CHAPTER 26 Radionuclide Lymphoscintigraphy
KEY POINTS
Radionuclide lymphoscintigraphy (LSG) is an essential, noninvasive test not only for the diagnosis of chronic lymphedema, but also for the follow-up assessment of functional changes in lymphatic dynamics.
LSG is easy to perform, repeatable with reliable results, and harmless to the lymphatic endothelial lining.
LSG has been the procedure of choice for the clinical evaluation of lymphatic functional status and provides clear images of lymph transport vessels and draining nodes.
Chronic lymphedema is no longer viewed as a simple condition of static swelling of an affected limb or region after blockage of the lymph transporting and collecting systems. Lymphedema is now considered a progressive condition involving the lymphatic system and the entire skin and soft tissue integument in which a chronic degenerative and inflammatory process occurs, resulting in fibrotic change. This condition involves tissues beyond the lymphatics and lymph nodes, characterized by recurring episodes of dermatolymphoadenitis. 1 – 4
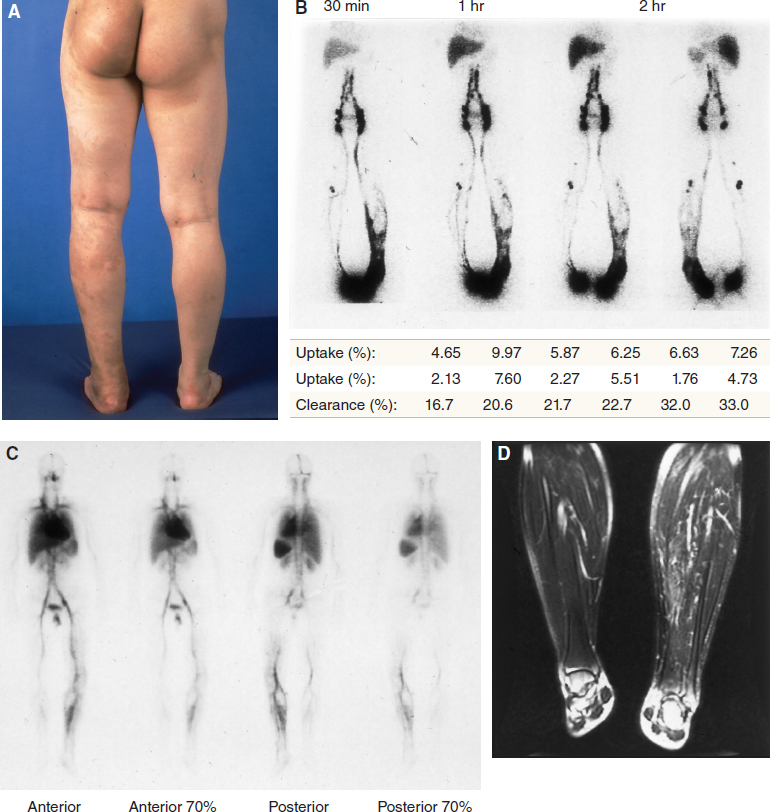
Such a steadily progressing condition that affects the entire soft tissue envelope will eventually result in a disabling and distressing condition associated with numerous complications, including bacterial and fungal infections, dermatolipofibrosis with chronic inflammation, immunodeficiency and a wasting phenomenon, and malignancy (for example, Kaposi sarcoma and lymphangiosarcoma) 5 – 8 (Fig. 26-1).

Therefore chronic lymphedema is no longer considered a simple phenomenon of fluid accumulation but the beginning of a complex systemic disease. This mandates correct diagnosis at the earliest possible stage for more effective treatment. Radionuclide lymphoscintigraphy (LSG) fulfills a critical role as a precise method of evaluation and repeated assessment of patients with lymphedema for advanced treatment and care. 9 – 12 One of the main advantages of LSG is that it is readily available at most centers, compared with some of the newer techniques, such as MRI and indocyanine green lymphangiography. Although these latter techniques in some ways provide even better information than LSG, their relatively restricted availability and evolving role mean that LSG is still the benchmark procedure.
Many conditions cause swelling (edema) that mimics lymphedema. True lymphedema as the cause of limb swelling is less common than one would think. Most cases of limb swelling are caused by local (cellulitis and arthritis), regional (deep vein thrombosis and chronic venous disease), and systemic disorders (congestive cardiac failure, renal failure, hypoalbuminemia, and protein-losing nephropathy). Moreover, lymphedema is not necessarily an isolated condition and can coexist with other medical conditions. 13 – 16
In this context, LSG is essential not only to sort out the differential diagnosis, but also to evaluate the various conditions that can be associated with lymphedema (either primary or secondary), although a careful history and physical examination are often sufficient to make the diagnosis of chronic lymphedema. 1 , 4
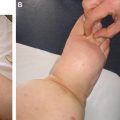
LSG is performed particularly for the assessment of primary lymphedema, because this congenital condition is the clinical manifestation of a truncular lymphatic malformation (LM) (Fig. 26-2). Together with extratruncular LM lesions, known as lymphangiomas, truncular LM malformations can occur in combination with many other vascular malformations (for example, a venous malformation). 17 – 20
Thus a detailed evaluation of primary lymphedema should be performed, including the use of LSG. Other vascular imaging studies should also be done throughout all potential areas of involvement, as well as the contralateral normal limb or body part for comparison, because various abnormal conditions of lymphatic leakage, lymphangiectasia, chylous ascites, and chylothorax are infrequently involved. 1 , 4 , 21 , 22
The basic initial diagnostic procedures for both primary and secondary lymphedema, including volumetric measurements and symptom evaluation, should be performed to make the earliest possible diagnosis in patients at risk. 23 – 26 An assessment of the clinical condition, including the clinical staging of lymphedema, requires the use of LSG, along with some other basic diagnostic tests. This is especially the case for primary lymphedema. 27
Definition
LSG is an imaging technique developed for the assessment of lymphatic function. It is a radionuclide technique that uses radioisotope-tagged or radioisotope-labeled pharmaceutical particles as a tracer, which are injected intradermally or subcutaneously. 28 – 31
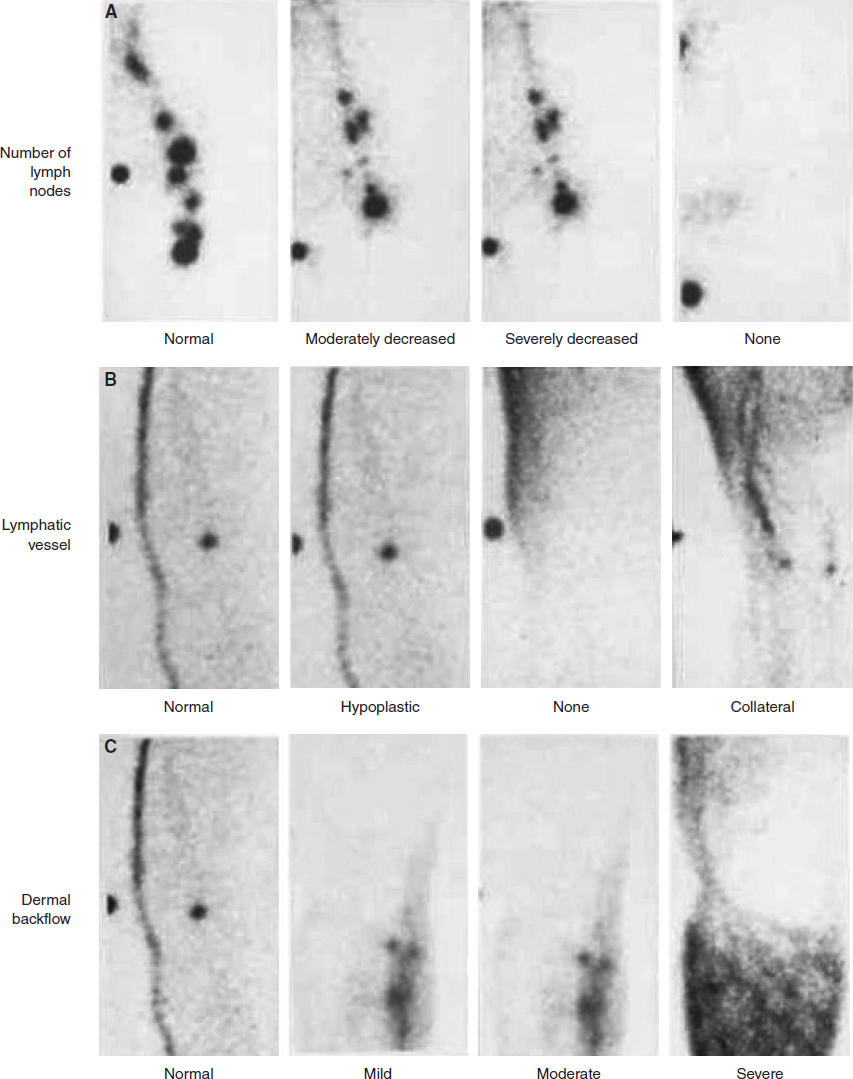
LSG is a functional study to complement the anatomic information on the lymphatic system gleaned from other studies, such as phlebography or venography. It offers not only an anatomic study of the subaponeurotic lymphatic vessels but also a functional assessment. One of the criticisms of LSG is that the anatomic definition of the images is very poor, and this is true in the context of surgical planning. Both MRI (see Chapter 28) and ICG lymphangiography (see Chapter 27) provide much better information on detailed anatomy. However, neither of these studies is as widely available as LSG. With LSG, an evaluation can be done in both qualitative and quantitative assays, and the quantitative measurements in particular can give functional imaging of the lymphatic transport capacity 30 – 33 (Fig. 26-3).
LSG, which was first introduced in 1953, has become increasingly popular because of the benign nature of the technique. LSG is a minimally invasive test, easily performed and safe. This method has largely replaced the more invasive and technically demanding technique of lymphangiography, although in the future it will likely be replaced by other higher definition studies. Nevertheless, LSG is now considered an essential test not only to confirm clinically suspected lymphedema, but also to assess the progress and response to treatment. LSG has replaced the classic role of oil contrast–based lymphangiography. 28 , 29
Before LSG became easily available for the management of lymphedema, the classic oil contrast–based lymphangiography, which was established by Kinmonth, 34 was the only tool to visualize the lymphatics. For more than 40 years, it was the procedure of choice for definitive delineation of the lymphatic system. However, three major issues associated with lymphography limited its widespread use: (1) difficulty in the cannulation of large lymphatic draining collectors through tiny skin lymphatics; (2) the risk of damage to the lymphatic endothelial lining by the iodinated oil contrast; and (3) the risk of oil (fat) embolism. 35 Because it is a difficult technique with potential side effects, lymphangiography has fallen out of favor and has largely been abandoned as a diagnostic tool. It is seldom used today. 26
Although LSG is considered a “functional” imaging modality, it delivers comprehensive and consistent images, visualizing various structural and functional changes in lymphatic flow dynamics. LSG produces dynamic images of lymphatic transport and the peripheral and central lymphatic structures and function. Its transport index score 36 allows semiquantification of peripheral lymphatic radiotracer transport. Delayed imaging shows lymph node uptake, albeit without the detailed structural information seen with conventional lymphography.
Periodic LSG findings provide proper clinical and laboratory staging, which is essential for proper clinical management 37 , 38 (Table 26-1).
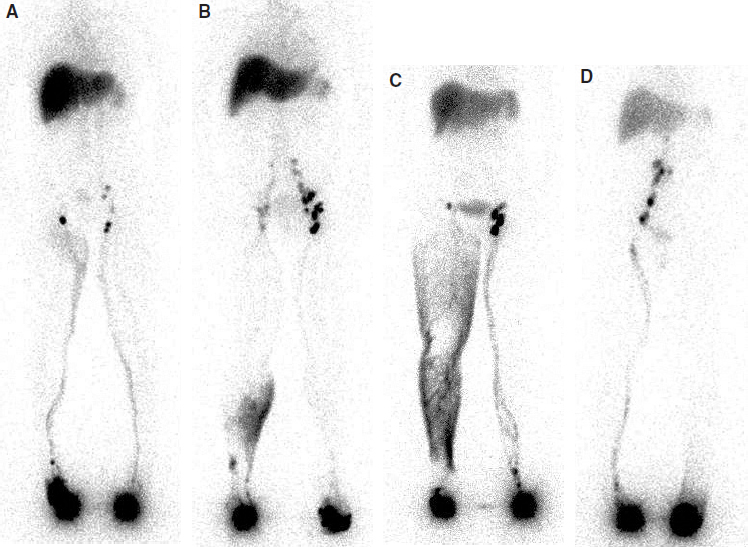
LSG also has special merit in assessing the efficacy of medicines, surgery, and physical means to facilitate lymph movement or reduce lymph formation before and after treatment. Images of truncal lymph transport and draining nodes can be routinely obtained for follow-up studies to document functional changes in lymphatic dynamics (Fig. 26-4).
However, LSG has never been fully appreciated for its ability to evaluate the lymphatic system as an independent test or adjunct to the patient’s history and physical examination. This is partly related to clinician unfamiliarity with LSG or a bias against LSG based on the old concept of chronic lymphedema. Thus the appropriate use of LSG requires a proper understanding of the new concept of chronic lymphedema. 1 , 4
LSG has now been well proved to be a safe, noninvasive, easy to perform method of assessing the lymphatic system. Furthermore, it is harmless to the lymphatic endothelial lining. In addition, technetium-99m (99mTc) has a short half-life (6 hours) and is nearly completely decayed within 24 hours.
The diagnostic value of LSG is further enhanced when combined with MRI and/or duplex ultrasonography as one of three essential noninvasive and minimally invasive tests for the evaluation of the lymphatic system. This combination of tests improves lymphatic functional assessment, allows the evaluation of the involvement of the arterial and venous systems, and provides a framework for subsequent therapy. 1 , 4
In addition to its primary role in assessing chronic lymphedema, recent advances in the understanding of phlebolymphedema as a combination of chronic venous insufficiency and chronic lymphatic insufficiency mandate a new role for LSG in the assessment of its lymphatic component, along with MRI and duplex ultrasonography. 39 , 40 Simultaneous assessment of the venous and lymphatic systems is essential for the proper identification of the delicate relationship between these two inseparable and mutually interdependent systems. Therefore a proper understanding of the unique relationship between these three tests is necessary, especially for primary lymphedema and phlebolymphedema management.
Duplex ultrasonography should be the first test performed, even before LSG, in all forms of primary lymphedema to differentiate between lymphatic and venous etiologic factors. The ultrasonic features of lymphedema include volumetric changes, a change in the thickness of the dermis and subcutaneous layer, and structural changes, such as a hyperechogenic dermis and hypoechogenic subcutaneous layer. The suprafascial and subfascial thicknesses of the edematous tissue in high resolution are very useful measurements that allow the periodic assessment of the response to therapy, monitor a patient’s progress, and determine the prognosis. 41 – 44 Ultrasonography has the distinct advantage of being noninvasive and easy to perform. However, it is very user dependent and demands a significant skill level on the part of the ultrasonographer.
The features of MRI include circumferential edema with a typical honeycomb pattern, in addition to increased subcutaneous tissue volume with marked thickening of the dermis. MRI is also helpful to identify lymph nodes and enlarged lymphatic trunks and to differentiate the various causes of lymphatic obstruction in secondary lymphedema. The anatomic information from MRI provides a substantial complement to the functional assessment provided by LSG. 45 , 46 A more detailed description of MR lymphangiography, including the most recent developments in this technology, is found in Chapter 28.
Recently LSG and CT scans have been combined to improve diagnostic accuracy by retrieving functional (scintigraphy) and anatomic (CT) data together. 47 , 48 The limb volume computation is accurate with this three-dimensional reconstruction of the limb by the volume rendering technique 49 to characterize excess fluid limited to the skin and subcutaneous tissues.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


