CHAPTER 21 Basic Approaches to the Diagnosis of Lymphedema: Clinicians’ Perspective
KEY POINTS
Lymphedema can be defined as the chronic accumulation of lymphatic fluid in the interstitial space between tissue cells.
The differential diagnosis of edema requires a detailed medical history of the patient and a physical examination. Physician experience diagnosing lymphedema also plays a key role.
According to the 2013 Consensus Document of the International Society of Lymphology, lymphedema can be divided into four stages.
To establish an accurate diagnosis of lymphedema, the most important factors are the duration of the swelling, clinical findings, and whether the disease is unilateral or bilateral. Clinical tests, such as an MRI, CT, SPECT-CT, and isotopic lymphoscintigraphy, also play a crucial role.
Clinically, lymphedema can be described as chronic excessive fluid accumulation in the interstitial spaces between tissue cells. This deposition (which at least in the extremities is epifascial) swelling is a consequence of increased inflow or decreased outflow or both. 1
The diagnosis of lymphedema is basically made by a familial and clinical history and physical examination. To do this well, the physician should have many prior assessments of clinically manifest lymphedema.
The typical presentation of a patient with early to midstage lymphedema is with a combination of the following signs and symptoms: whole or partial limb swelling; tightness in the skin; pitting caused by rings, a watchband, tight socks, or underwear; and a history of recurrent infections or functional complaints, such as heaviness, fatigue, and difficulty moving joints. 2 , 3 Most patients will also have a history of injury or damage (for example, from cancer treatment) to the lymphatic system, because secondary lymphedema is the most common form of lymphedema, at least in Western populations. However, we are now aware that for some of these patients, there may be an underlying primary component. Furthermore, obesity, infections, and a history of radiotherapy significantly increase the risk of lymphedema.
Patients with primary lymphedema may have a family history; however, sporadic forms of primary lymphedema are more common. In these situations, the diagnosis of primary lymphedema is one of exclusion. 3
Differential Diagnosis
There are many reasons for a swollen limb, and an accurate and appropriate diagnosis is critical to ensure the appropriate treatment. The differential diagnosis of edema requires a detailed medical history of the patient, physical examination, and occasionally special laboratory tests, such as an MRI and ultrasonography. Although distinguishing, the duration and distribution of the edema and the presence of dermatologic changes depend on the reason for the edema. 4 , 5
According to the 2013 Consensus Document of the International Society of Lymphology, 6 lymphedema has four stages. Stage 0 refers to the latent or subclinical period. Stage I refers to the early phase of swelling. Stage II swelling is accurate, and limb elevation does not reduce the swelling alone, although it does in stage I. Stage III refers to lymphostatic elephantiasis.
If the duration of the edema is less than 2 weeks and also unilateral with the presentation of pain, it may be related to an acute condition, such as deep vein thrombosis, cellulitis, or a ruptured Baker cyst. 7
If the edema is gradual and progressive over a few months (suggesting chronicity) and is unilateral without pain, then a possible diagnosis may be chronic venous insufficiency, external venous compression caused by a tumor of the iliac region of the lower extremity, or tumors of the soft tissue or vascular structures. 8 However, lymphedema (primary or secondary) cannot be easily excluded.
If the beginning of the edema is gradual, progressive, and bilateral, possible causes include congestive heart failure, glomerulonephritis, cirrhosis, lipedema, chronic venous insufficiency, or a malignancy in the pelvis, abdomen, or retroperitoneal space. 7 , 8 Of course, it could also be bilateral lymphedema. Table 21-1 defines the differential diagnosis.
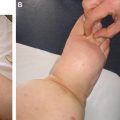
Rarely, patients with long-standing lymphedema will present with lymphangiosarcoma, an aggressive tumor with a 5-year survival rate of less than 10%. This complication was first reported by Stewart and Treves in 1948 in patients with postmastectomy lymphedema and is referred to as Stewart-Treves syndrome. In this case, patients present with red or purple nodules in the diseased tissues and are most commonly treated with amputation (Fig. 21-1).

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


