CHAPTER 25 Hydromechanics of Intercellular Fluid and Lymph
KEY POINTS
In normal limbs, lymph flow occurs only during spontaneous contractions of lymphangions.
In obstructive lymphedema, the stagnant tissue fluid is primarily deep in the subcutaneous tissue.
In advanced stages of lymphedema, the hydraulic conductivity of the subcutis decreases.
Tissue fluid pressure is low in advanced stages of lymphedema because the interstitial spaces of the subcutis expand.
Compression pressures of 50 to 60 mm Hg are recommended in early stages of lymphedema, and pressures of up to 125 mm Hg are needed in advanced stages.
Human limb soft tissues are composed of skin; subcutaneous tissue containing loose connective tissue structures such as ground matrix, fibers, and adipocytes; nerve fibers; blood and lymphatic vessels; muscular fascia; and muscle fibers. All of these tissue elements bathe in the fluid filtered from blood exchange vessels, which is partly mobile and partly taken up by cells bound to the matrix. In cases of enhanced plasma filtration or obstruction of tissue fluid flow to the lymphatics, and further, to the blood circulation, the interstitial space becomes overloaded with fluid. This is clinically diagnosed as tissue edema.
In the lower limbs, the estimated extravascular extracellular volume is 12% of the total tissue volume under normal conditions, whereas in lymphatic obstruction it may be 40% to 50%. 1 Knowledge of the location of excess fluid and its pressure/flow mechanics is necessary to understand the role of tissue fluid in the metabolism of parenchymal cells under normal conditions and in patients with lymphedema from obstruction of lymph flow. Such information is indispensable for effective antiedema therapy.
Various external forces in specific directions should be applied in compression therapy, depending on the mobile fluid topography at different limb levels; the fluid location in the deep layers of the subcutaneous tissue, around blood vessels and nerves, and above and under muscular fascia; and the hydraulic conductivity at various levels.
Accumulation of Tissue Fluid and Lymph Under Normal Conditions and in Obstructive Lymphedema
Our understanding of the limb lymphatic network in physiologic conditions and in lymphedema is based on lymphographic or lymphoscintigraphic images of the superficial and deep systems and lymph nodes. This technique does not reveal minor lymphatic structures located under the epidermis. Direct lymphangiography with fluorescent tracers may be helpful in delineating minor dermal lymphatics but is rarely used, as it requires special equipment for visualization. Ultrasonography, CT, and MRI provide pictures of tissue spaces filled with stagnant tissue fluid; however, they do not show lymphatics. None of the listed methods provides sufficient imaging of the entire tissue fluid and lymph space—including the interstitial space and lymphatics—to know what these tissues look like in reality. It is difficult to imagine how tissue fluid in the areas with obstructed lymphatics finds its way to the normal, noncongested tissue regions and is absorbed. To date, it is only through anatomic dissection and histologic processing of biopsy material that one can visualize the tissue lymphatic network and the sites of accumulation of the excess mobile tissue fluid. 1
Under normal conditions, the volume of mobile tissue fluid is negligible. Collecting lymphatics contain little lymph in the lymphangions (segments of lymphatic vessels bounded by valves). Some of them remain empty. The situation changes dramatically with the obstruction of lymph flow caused by damage to the lymph collectors: subepidermal lymphatics dilate and tissue fluid spaces form in the subcutaneous tissue around small veins and in the muscular fascia.
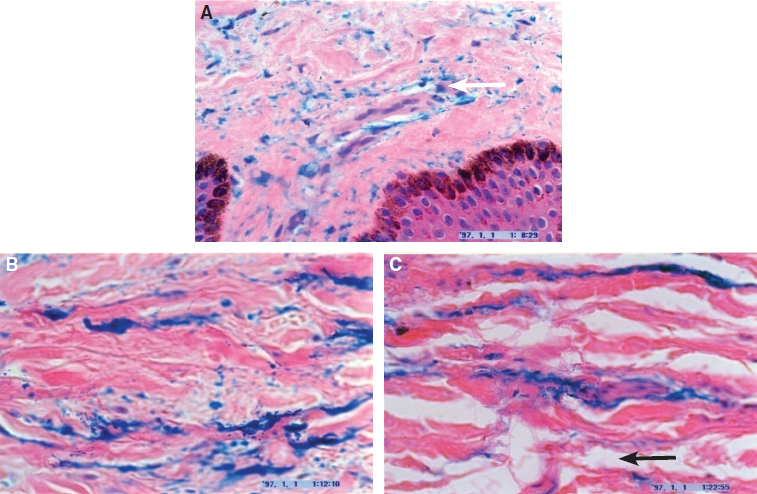
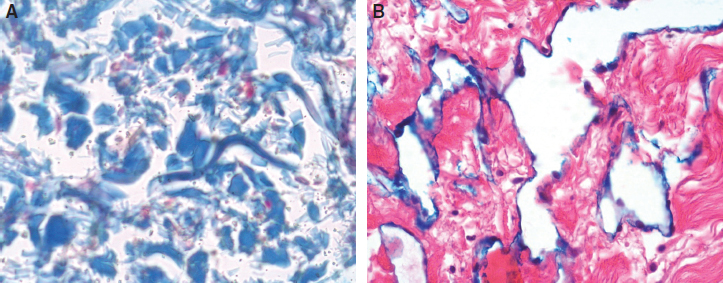
The most superficial layer where fluid accumulates is the subepidermal lymphatic plexus, occupying a papillary and reticular dermis with a thickness of 200 to 300 microns (Fig. 25-1). However, the volume of fluid in this plexus is negligible, compared with the volume of the subcutaneous tissue fluid, and does not exceed 2% to 3% of the total tissue fluid retained in soft tissues. The bulk (95%) of mobile tissue fluid accumulates in the subcutaneous tissue, forming artificial, partly interconnected spaces (Fig. 25-2). These spaces are located between fat globules, fibrous bundles, and around small veins.
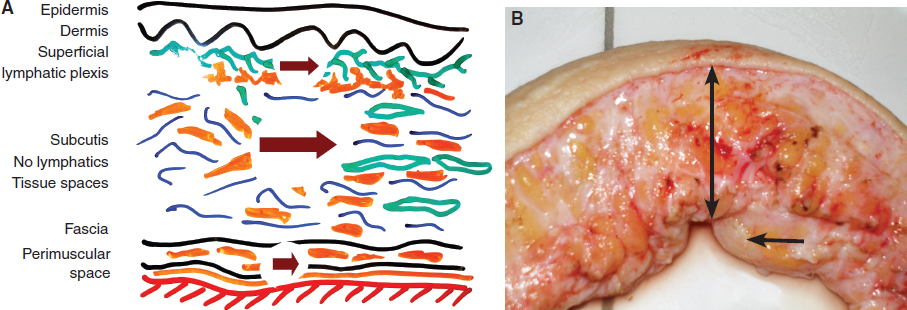
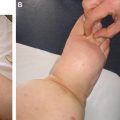
The formation of large lakes of tissue fluid can be explained by the presence of lax connective tissue in these regions, its high compliance and subsequently low resistance to fluid flow. Tissue fluid channels form, which mostly are narrow longitudinal spaces between the normal fascial fibrous elements around and in the hypertrophic muscular fascia of the calf, sometimes reaching 2 cm in diameter. The hydraulic conductivity of these structures is high because of the linear positioning of fibers. 2 The volume of fluid accumulating in the tissue spaces and calculated from the densitometric readings of the stained tissues can be as high as 40% to 50% of the total tissue volume 1 (Fig. 25-3, A). Anatomic images of the skin and subcutis in lower and upper limb lymphedema show that the thickness of edematous tissues is 1 to 10 cm or more (Fig. 25-3, B). (The staging system referred to in this chapter is that of W.L. Olszewski. 14 ) This information raises the following question: How much massaging force should be applied to affect the deepest edematous tissue layers? In this chapter, we attempt to answer this question.
Tissue Resistance to Flow and Dissipation of External Force
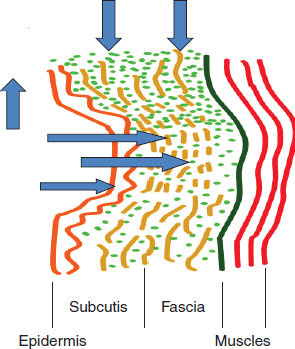
Which tissue elements create tissue resistance to fluid flow, and where is most of the external force dissipated? The answers to these questions are presented in Fig. 25-4. Skin has inherent stiffness and becomes even harder in advanced stages of lymphedema because of continuing fibrosis. The subcutaneous tissue contains collagen, elastic fibers, and fat agglomerates. Its stiffness is lower than that of skin. However, in lymphedema, fibrogenesis makes it less elastic. These structures create resistance to flow. To move mobile tissue fluid, a pressure gradient should be generated between the collagen bundles and the ground matrix, perpendicular to the limb axis (middle horizontal arrow). The hydraulic conductivity of the subcutis thus steadily decreases. Higher external pressure will be needed to mobilize edema fluid in the deeper layers. The subcutaneous tissue becomes swollen and is relatively thicker than the skin.
The amount of force lost during external compression can be estimated by measuring the pressure of the therapist’s hand on the skin, or measuring the undergarment pressure of a bandage or pneumatic device on the skin, and comparing that with tissue fluid pressure. The difference between applied and in-tissue, generated pressure will provide information on how much force was absorbed by the solid tissue and how much was used for generating the fluid pressure gradient necessary for propelling tissue fluid. Thus loss of force should always be taken into account when planning compression procedures. Compression-generated tissue fluid pressures are always lower than pressures applied at the compression device–skin interface. 3
MEASUREMENT TECHNIQUES
Intralymphatic Pressure and Flow
To measure intralymphatic lymph pressure, a subcutaneous lymph vessel of the leg is cannulated against the direction of lymph flow, according to published techniques. 4 , 5 The lymph vessel draining lymph from the skin, subcutaneous tissue, and perimuscular fascia of the foot and anterior aspect of the lower leg is cannulated. Pressures are recorded by an electronic micromanometer.
To measure intralymphatic flow, we use a low-flow flowmeter that measures from 0.1 to 6 µl/min, with an accuracy of 0.1 µl. 5
Tissue Fluid Pressure and Flow
To measure tissue fluid pressure, the wick-in-needle technique is routinely used. An 8-gauge injection needle with polyethylene tubing (outer diameter 1.34 mm) containing a glass-wool wick protruding 5 mm from the tubing tip is introduced under the skin. The outer part of the tubing is connected to the pressure transducer, and recordings are obtained using a three- or six-channel device. We use LabVIEW software. 3
Tissue fluid flow is measured using strain-gauge plethysmography. The device measures circumference changes in the calf and thigh segments corresponding to the compressed limb region or sequentially inflated pneumatic sleeve chambers. The data are used for calculating volume changes of the limb caused by the proximally moved tissue fluid. The volume value obtained before compression is subtracted from that obtained during compression, providing data on the proximally transferred fluid volume. 3
Characteristics of Lymph and Tissue Fluid
NORMAL TISSUES
Lymph and tissue fluid hydraulics in human limb soft tissues, under normal conditions and in lymphedema, have been studied only in a few centers. 6 – 11 The hydromechanics of lymph and mobile tissue fluid (normal and stagnant edema) differ considerably. Lymph is contained in the lumen of a rhythmically contracting vessel generating a pressure gradient, whereas tissue fluid is contained in the interstitial space, limited by cells and fibers. (Hydraulic conditions change dramatically with obstruction of the draining lymphatics.)
Extrinsic Factors Propelling Lymph
Muscular activity, respiratory movements, passive movements, and arterial pulsation have no effect on lymph flow. 6 – 8 , 10 , 11 Generally, limb lymphatics are empty, with only a few microliters of lymph in some lymphangions. In a normal leg positioned upright, the lymphatics have no hydrostatic pressure. 8 , 11
Intrinsic Factors Propelling Lymph
Lymph is propelled by autonomous rhythmic contractions of lymphangions. 6 – 11 Tissue fluid enters the initial lymphatics to flow into the lymphangions. Stretching of lymphatic walls by inflowing tissue fluid causes contractions of the lymphatic wall muscles (according to Starling’s law for the heart muscle) and generates flow.
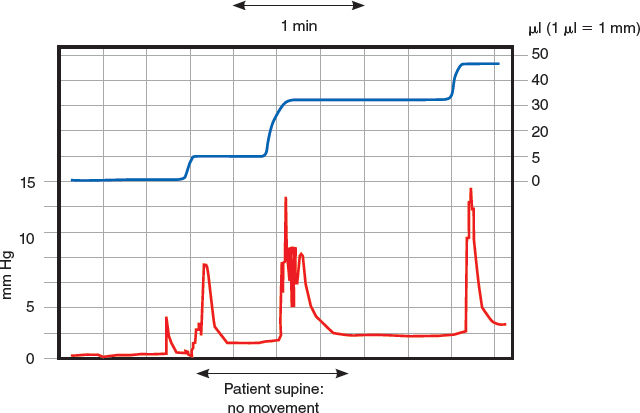
Lymph Pressures
Limb lymphatics contract rhythmically; the frequency depends on the volume of inflowing tissue fluid (Fig. 25-5). The frequency is high in regions with a high capillary filtration rate and tissue fluid formation. Table 25-1 outlines normal lymph pressures. Massaging of the foot or tapping of tissues containing lymphatics has no effect on lymph pressures. Heating of the foot significantly increases the pressure, amplitude, and frequency of lymphatic contractions. 8 , 11
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


