Chapter 21 TREATMENT OF DIFFICULT WOUNDS AND SCARS WITH FAT GRAFTS
The use of fat grafting has become a common practice among plastic surgeons around the world aiming at the possible benefits of adipose-derived stem cells (ADSCs) for regenerative purposes and for their ability to differentiate in fat, bone cartilage, muscle and possibly other tissues. This injected (or deposited) fat has also a great variety of regenerative and metabolic properties, as well as growth factors such as EGF, TGF-beta, HGF, PDGF, and BFGF. 1 – 4
The adipose tissue to be used in fat grafting is harvested by common liposuction techniques. The lipoaspirate can be treated by physical or chemical methods or by a combination of both, in the operating room or in the laboratory, concentrating or isolating stem cells, which can be injected and/or deposited in the area to be treated.
Over recent years, we have progressively changed our routine treatment of deep burn wounds of the hand or foot from excision with grafting to excision with fat grafting, and only occasionally with skin grafting. We also treat referrals from a local state hospital, typically patients with chronic leg wounds with exposed bone, with or without fractures. In the past, we would rotate a muscle flap over the (fractured) bone and graft immediately; currently, we treat the majority of these with fat injection and delivery. These cases have healed with very satisfactory results.
Similarly, we have also used fat grafting for treating pressure sores (decubitus ulcers), in other fractures and around tendon repairs, as well as for releasing eventual fibrotic adhesions of these healed sites. One of the most pleasant surprises and common findings for surgeons initiating and continuing to use fat grafting is that there is minimal or no hypertrophic scarring if the grafting is used in the acute phase, or that grafting controls the development of hypertrophy when used after healing has occurred.
Indications for Fat Grafting for the Treatment o f Dif ficult Wounds and Scars
Candidates for adjuvant treatment with a fat grafting procedure at our service are those with:
Deep second- or third-degree burns of the hand or the foot
Burn wounds that have had no apparent progression toward healing for 3 or more weeks
Subacute burns or other wounds within more than 6 weeks after the accident, with or without open wounds or fractures
Hypertrophic scars that are not improving after 6 or more weeks with the use of pressure garments or devices, or that are causing functional deformities
Deformities around joints and their consequences resulting from the development of fibrosis
Partial scar resections, when fat is injected under the suture line, immediately after the resection is performed
Filling of decubitus ulcers, avulsion injuries, and void spaces, with or without flap repair (eliminating the use of suction drains)
Material and Methods
We use the Coleman technique in all procedures (see Chapter 1). We repeat injections in wounds every 2 to 3 weeks until healing or a definitive procedure is performed, such as skin grafting, a flap, or some other operation. After these wounds are healed, procedures using fat grafting through injections under the scar and/or delivery to its surface are performed at 3-month intervals. In patients who present to us when their wound is already healed, we also graft fat to the hypertrophic scars that do not respond to pressure; we perform the grafting at 3-month intervals, using similar techniques. In hypertrophic scars that will lead to a functional deformity, fat grafting is performed as soon as the deformity is diagnosed, and these injections are repeated at 2-month intervals. 5 – 7
OBJECTIVES OF TREATMENT
Fat grafting sessions 15 to 21 days apart are used in wounds to take advantage of fat’s benefits; the objective of treatment is to obtain healing of the wound. 8 – 10
When treating burns or other scars, the objective is to decrease the amount of hypertrophy (fibrosis), diminishing the scar thickness and increasing scar malleability. We also use this technique to decrease fibrosis around bone joints and to release tendon adhesions. 11 – 13
ANESTHESIA
Procedures are performed with the patient under general anesthesia.
DONOR AREAS, INCISION SITES, AND VOLUME
We rotate among donor sites as needed. Fat is most frequently obtained from the abdomen, inner thighs, or lateral upper buttocks. Incisions for introduction of the liposuction cannula are placed on the midline, at the suprapubic crease, or medial to the femoral pulse, at the inguinal crease (with the patient supine), or in the middle axillary line, at the upper border of the iliac bone (with the patient in the lateral decubitus position).
The actual volume of harvested lipoaspirate should be at least twice the anticipated volume that the surgeon plans to inject, and at least four times this volume if the plan includes delivering fat over the wound. Fat is delivered by laying the prepared fat directly over the wound or the scar that has been pretreated with a laser or microneedling. The amount of fat delivered or laid over the area is usually approximately 2 ml/10 cm2, and this fat is covered with fine mesh Vaseline® gauze.
As an initial volume estimate, we consider that approximately 2 cc of prepared (centrifuged) fat will be needed for every 10 cm2 of wound area. One must also consider that on average, 30% to 40% of the lipoaspirate is discarded as oily or aqueous fractions after centrifugation.
PATIENT POSITIONING
Patients are placed supine when the abdomen or thighs are the donor areas or in the lateral decubitus position when fat is obtained from the lateral upper thighs. Fat is usually injected while the patient is supine.
PROCEDURE
Because fat harvesting and grafting are sterile surgical procedures, these should be performed only in accredited operating rooms using rigorous, completely sterile technique. When necessary, shaving of the pubic area or proximal thigh is performed in the operating room immediately before the procedure.
In patients with scars (healed wounds), the donor area and recipient area are individually prepped and draped in the usual manner. In patients with open, nonhealed wounds, the recipient area is prepped only after the planned amount of fat is obtained, while it is being centrifuged and distributed in multiple syringes.
Fat is harvested using a 10 cc Luer-Lok syringe attached to a 3 mm cannula, with two 3 mm side openings distally. We use lengths of 10, 15, or 20 cm, depending on the harvesting site. The cannula is introduced through a No. 15 blade puncture incision.
In children weighing less than 25 kg, we prefer to use 20 cc syringes and multi (micro)–perforated cannulas, which will generate a higher negative pressure and a more even and efficient fat harvesting, respectively. Occasionally, in very small patients (our smallest patient weighed 13 kg), it may be necessary to harvest fat from more than one donor site.
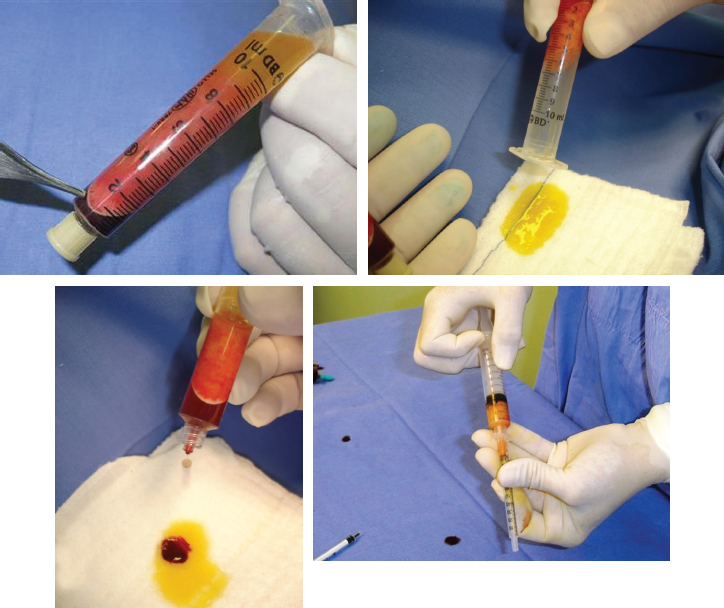
One or more distally plugged 10 cc syringes containing the lipoaspirate is centrifuged at 3000 rpm for 3 minutes in a 30-degree-angle centrifuge. The resulting material will have a top layer of oil, a middle layer of fat with the stromal vascular fraction (SVF) within at its lower portion, and an aqueous bottom layer. The top layer of oil is discarded while the plug is still on the syringe. The plug is then removed and the aqueous layer drains out by gravity. The remaining compound is sequentially injected into insulin syringes without the plunger, which is then replaced.
Fat Injection
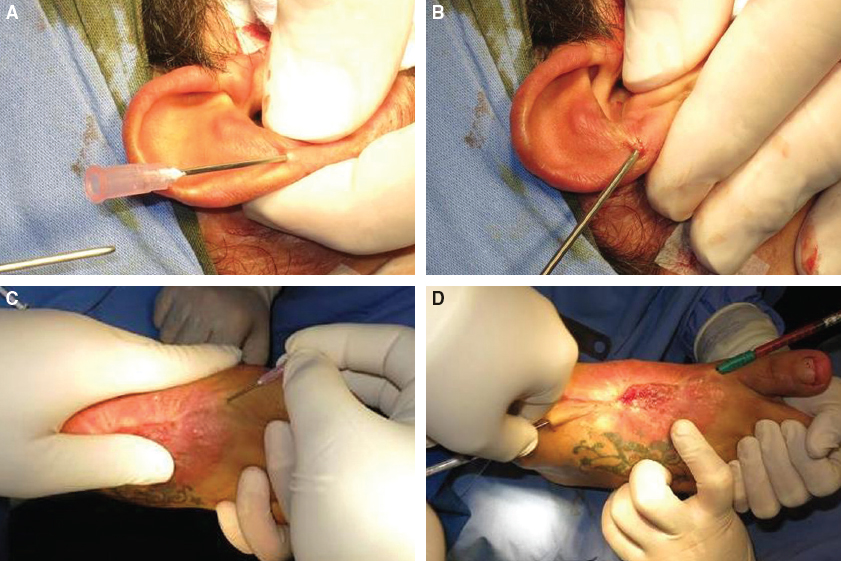
Fat is injected through a perforation made with a 16-gauge needle at an acute angle in healthy skin in the periphery of the wound or scar. A 70 mm long cannula with a 1.8 mm outside diameter and a 1.2 mm internal diameter, connected to a 1 cc syringe, is inserted through the needle puncture hole and forcefully driven immediately under the wound bed or the scar. (Patient 1, A and B, 0.8 cc of fat was injected; patient 2, C and D, 12 cc of fat was injected.)

Fat is injected in a retrograde manner in several passes until the entire area has been covered, through as many puncture sites as needed around the periphery of the scar or wound. An average of 1.6 to 2.0 cc is injected per each 10 cm2 area; 25 to 30 passes are necessary to inject a total of 1 cc. In chronic wounds, fat is also injected under the indurated, “healed” area in the periphery of the remaining wound. 14 – 17 (A through D, 0.3 cc of fat was injected in the ear and 4 cc in the facial scars. E through H, in the same patient, 1.5 cc of fat was injected in each wound and 0.8 cc to each wound.)

This 48-year-old diabetic woman presented with a venous ulcer that she had had for 3½ years. The size and depth of the erythematous peripherally indurated area was significant. After debridement of the wound, 8 cc of fat was injected under the wound. A needle roller was applied in all directions on the indurated tissue. Then 22 cc of fat was delivered/laid over the indurated area (pretreated with microneedling) and the wound. This patient eventually had one more similar procedure performed 15 days later, and a skin grafting 32 days later, with healing occurring within 44 days of treatment.
Fat Delivery
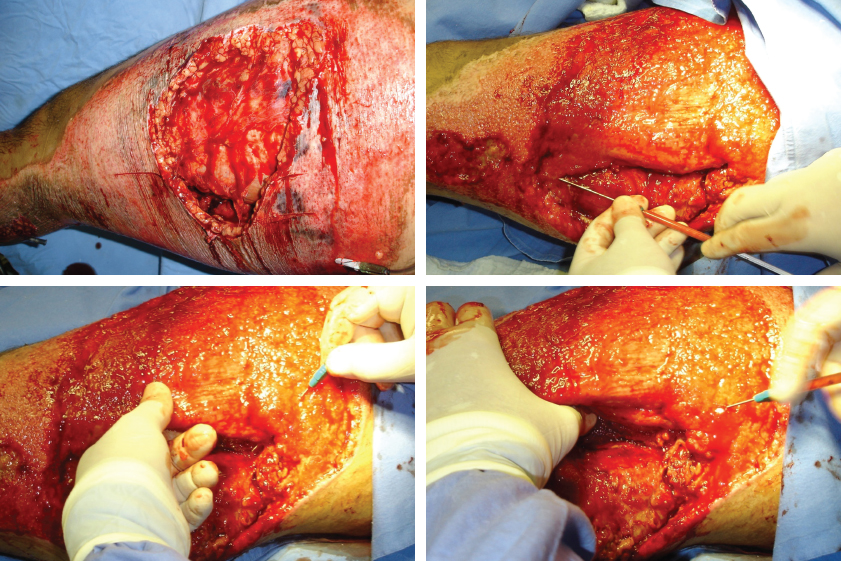
This 32-year-old patient was seen 8 days after a crush injury from a motorcycle fall with an infected hematoma. Drainage and excision of necrotic tissue were performed. Fat grafting (22 cc) was performed on day 12, through the wound, inside the muscle septa and the muscle spaces, and delivered/laid over the entire wound (28 cc). Fat can occasionally be injected through the wound in larger areas or when there are fracture lines, bone-loss voids, or exposed bone. In such cases, fat can be targeted to these specific areas.
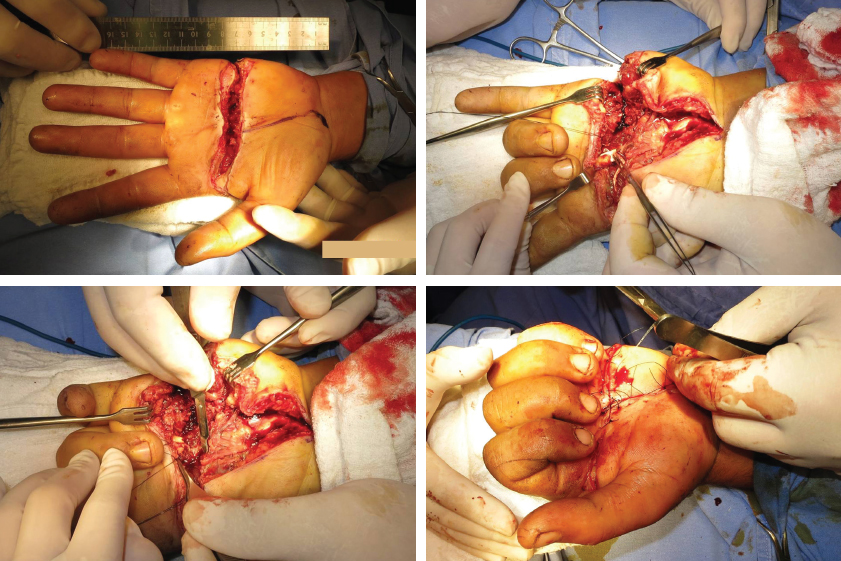
This 22-year-old patient was seen 6 days after making contact with an urban high-tension line (13,800 volts) while holding a metal screen. He sustained electrical injuries to the left hand and complete rupture of the flexor tendons for the second through fifth fingers. The tendons were surgically reconnected, and 8 cc of fat was grafted into the open wound and over the tendons. Fat allowed for an excellent recovery. This same patient is shown in Fig. 21-10, E through H.

Fat is delivered directly over scar tissue that was previously treated with a fractional CO2 laser or a needle roller. A total of 16 cc of fat was delivered to the facial scars (C). The puncture wounds so produced will carry the delivered fat to within the scar tissue, greatly increasing the effect of the ADSCs and the contained growth factors. The desired result is a greater decrease in hypertrophy and a major improvement in malleability.
In wounds in which the entire thickness of the skin or more noble tissue (nerves, blood vessels, tendon, bone) has been lost, fat is also deposited in a zigzag pattern over the entire surface of the wound, using the same cannula as for the injection. When treating scars, fat can also be delivered directly to (over) the scar, after the area is treated with a needle roller or a fractional CO2 laser. The needle roller or the laser will produce minimal puncture wounds on the scar substance, through the skin epithelium, and these holes will absorb the centrifuged fat and its contents directly, thus amplifying the benefits of fat grafting.
Related posts:
 Chapter 17 MICROFAT INJECTIONS WITH DISPOSABLE CANNULAS
Chapter 17 MICROFAT INJECTIONS WITH DISPOSABLE CANNULAS
 Chapter 20 SCLERODERMA AND FAT GRAFTING
Chapter 20 SCLERODERMA AND FAT GRAFTING
 Chapter 19 STRUCTURAL FAT GRAFTING FOR THE REGENERATION OF IRRADIATED TISSUE
Chapter 19 STRUCTURAL FAT GRAFTING FOR THE REGENERATION OF IRRADIATED TISSUE
 Chapter 16 IMPROVING SKIN QUALITY: AN EXPERIMENTAL AND CLINICAL STUDY OF THE EFFECTS OF FAT AND STROMAL CELLS ON THE SKIN
Chapter 16 IMPROVING SKIN QUALITY: AN EXPERIMENTAL AND CLINICAL STUDY OF THE EFFECTS OF FAT AND STROMAL CELLS ON THE SKIN
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


