CHAPTER 20 Causes and Classification of Lymphatic Disorders

KEY POINTS
Primary lymphedema is generally categorized based on age of onset and is presumed to have a genetic basis.
Lymphedema is a hallmark feature of various syndromic disorders.
Secondary lymphedema arises as a consequence of other conditions or treatments.
Any surgical intervention can precipitate lymphedema.
Lymphangiomatosis can be isolated or systemic, superficial or visceral. It is generally characterized by the depth of the malformation within the tissue planes.
Lymphatic filariasis results from an infection and worldwide is the most common cause of lymphedema.
Abnormal development or damage to blood and lymphatic vascular systems can contribute to the appearance of complex vascular malformations.
Protein-losing enteropathy and intestinal lymphangiectasia are associated with the loss of lymphatic fluid and plasma protein within the lumen of the gastrointestinal tract.
Lymphedema is a complex edematous state resulting from dysfunction of the lymphatic transport system that is essential to the maintenance of tissue homeostasis. Beyond lymphedema, however, there is a broad spectrum of diseases that directly or indirectly alter lymphatic structure and function. These lymphatic vascular diseases, which are characterized by a failure of adequate lymph transport, lead to a wide range of pathologic presentations. 1 Given the central role of lymphatic function in circulatory homeostasis and a robust immune and metabolic contribution (based on suitable dietary absorption of gastrointestinal lipids), any lymphatic pathology will become clinically manifest as a regional or systemic immune impairment and/or significant metabolic derangement, often accompanied by chronic and often debilitating regional swelling and tissue edema. 2 – 4
Embryologic Development
The lymphatic system arises from endothelial cells within the embryonic venous structures. Specific molecular markers determine the lymphatic endothelial cell specification and thus its unique phenotype. Additional lymphatic-specific markers are expressed, and blood vascular expression profiles are suppressed as the lymphatic endothelial cells continue to differentiate. 5 Vascular endothelial growth factor C is necessary for the earliest steps of lymphatic endothelial cell differentiation. 6
The differentiated lymphatic cell population migrates peripherally and establishes complete autonomy from the local venous environment. This developmental stage is characterized by primary budding. The primary lymph sacs form throughout the embryo, followed by secondary budding and migration. The latter requires endothelial sprouting into tissues to form local capillaries, thereby marking the final stages of lymphatic development. 7 , 8
Lymphedema
The International Society of Lymphology consensus document has identified four stages in the natural history of lymphedema. 9 Stage 0 refers to a latent or subclinical condition in which swelling is not seen despite the presence of impairment in lymph transport. Stage 1 is seen as pitting edema. There is early accumulation of fluid that is relatively high in protein content and resolves with limb elevation. Stage 2 is characterized by the presence of pitting edema that does not resolve with limb elevation alone. Stage 3 is lymphostatic elephantiasis, in which pitting is no longer seen. The lymphedema is characterized by trophic skin changes, such as acanthosis, fat deposition, dermal cutaneous fibrosis, and verrucous overgrowth. 10
Although lymphedema can be hereditary, its development can also be sporadic. Its cause is either primary or secondary:
Primary lymphedemas are congenital, developmental, or inherited disorders that arise from an inborn malformation or dysfunction of the lymphatic system.
Secondary lymphedema arises as a consequence of other conditions or treatments.
Lymphedema is not a reversible condition. Its treatment is largely mechanical and requires physiotherapeutic interventions that reduce limb swelling through the stimulation of lymphatic contractility and that control reaccumulation of edema through limb compression. Complete decongestive therapy is a multicomponent treatment that reduces the degree of lymphedema and maintains skin health. 11 – 13 At present there is no long-term pharmacologic therapy that is recommended for patients with lymphedema.
PRIMARY LYMPHEDEMA
Primary lymphedemas are congenital, developmental, or inherited disorders that arise from an inborn malformation or dysfunction of the lymphatic system. In general, these disorders do not shorten life expectancy but worsen quality of life. 14 They are presumed to have a genetic basis; an autosomal dominant transmission pattern is most often described. Numerous distinct gene mutations associated with lymphedemas have thus far been noted and characterized. 15 , 16
Primary lymphedemas are classified by the age of onset:
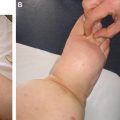
Congenital lymphedema presents at birth or by the age of 2 years
Lymphedema praecox presents before 35 years of age (most often in association with puberty).
Lymphedema tarda appears after 35 years of age.
Congenital lymphedema can be syndromic in nature (for example, Noonan syndrome, Turner syndrome, or Klippel-Trenaunay syndrome) 16 , 17 and can be organized by its pattern of inheritance. Chromosomal disorders, such as Klinefelter or Edwards syndrome, can result in multiple organ defects and a wide constellation of symptoms and complications, including a severe distortion of lymphatic function. 3 Typically, congenital lymphedema of the hands and feet is seen in infants with Turner syndrome. 18
Milroy disease, or hereditary autosomal dominant congenital lymphedema, presents as painless, nonprogressive edema of the lower extremity in infancy. 19 It has been associated with mutations in the kinase domain of vascular endothelial growth factor receptor 3 (VEGFR-3), with incomplete penetrance. 20 Despite the association of Milroy disease with a systemic mutation, lymphoscintigraphy often reveals normal, functional lymphatic anatomy in the upper limbs, but inadequate lymphatic functional integrity is present at the sites of swelling in the lower limbs. 19
Lymphedema-distichiasis is a single-gene disorder caused by a mutation in the gene that encodes the nuclear transcription factor FOXC2. This is another common cause of primary lymphedema. Distichiasis (abnormal cilia arising from the meibomian glands along the lid margin) typically presents at birth, but the lymphedema generally presents at puberty (often earlier in males) 21 ; it is an accompanying somatic anomaly that is found in 94% to 100% of patients with lymphedemadistichiasis. This feature can lead to recurrent corneal irritation and conjunctivitis. 19 FOXC2 mutations can also be associated with the presence of cleft palate or congenital heart disease. Lymphoscintigraphy reveals reflux within the main collector lymphatics; in addition, deep vein reflux is seen on venous Doppler ultrasound examination. 19 , 22
Lymphedema praecox (lymphedema presenting before the age of 35) is the most common form of primary lymphedema. 23 The edema in this disease is often unilateral and commonly limited to the foot and calf. 24 The disorder is characterized by an initial presentation at puberty and female preponderance, leading to the hypothesis that estrogen may play a role in the expression of the lymphedema. 24 Meige disease is a term that has been applied to a familial form of lymphedema praecox with pubertal onset and an autosomal dominant pattern of inheritance. 19
SECONDARY LYMPHEDEMA
Secondary lymphedema arises as a consequence of other conditions or treatments. However, there is a growing conviction that genetic factors contribute to the susceptibility to the stressors that elicit an ostensibly pure acquired lymphedema. In other words, in many cases, there may be a primary predisposition to the development of secondary lymphedema.
A common cause of acquired lymphedema is iatrogenic, as a result of treatment of malignancies. Furthermore, and less commonly, tumors can primarily obstruct lymphatic channels or infiltrate the lymphatic system, leading to lymphedema through obstruction of lymph flow. Treatment of a wide variety of cancers is associated with a significant incidence of lymphedema, including breast cancer, malignant melanoma, urogenital malignancies, lymphoma, and soft tissue sarcomas. 25
Any surgery can result in lymphedema. The operative intervention can be for cancer (for example, a modified radical mastectomy or even a partial excision) or a non-cancer-related procedure, such as varicose vein ligation or saphenous vein harvesting for aortocoronary bypass. 26 , 27 Trauma, infection, and burns can also lead to the development of lymphedema. Moreover, peripheral arterial disease can result in secondary lymphedema. 26 Iatrogenic causes, such as intrathecal pump insertion or sirolimus administration, are common precipitators of lymphedema. 28 , 29 Globally, infection is considered the leading cause of lymphedema. In tropical regions, endemic lymphatic filariasis predominates and is the most common worldwide cause of lymphedema. 30
Acquired Conditions
INFECTIOUS DISEASES
Lymphatic filariasis and lymphangitis are two conditions in which invading pathogens infect and infiltrate the lymphatic system, which leads to lymphatic dysfunction. The consequence of such events can often result in a chronic obstruction to lymph flow (acquired lymphedema), which is accompanied by the resulting impairment in regional immune function.
More than 140 million people worldwide have been infected with filariasis. The prevalence and global burden of the disease lag only behind malaria and tuberculosis. 31 Most of these infections are caused by Wuchereria bancrofti, whereas the remaining cases are caused by Brugia malayi. 32 Patients are infected by the larvae of these filariae, or parasitic worms; after the larvae are delivered through the wound, they enter the draining lymphatic vessels. The larvae develop into mature adult worms that produce microfilariae, which then enter and circulate in the bloodstream.
Lymphatic filariasis can be asymptomatic (subclinical) or can have acute or chronic clinical manifestations. Acute presentations include adenolymphangitis, which is characterized by fever and painful lymphadenopathy. Ultimately, there is fibrosis of the lymph nodes and impaired regeneration of lymphatic channels. Dermatolymphangioadenitis is another acute presentation that is characterized by inflammatory plaques and systemic symptoms as a consequence of superficial bacterial infection of damaged skin. 33 Other acute presentations include filarial fevers and tropical pulmonary eosinophilia, which is caused by an immune response to filariae trapped in the lungs. Chronically, filariasis can lead to lymphedema, hydrocele, and renal involvement. 34 Active infection can be diagnosed by the detection of the microfilariae in the blood; detection of localized, lymphatic obstruction by Doppler ultrasound is feasible. 31 Serologic techniques can be substituted for the microscopic detection of microfilariae. The infection is treated with antibiotics and antiparasitic medications, such as albendazole, diethylcarbamazine, and ivermectin. 35 – 37
Lymphangitis represents an inflammation of the lymphatic channels, most often seen in relation to infectious causes, including bacterial, mycobacterial, fungal, viral, and parasitic pathogens. 38
Lymphangitis often develops after cutaneous inoculation of microorganisms through a skin wound or as a complication of a distal infection that invades the lymphatic vessels and spreads toward regional lymph nodes. Lymphangitis can also reflect inflammation in the setting of malignancy (neoplastic lymphangitis or lymphangitis carcinomatosa) or a systemic inflammatory process, such as Crohn’s disease (granulomatous intestinal lymphangitis) or sclerosing lymphangitis of the penis. 39 – 43 Recurrent episodes of bacterial lymphangitis lead to thrombosis and fibrosis of the lymphatic channels; this is one of the most common causes of lymphedema. 44 The clinical presentation of this disease often encompasses the presence of painful erythematous cutaneous streaks and enlarged and tender lymph nodes. 38 Patients also frequently have a history of minor trauma or skin infection and fever, chills, muscular pain, and headache. 45
Imaging is rarely used for infectious causes, but lymphangiography and lymphoscintigraphy can be used to detect anatomic abnormalities, such as lymphatic obstruction or dilated, tortuous lymphatic vessels. 46 Treatment most often involves the use of antimicrobial agents; some patients require surgical debridement. 38 , 47
Congenital Conditions
LIPEDEMA
Lipedema is a chronic disorder of adipose biology that results in symmetrical, bilateral, fatty subcutaneous tissue deposition in the lower extremities and buttocks. The condition is characterized by hyperplasia and hypertrophy of adipocytes. Lipedema can occur with lymphedema, although lipedema has distinctive features that allow it to be differentiated from the more common problem of lower extremity lymphedema. In lipedema, the skin is often sensitive to pressure. Affected individuals have both spontaneous pain and pressure-induced discomfort. The problem is also associated with easy bruising and hematoma development after even minimal trauma. In lipedema the Stemmer sign is absent, and the condition is described as foot sparing. Moreover, it is often characterized by a normal cutaneous architecture, with no demonstrable dermal fibrosis or cutaneous thickening. Lipedema almost exclusively affects females and is often associated with a familial distribution. Lipedema can ultimately cause secondary lymphedema (socalled lipolymphedema) by distorting the microlymphatic function. 7 , 48 – 50 Therapies are mostly conservative and similar to those used in lymphedema, including complex decongestive therapy, pneumatic compression, manual lymphatic drainage, bandaging, and diet modifications. 51 , 52
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


