as a reminder that placement of the fat should be extended slightly into the base of the philtral columns to slightly increase their turgor. The lateral oblique balls of the lower lip are also marked. The lower lip placement is in the vermilion next to the cutaneous lip, with no placement at all deep to the cutaneous element of the lower lip. Slight depressions in the lateral cutaneous lip were identified in this patient and marked on the skin. This is the only place that structure will be placed under the lower lip cutaneous portion.
Anesthesia
A solution of 1% lidocaine with 1:100,000 epinephrine is used for infraorbital and mental nerve blocks. Then 0.5% lidocaine with 1:200,000 epinephrine is infiltrated into the dermis at the incision sites before the incisions are made. Next, 0.5% lidocaine with 1:200,0000 epinephrine is infiltrated into the superficial muscle and submucosal planes using a type III cannula with placement of approximately 3 or 4 cc into each lip.
When I make an incision near mucosa, I give the patient prophylactic intraoperative antibiotics (usually intravenous cephalosporin). I also ask patients to gargle with Peridex preoperatively.
Incisions

The incisions for placement into the upper and lower lip are most commonly made near the commissure of the lip entirely on the cutaneous lip. I place the incision in a wrinkle line radiating from the lip. Access for the white roll placement is from the incisions near the lip commissure on either side. Occasionally, I use the midmalar incision or mandibular incisions for placement of some of the tissue, especially to approach the cutaneous lips.
Infiltration Cannulas
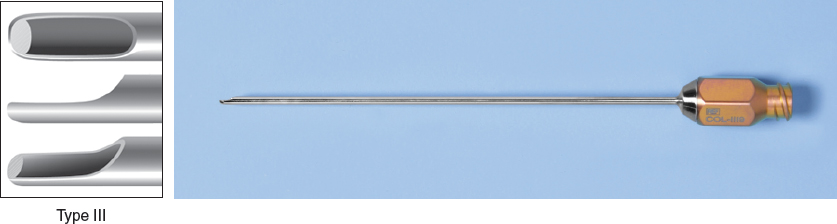
The sharpest of the blunt cannulas, a Coleman type III infiltration cannula, is used almost exclusively for placement into the entire lip. This cannula allows me to place the refined fat with the greatest accuracy into the plane immediately deep to the mucosa or vermilion. Over the past 10 years, I have been using the style III mini-cannula with greater frequency; now I use this mini-cannula mainly for placement of fat into the lips.
Level of Infiltration
Successful enhancement of the lip is not just a matter of placing a specific volume of fat into the lip. The level of fat placement is of paramount importance to consistently realize any planned changes. Almost all of the grafted fat should be infiltrated into the most superficial level, immediately deep to the vermilion and mucosa.
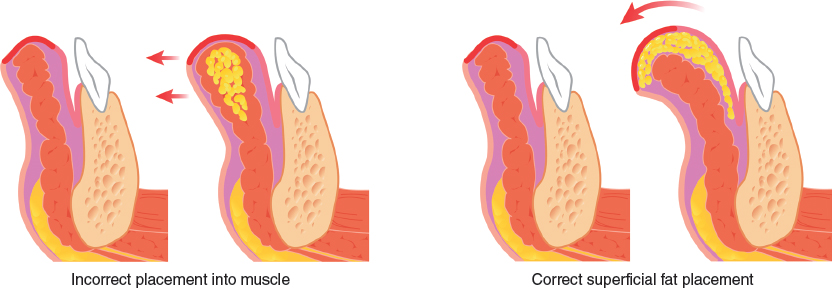
Placement of fat into the deep muscle often does little more than increase lip projection in a forward direction, which effectively increases the distance from the cutaneous lip to the teeth but does little toward creating a more voluptuous lip with improvement of vermilion show.
Almost all of the grafted fat should be infiltrated into the most superficial level, immediately deep to the vermilion and mucosa.
Placement Volumes
The suggested placement volumes are as follows:
Restructuring of the white roll: more than 0.75 cc, but rarely more than 1.25 cc
Lower lip rim: more than 0.75 cc, and less than 1.25 cc
Body of the upper lip: a minimum of 1.5 cc, but rarely more than 4 cc
Slightly more than twice the amount placed in the upper lip is placed in the lower lip body
TECHNIQUE
White Roll

Simple aesthetic augmentation of the lip begins by placing tissue into the area of the white roll. This is the most difficult and requires the most precise placement. After the cannula tip is advanced almost to the opposite commissure through the upper lip, it is withdrawn slowly across the most cephalic vermilion with gradual pressure placed onto the plunger of the 1 cc syringe. The goal is to lay down a small increment of refined fat. Placement into the white roll is usually approached from both lateral incisions. To add structure to the philtral columns, I divert the cannula up from the vermilion into the columns. This placement is extremely superficial, and the tissue is placed immediately under the skin, avoiding insertion of fat directly into the orbicularis oris muscle when possible.
Related posts:
 Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
Chapter 22 A MODEL OF AGING: A PARADIGM CHANGE
 Chapter 29 STRUCTURAL FAT GRAFTING IN THE NECK
Chapter 29 STRUCTURAL FAT GRAFTING IN THE NECK
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
 Chapter 26 STRUCTURAL FAT GRAFTING IN THE NASOLABIAL FOLD
Chapter 26 STRUCTURAL FAT GRAFTING IN THE NASOLABIAL FOLD
 Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
Chapter 28 STRUCTURAL FAT GRAFTING IN THE CHIN AND JAWLINE
 Chapter 24 STRUCTURAL FAT GRAFTING IN THE SUPRAORBITAL AREA
Chapter 24 STRUCTURAL FAT GRAFTING IN THE SUPRAORBITAL AREA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


