Chapter 18 Complications and Adverse Effects

Introduction
All procedures have the potential to cause complications. The physician in charge of the procedure must be able to diagnose the condition and provide suitable treatment.
Ecchymosis
Filling procedures can cause ecchymosis, which is observed more frequently following injection into the dermal plane and when using fanning or crosshatching technique. Ecchymosis occurs less frequently with the bolus technique and in the supraperiosteal plane. To minimize the risk of ecchymosis and/or hematomas, the patient should avoid taking medicinal products such as acetyl salicylic acid, warfarin, clopidogrel, nonsteroidal antiinflammatory drugs (NSAIDs), fish oil, vitamin E supplements, St. John’s wort, garlic capsules, gingko biloba, and ginseng, from one week prior to the procedure. It is, however, important to ask for the prescribing doctor’s written consent before suspending any medicinal product. If ecchymosis occurs, patients should be advised to avoid sun exposure until it disappears completely, and intense physical exercise should be avoided in the first 24 hours. Ecchymosis can also be avoided by using microcannulas. 1
Edema
Immediate Edema
Transitory edema in the immediate postoperative period is nor mal and is associated with the technique used, the number of punctures, and the volume injected.
Antibody-mediated Edema (Angioedema)
Some patients may develop hypersensitivity to the product in jected due to an IgE-mediated hypersensitivity reaction (type I reaction), which can occur after the first exposure or after repeat exposures. IgE stimulates degranulation of mast cells, releasing proteases, heparin, histamine, cytokines, prostaglandins, and leukotrienes, resulting in edema, erythema, and pruritus, which are characteristics of an allergic reaction. Edema can be confined to the site of injection or be generalized. Treatment consists of antihistamines in combination with prednisone. Rapidly progressive angioedema is treated as a medical emergency because of the risk of airway obstruction.
Nonantibody-mediated Edema (Delayed Onset)
Delayed hypersensitivity reaction is characterized by induration, erythema, and edema, mediated by T-lymphocytes. It generally occurs one day after the procedure, but can start weeks later and last for several months. It can be treated with prednisone and hyaluronidase.
Edema Due to Congestion
Some patients can present with edema even months after the procedure, due to the hygroscopic characteristics of the filler agent. Situations such as sinusitis and crying can cause facial congestion and consequent water retention at the filler injection site.
Erythema
It is normal to experience a certain degree of erythema immediately after the procedure, but if it persists for more than a few days, it is probably a hypersensitivity reaction. In these cases, a medium-strength topical corticosteroid can be used. High-strength corticosteroids should be avoided due to the risk of atrophy and telangiectasis. Laser and intense pulsed light (IPL) are good adjuvants.
Infection
As with any procedure that breaks the skin barrier, there is an associated risk of infection. Good antiseptics should be applied to the site to minimize this risk. The skin can be cleansed with 70% alcohol, immediately followed by chlorhexidine solution. It is also important to use surgical gloves during the procedure and to take care not to contaminate the tip of the needle or cannula. The responsible organisms are usuallyStaphylococcus aureusorStreptococcus pyogenes,but delayed signs of infection, two weeks after the procedure, can be suggestive of atypical infection. Mild forms can be treated with oral antibiotics (PO), but more severe cases require systemic antibiotics and hospitalization. The differential diagnosis includes a delayed hypersensitivity reaction, which also causes erythema, but generally involves itching with no local heat. The formation of abscesses is a rare complication that can occur from one to several weeks after the procedure. Abscesses should be drained, and antibiotic therapy should be prescribed according to the culture results.
Patients with a history of herpes virus may suffer reactivation. When applying filler injections to the lips and perioral region, prophylactic treatment with valaciclovir should be started before the procedure (500 mg, 2/day, for 5 days). The majority of reactivations occur in the perioral region, nasal mucosa, and hard palate. Differential diagnosis should be made with vascular occlusion (Fig. 18.3). 1 ,. 2
Nodules
Nodules can be classified didactically as noninflammatory and inflammatory. 1 ,. 2
Noninflammatory Nodules
These result from an accumulation of the product in a specific area, due to overcorrection or a very superficial injection. They are palpable and/or visible after the procedure and their differential diagnosis includes foreign body granuloma, biofilm, and other inflammatory nodules. They are treated with massage alone or in combination with hyaluronidase.
Inflammatory Nodules
Delayed-onset erythematous nodules are generally painful, and secondary to hypersensitivity to the product, infection, or foreign body reaction. The differential diagnosis of these reactions is often diffcult; therefore, when faced with a nodule or indurated plaque, regardless of the time since onset, bacterial biofilm should be considered.
A biofilm is a structured community of bacteria that surrounds a polymeric matrix. When a product is injected into the skin, it can be contaminated by bacteria and form a biofilm. These bacteria secrete a protective and adherent matrix that allows them to adhere to a living or inert surface, forming a chronic, low-grade infection that is nonetheless resistant to antibiotics. Biofilms also secrete free bacteria into the tissues. Several species of bacteria form biofilms, and the longer the infection lasts, the greater the resistance to antibiotics.
When activated, for example, by trauma from another procedure, a biofilm can cause local or systemic infection, inflammatory response, or granulomatose response. As cultures are usually negative, it was thought that these nodules are caused by allergic or granulomatous reactions to the filler. Antibiotic therapy is the first step for treating a patient with a suspected biofilm, even when the culture is negative. Quinolones, such as ciprofloxacin 500 mg every 12 hours, and macrolides, such as clarythromycin 500 mg every 12 hours, can be administered for t wo weeks. In the case of f iller i njections with hyaluronic acid (HA), the use of hyaluronidase should be considered after starting antibiotic therapy. Biofilms can be treated according toFig. 18.1.
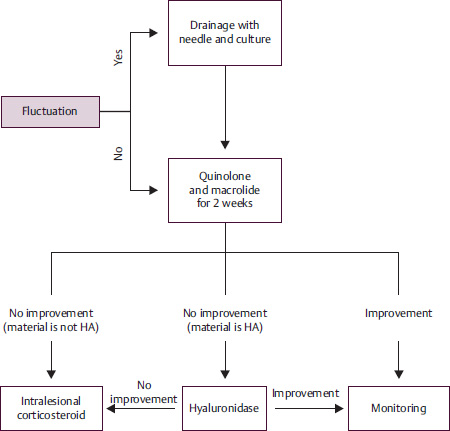
A strategy for reducing the risk of biofilm formation is to clean the patient’s face properly before the procedure, avoid injecting through the oral mucosa, avoid permanent materials, and not inject in the same plane used for another filler injection or in traumatized tissue (Fig. 18.4). 3
Paresthesia
Nerve lesions are a rare complication and occur due to direct trauma, when the nerve is pinched or partially lacerated by the needle, when the injection is applied inside the nerve, when the product compresses the nerve, or when the nerve foramen is massaged vigorously. Nerve lesions can be transitory and reversible or permanent. Neuropraxia refers to a nerve lesion without axon rupture, which can result in sensory or motor deficiencies, but which improves after 2 to 3 weeks. The transection of small sensory skin nerves (axonal injury) can result in an anesthetic plaque at the site of nerve innervation; this injury is also reversible, and sensibility returns after a few months. The most common site for dysesthesia, paresthesia, and anesthesia is the region of the infraorbital nerve, caused by intraneural or intraforaminal injection, or by compression of material in the foramen after vigorous massage. Treatment with injections of triamcinolone into the foramen, dissolution of palpable material with lidocaine or saline solution, and vitamin B12 capsules are reported in the literature. 1
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


