CHAPTER 24 Measuring Methods
KEY POINTS
No perfect measurement tool for lymphedema exists.
Limb circumference and volume are the most commonly performed measurements for lymphedema.
Volume is most frequently calculated using the truncated cone model.
Perometry is a reliable method of measuring limb volume, but it is not universally available.
Lymph flow measurement using lymphoscintigraphy is a reliable way to document lymphedema.
MRI provides excellent information but is not easily applicable for documenting ongoing changes.
Bioimpedance analysis is probably the most useful method for diagnosing preclinical lymphedema.
Making a diagnosis is one of the most important things that physicians do when they first see a patient with lymphedema. Evidence suggests that a subjective assessment through patient self-reporting is a more sensitive and less expensive means of diagnosing the development of lymphedema. 1 – 3 Nevertheless, it is useful to maintain objective documentation. A combination of both approaches is probably best.
The first step in diagnosing lymphedema is to determine the extent of the disease. This requires some sort of measurement. A means of comparative and quantitative assessment of the results of treatment is also required. The measurement technique needs to be standardized, quantitative, repeatable, and reproducible; it should also be easily available and inexpensive. The most often used quantitative assessment of lymphedema is assessment of size based on the measurement of circumference or volume. Other methods include measurements of lymph flow, tonometry (to evaluate compressibility), and bioimpedance. 4 – 6 Each of these methods has advantages and disadvantages. No perfect measuring technique exists.
Measurement of Limb Circumference and Limb Volume
Limb circumference and limb volume are the most frequently obtained measurements in patients with lymphedema.
MEASUREMENT OF LIMB CIRCUMFERENCE
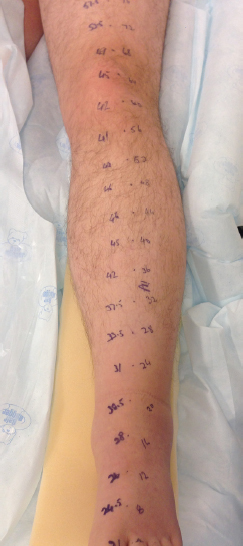
Limb circumference is measured from a fixed point such as the tip of the long finger or from anatomic landmarks such as the patella or the olecranon (Fig. 24-1). Identification of local landmarks can be problematic in lymphedematous patients, because they may not be readily palpable. Furthermore, landmark descriptions may have various interpretations, which can lead to confusion and inaccuracy. For example, the patella can be measured from the proximal end, the distal end, or the middle. This can make a significant difference, particularly when measurements are repeated and compared at different time points. Limb circumference as a means of measurement has been criticized because of inconsistencies in tape measure tension and placement from one measurement to the next. Although measurements at specified intervals from a fixed point may seem to be a more accurate technique, Taylor et al 7 found excellent correlation between measurements taken in reference to fixed anatomic landmarks and plethysmography.
MEASUREMENT OF LIMB VOLUME
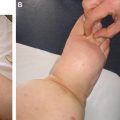
The most widely accepted measure of lymphedema is limb volume. The affected limb can be compared with the unaffected limb, or measurements of the affected limb can be compared before and after interventions or events that led to the lymphedema. Volumes are most accurately measured by plethysmography or water displacement 8 – 10 (Fig. 24-2). However, defining and replicating the upper level for immersion can be difficult, and water displacement is not convenient for routine clinical use.

Brorson and Höijer 11 followed 10 women with unilateral upper extremity lymphedema after breast cancer treatment. They calculated volume indirectly by circumference measurements (CM), using the formula for a truncated cone. The authors developed two Excel-based formulas of the truncated cone: one for fixed 4 cm intervals, leading to 10 volume segments (VS) (CM-10-VS), and one for varying intervals, leading to four volume segments (CM-4-VS). Plethysmography yielded greater volumes, because the hand was included, but excellent correlation was observed between volumes measured by plethysmography and volumes measured by limb circumference from a fixed point. No difference was noted between CM-10-VS and CM-4-VS. In my practice I have adopted the CM-10-VS method, because in my experience, it is simple, reproducible, and repeatable, regardless of who obtains the measurements. For the upper limb, circumference is measured at 4 cm intervals from the tip of the long finger, and for the lower limb, similar measurements are taken at 4 cm intervals from the tip of the second toe.
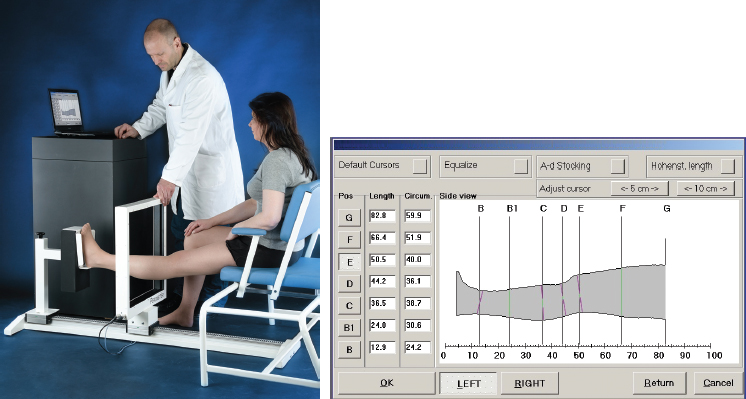
A Perometer (Pero-System) is an optoelectronic imaging device designed to measure the volume of an object. It is ideally suited for measuring limb volume. It consists of a square measuring frame that contains rows of infrared light–emitting diodes on two adjacent sides and rows of corresponding sensors on the other two sides 12 (Fig. 24-3). Two rows of measurement arrays are placed at a 90-degree angle to each other. Each of them determines an object diameter and its position inside the frame. The patient sits at one end of the Perometer, with the hand or foot resting centrally on an adjustable support or footplate. The frame is then moved along the length of the arm or leg, from the wrist to the axilla or from the ankle to the thigh. When the frame is moved manually, the diameters and positions are determined in short distances along the object. The collected data are not influenced by the position of the measured object within the frame. A computer produces a volume picture of the entire limb by using the cross-sectional information obtained from the biplanar shadow of the limb in the device. The collected data can be saved and analyzed. Data generated by a Perometer can be exported into other programs such as word processing programs, spreadsheets, or other standard software.
Perometry has been rigorously assessed by comparison with other methods and is considered more accurate than tape measurements. 12 , 13 In various studies it has proved highly reproducible, accurate, and reliable. 14 This technology is safe and fulfills many of the criteria for an ideal measurement tool. However, it is not inexpensive or easily accessible.
NUANCES OF CIRCUMFERENCE AND VOLUME MEASUREMENTS
One of the biggest confounders of circumference and volume measurements is that causes of increased volume other than lymphedema are not taken into account. For example, breast cancer patients tend to gain weight after having chemotherapy. 15 Measurement of changes in limb circumference or limb volume measurements alone is not helpful in distinguishing between increases from lymphedema and other causes. This confounder can be somewhat controlled in patients with unilateral lymphedema by comparing the affected side with the contralateral, normal limb. In patients with bilateral lymphedema, however, this method is not as useful.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


