Chapter 17 Filler Injection of the Chin and Mandible Contour
Introduction
The contour of the lower third of the face is determined by the inferior edge of the mandible. A well-defined mandibular line, well-proportioned chin, and marked mandibular angle are all characteristics of a young and attractive face.
Filler injections with a more viscous and cohesive hyaluronic acid (HA) are an excellent option for remodeling the facial contour, making it possible to restore the volume lost over time, or to provide greater projection and contour for certain facial biotypes.
Three different face types are routinely def ined in the literature. The mesofacial type expresses balance, whereas the brachyfacial and dolichofacial types are at opposite ends of the biometric scale of the face. Mesofacial individuals have proportionate horizontal and vertical dimensions. Brachyfacial and dolichofacial ones have diametrically opposed characteristics; those with brachyfacial features have shorter and broader faces than those with dolichofacial features. It is important to remember that this classification is academic, so on a daily basis you will come across patients with intermediate characteristics between one biotype and another. 1 There is also a classification of the face with respect to the position of the mandible in relation to the cranium. Most people find class I profile attractive (normal or orthognathic mandible). The class II profile presents increased facial convexity because of a rare maxillary excess or mandibular deficiency. Normally, a maxilla with a good facial expression can be observed in individuals in whom the lower third of the face is deficient and the chin-neck line is short. Brachyfacial and class II individuals can benefit from filler injec tions in the lower third of the face. It is important to remember that odontological assessment is fundamental, as this procedure provides increase in volume, but does not correct occlusion alterations. 1 –. 4
The lower third of the face also differs between sexes. A man’s face is more contoured, and the mandibular line and angles are more defined. In women, however, two facial formats predominate:
Heart-shaped face: the malar and zygomatic regions are clearly apparent, and the inferior contour is delicate and not very expressive.
Angular face: the malar and zygomatic regions are significant, with an expressive inferior contour that has welldefined mandibular line and angle.
Anatomy
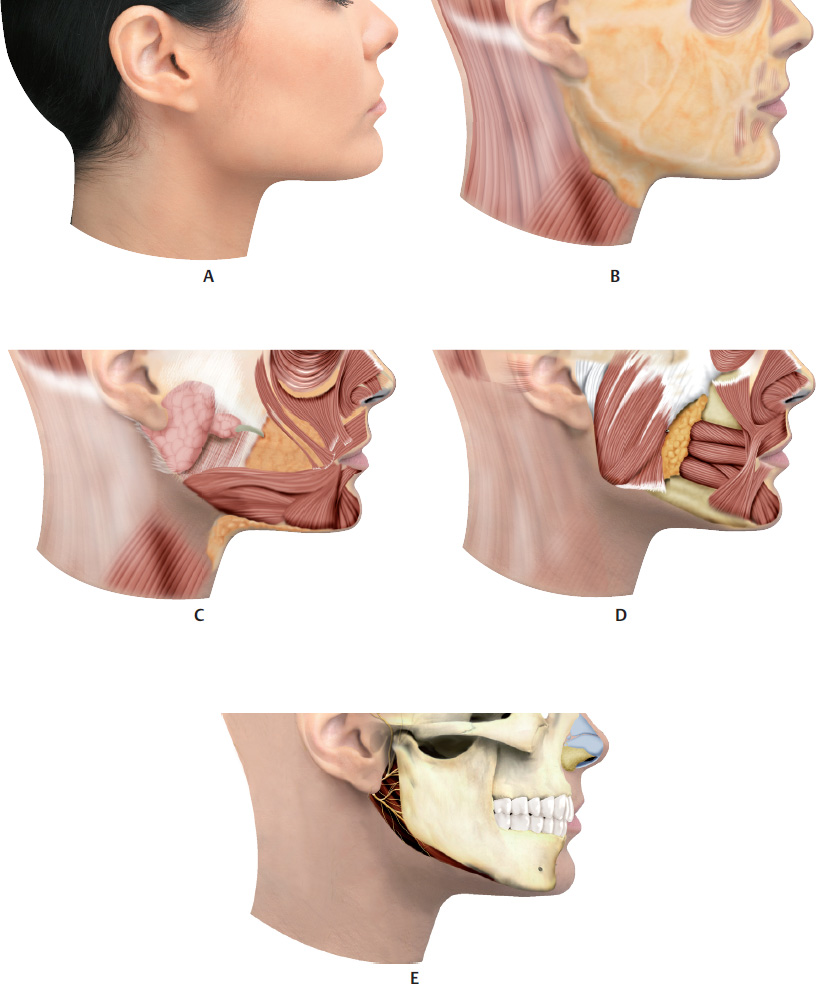
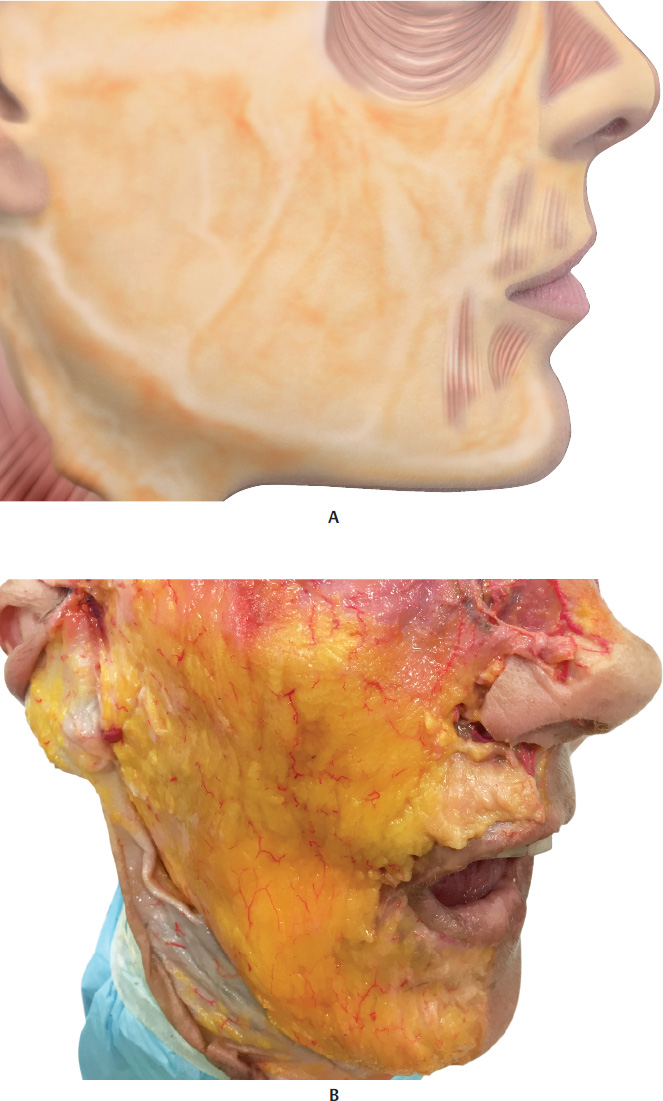
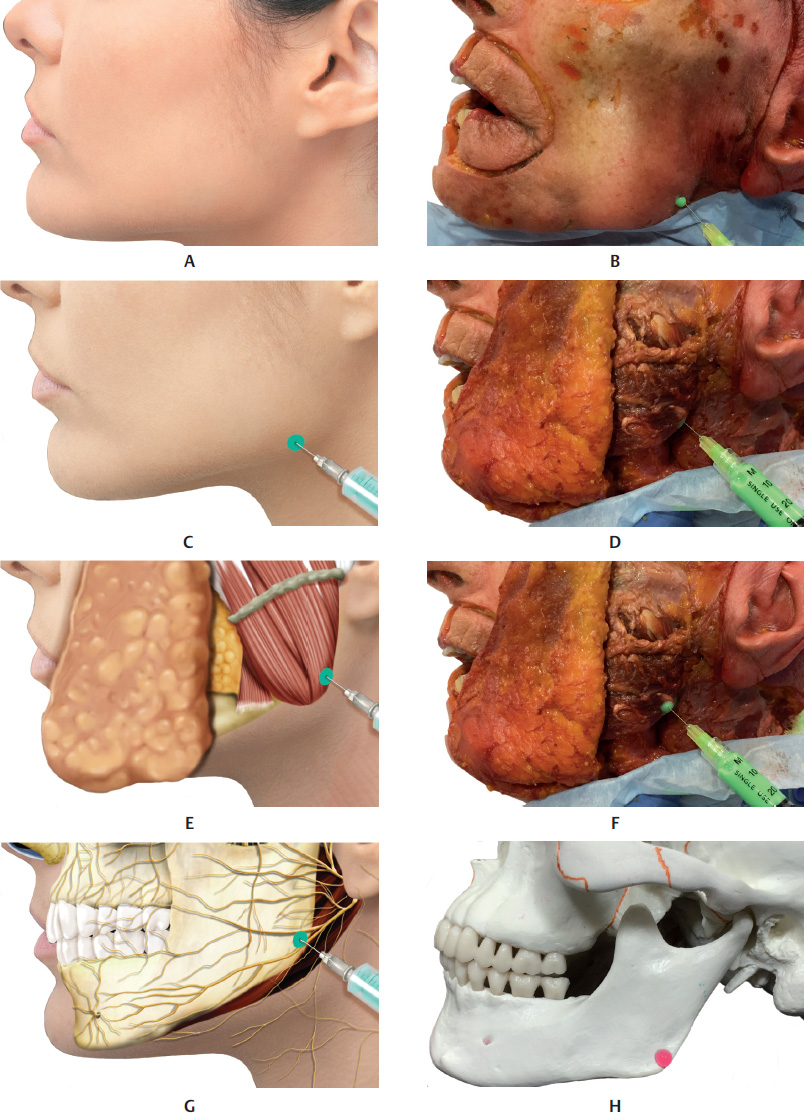
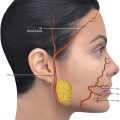
The mandible, or lower maxilla, consists of a horseshoe-shaped portion called the body, and two perpendicular portions, called the rami, which are joined to the body at almost a right angle. The external face is marked in the midline by a slight crest, which marks the mandibular symphysis or junction between the two pieces that make up the bone in a fetus. The space between the chin and the mandibular angle is called the mandibular line. 5
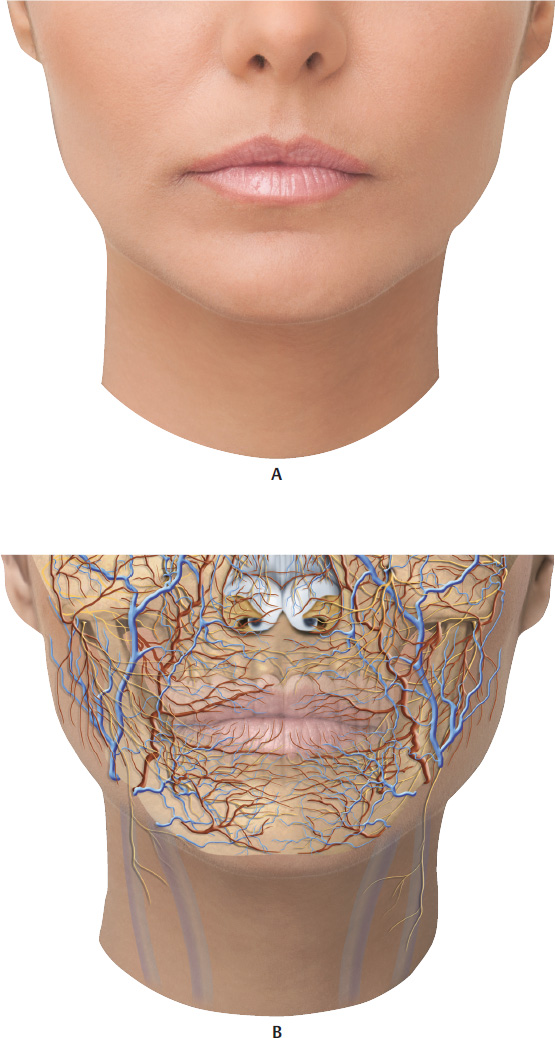
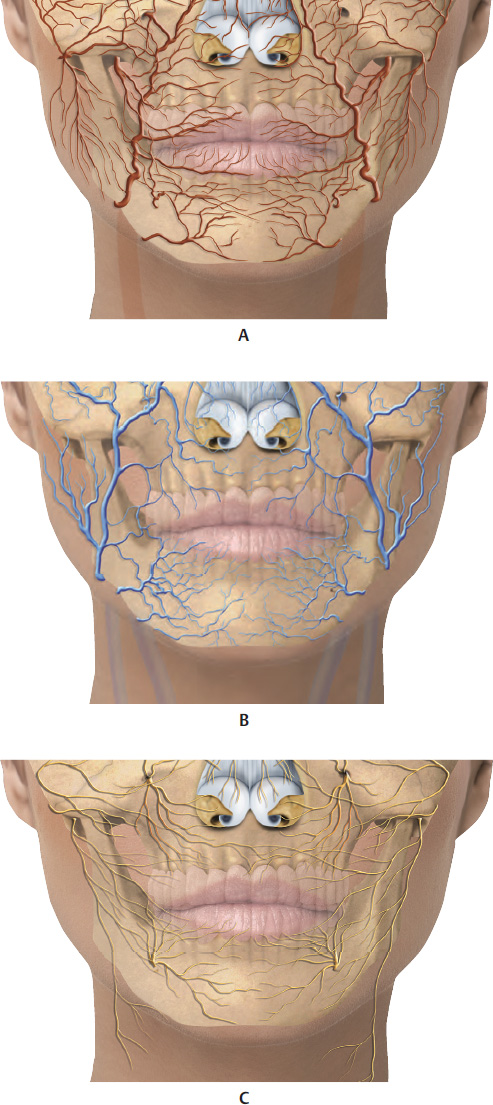
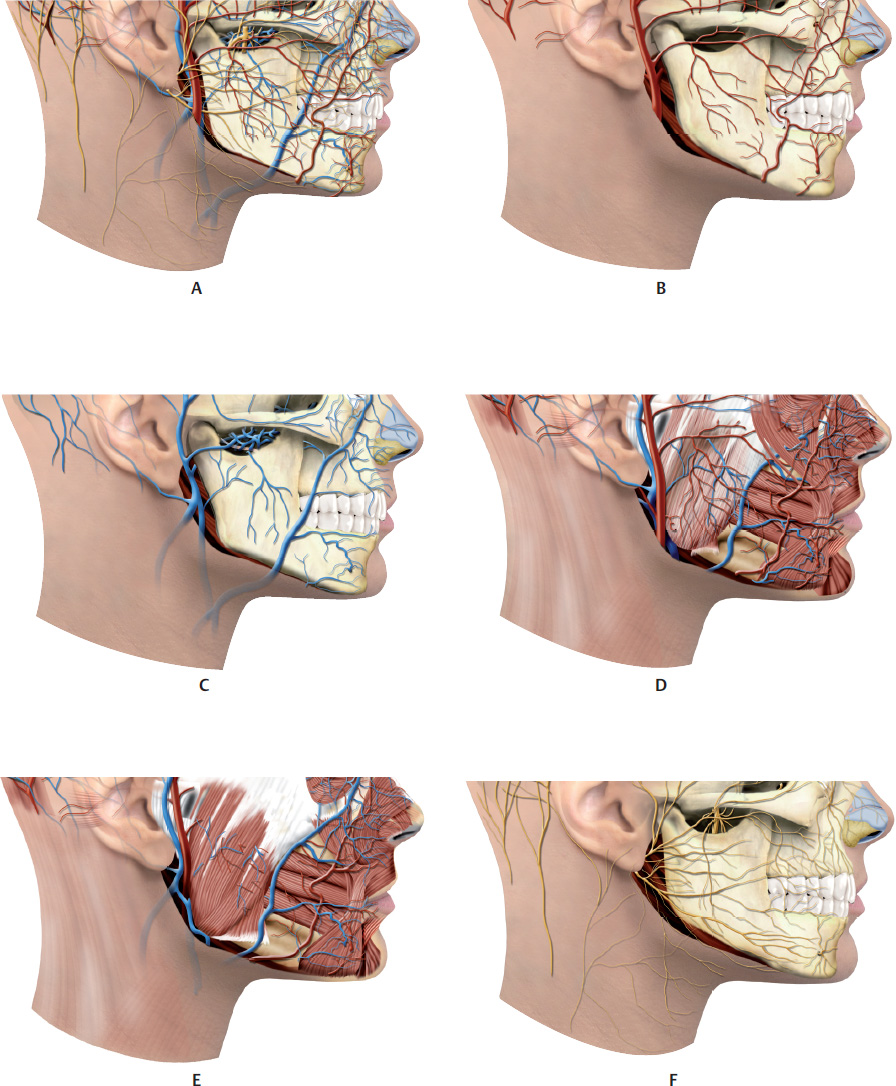
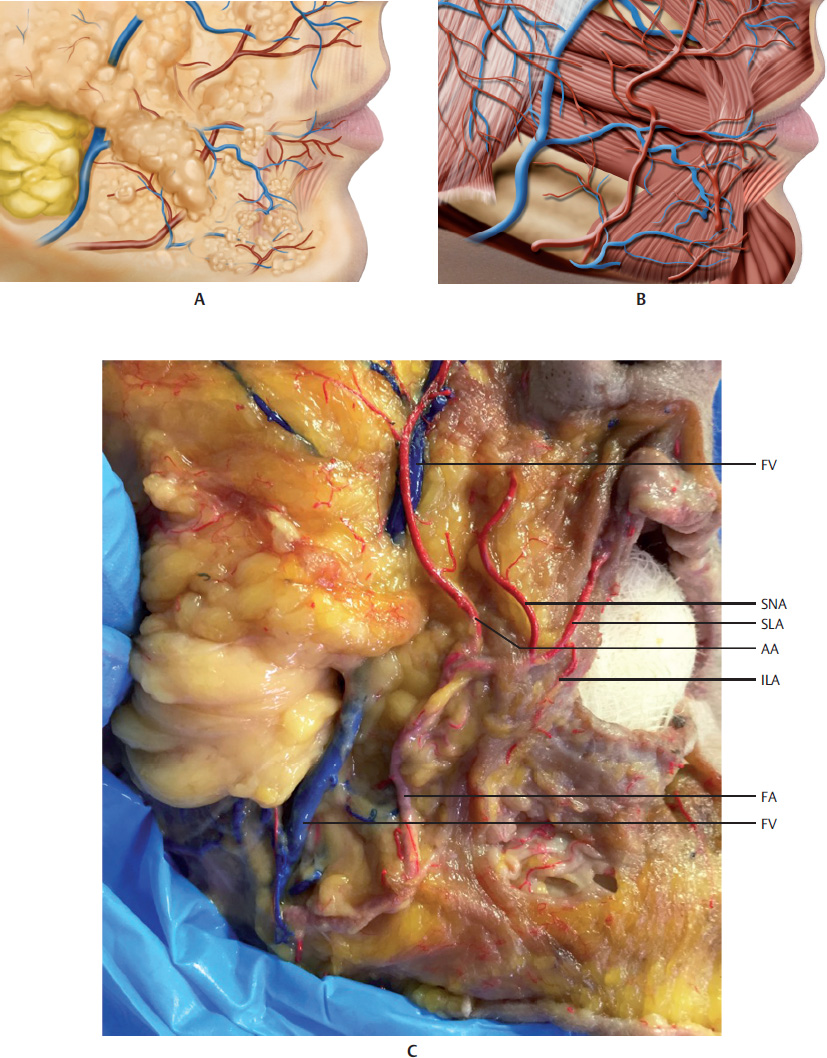
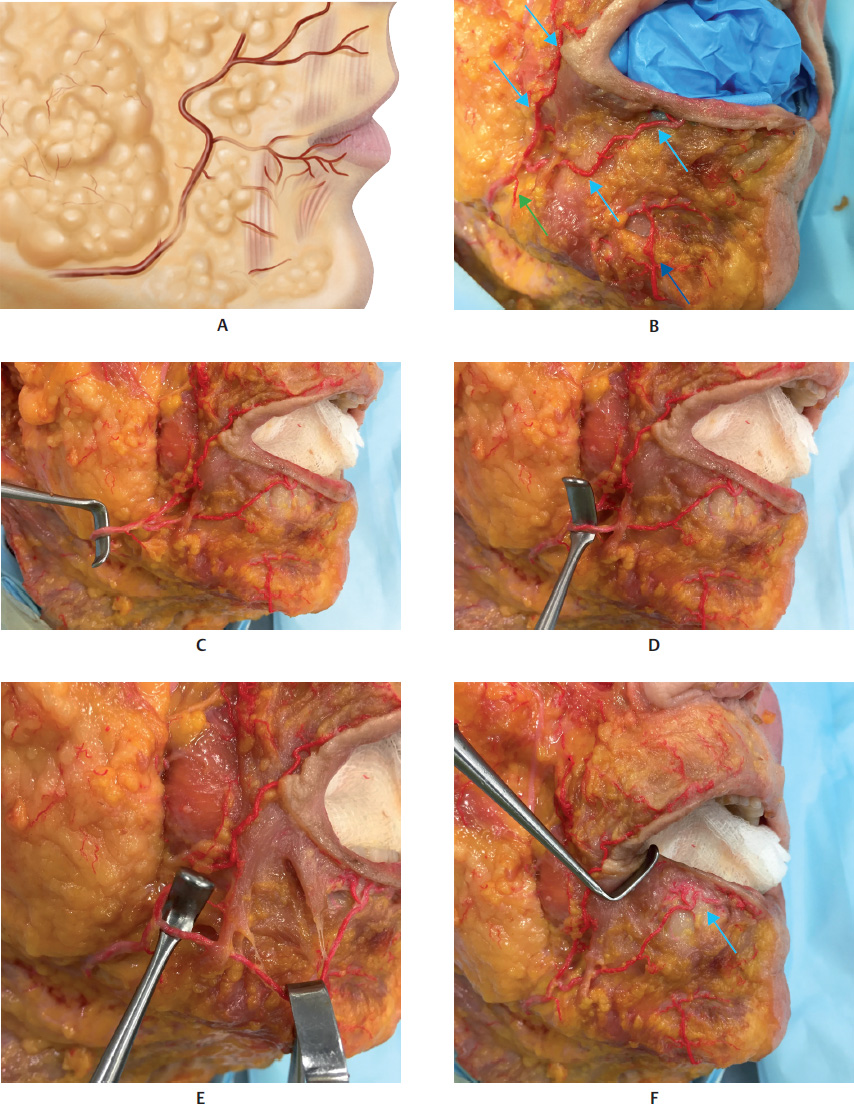
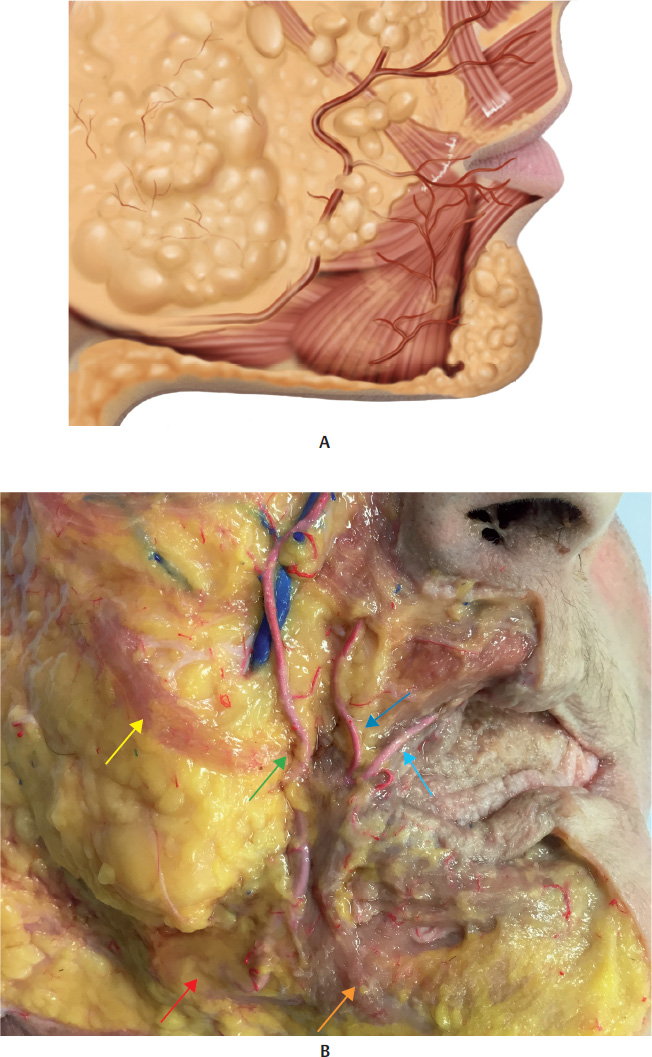
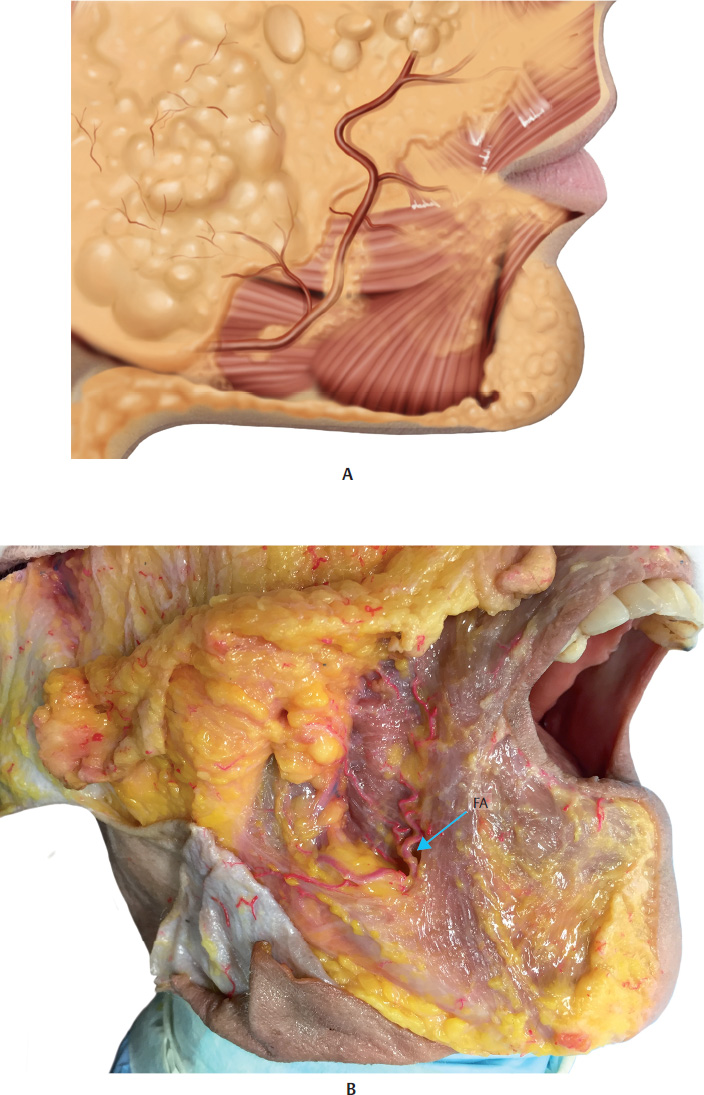
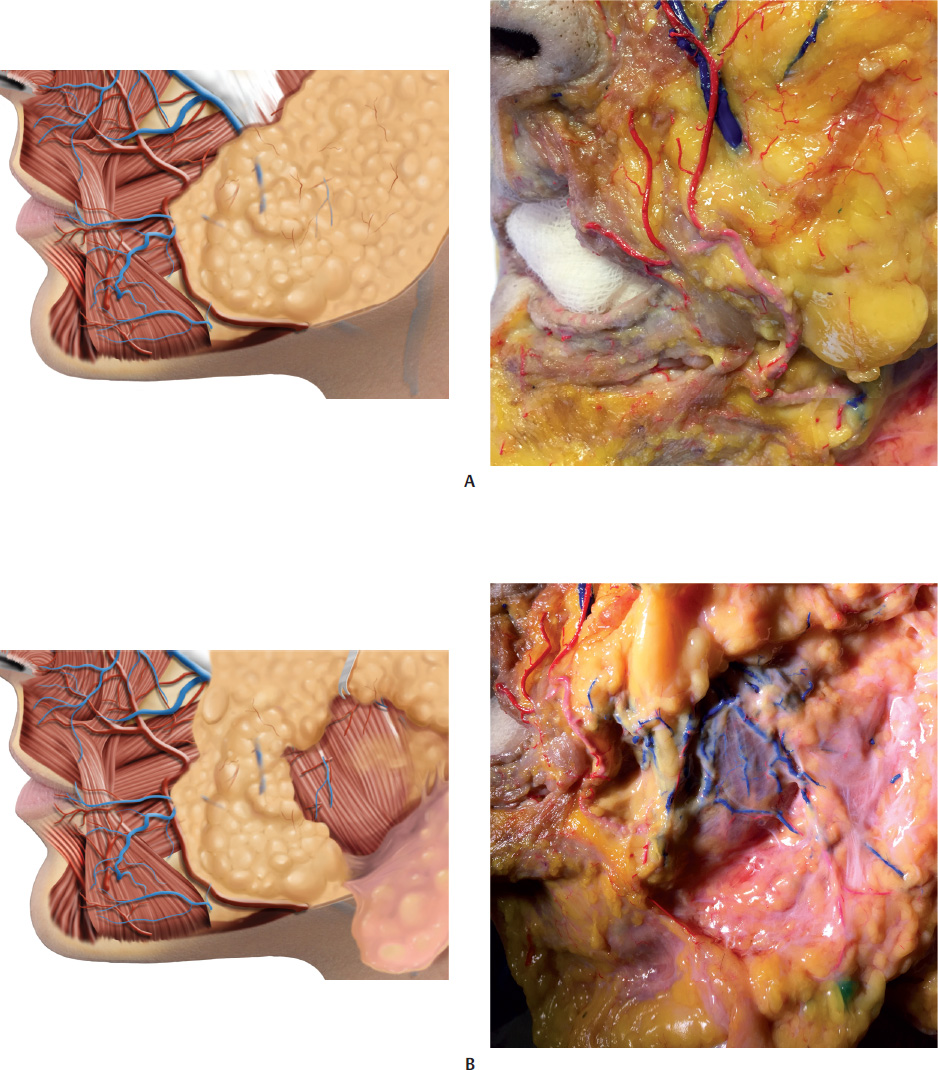
The lower teeth are located on the alveolar part of the man dible. The mental foramen (MF) is in the mandible, below the second premolar tooth; it allows for the passage of the mental nerve and vessels. The facial artery (FA) and facial vein (FV) course around the inferior edge of the mandibular body, and then pass ahead of the anterior edge of the masseter muscle. Their pulses can be easily felt at this point.
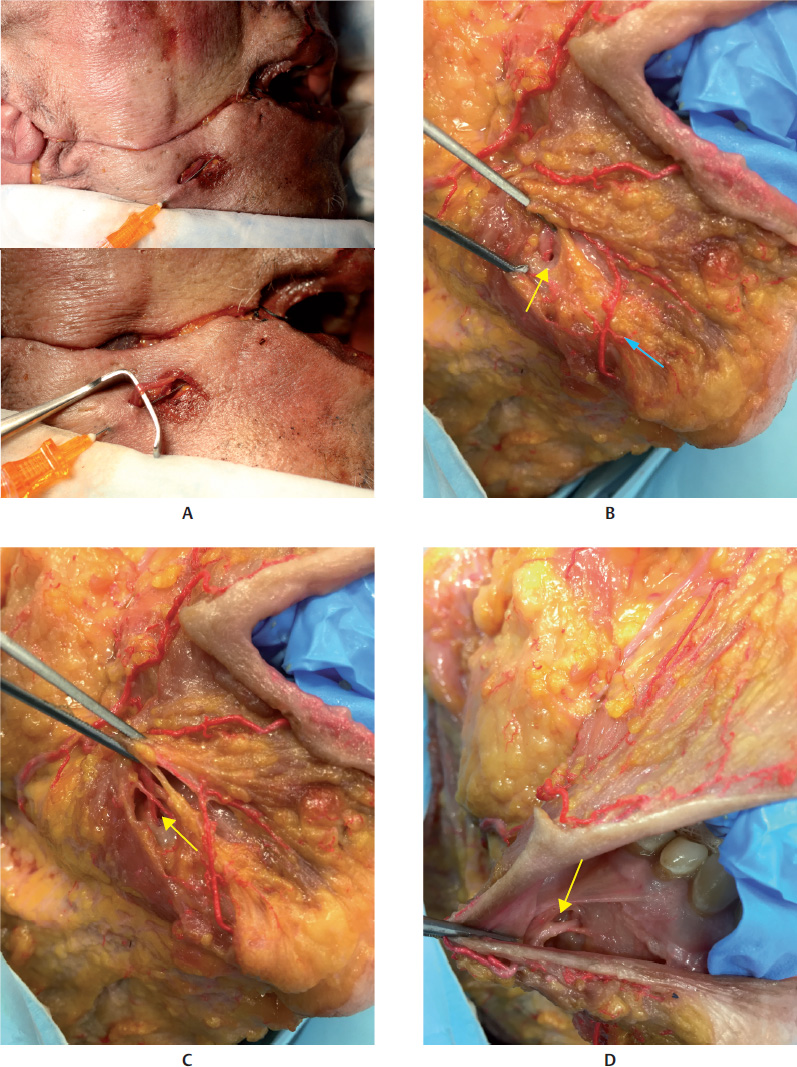
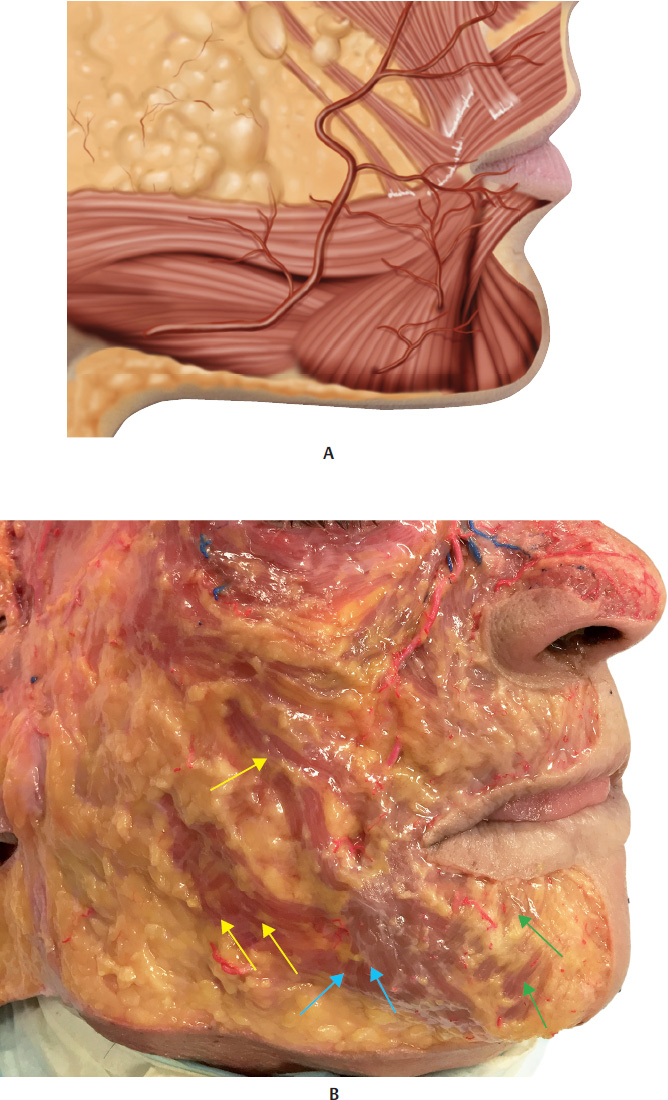
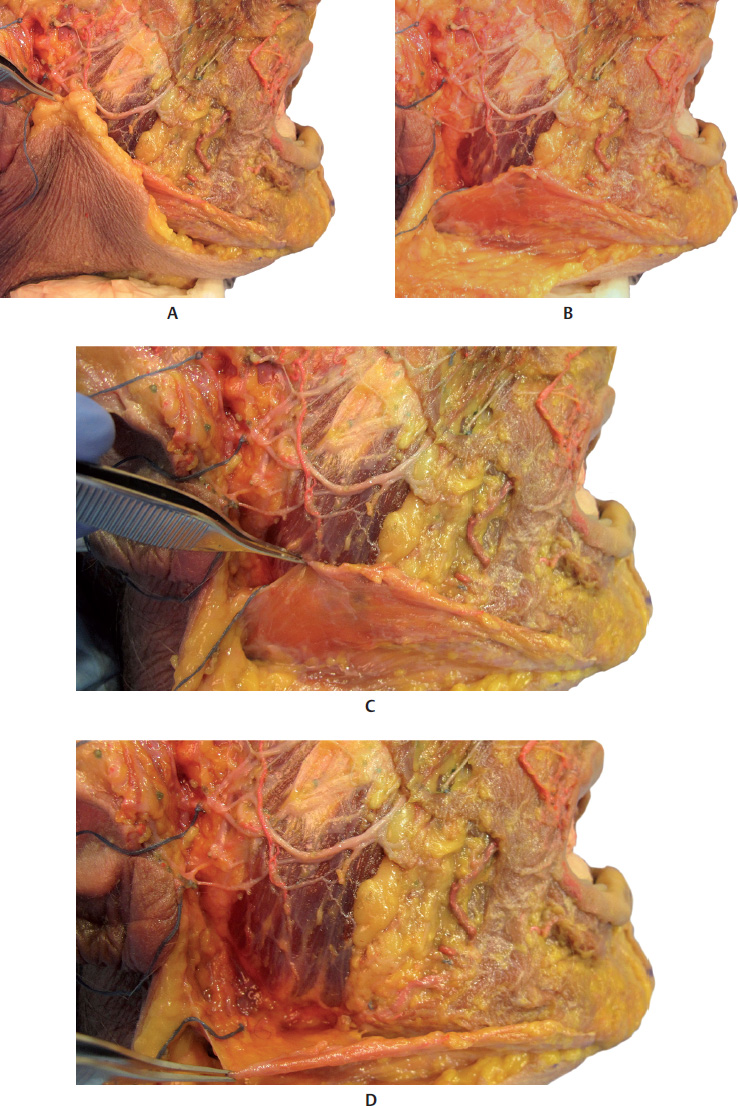
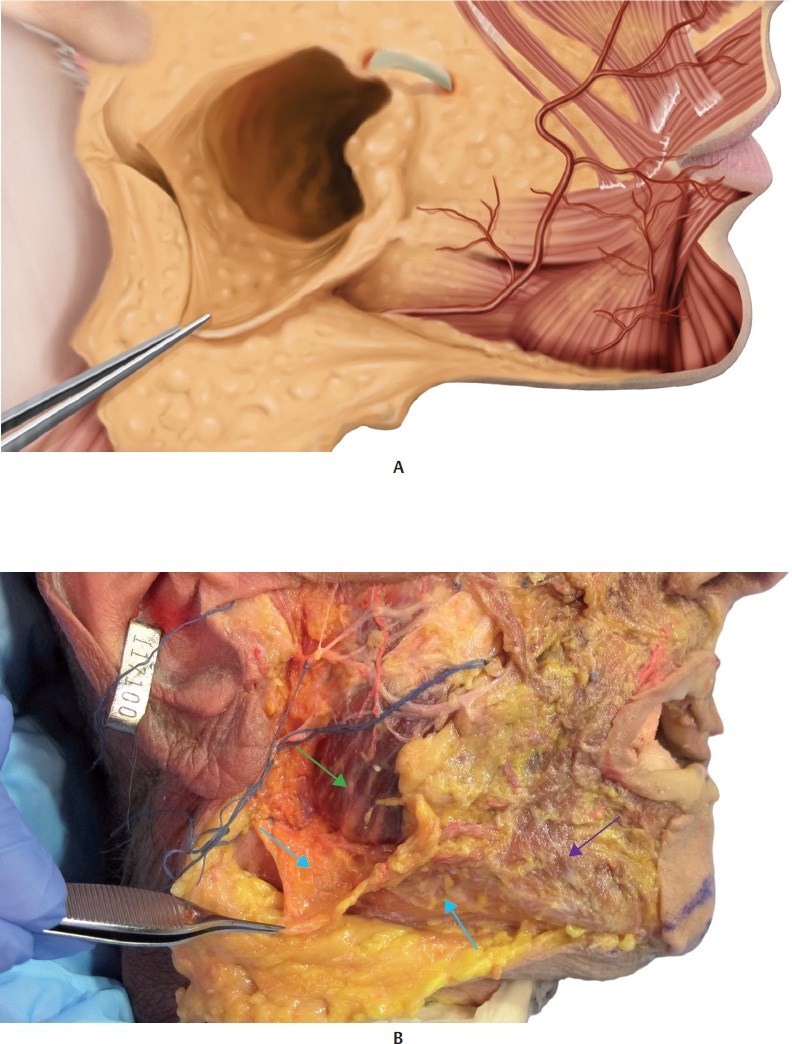
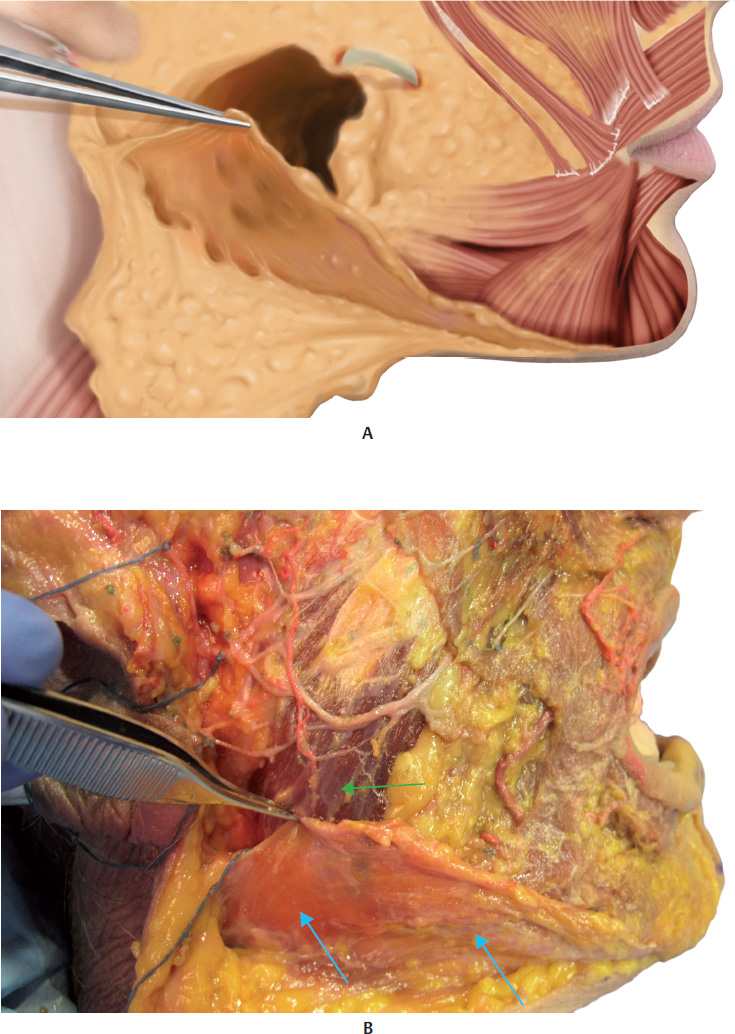
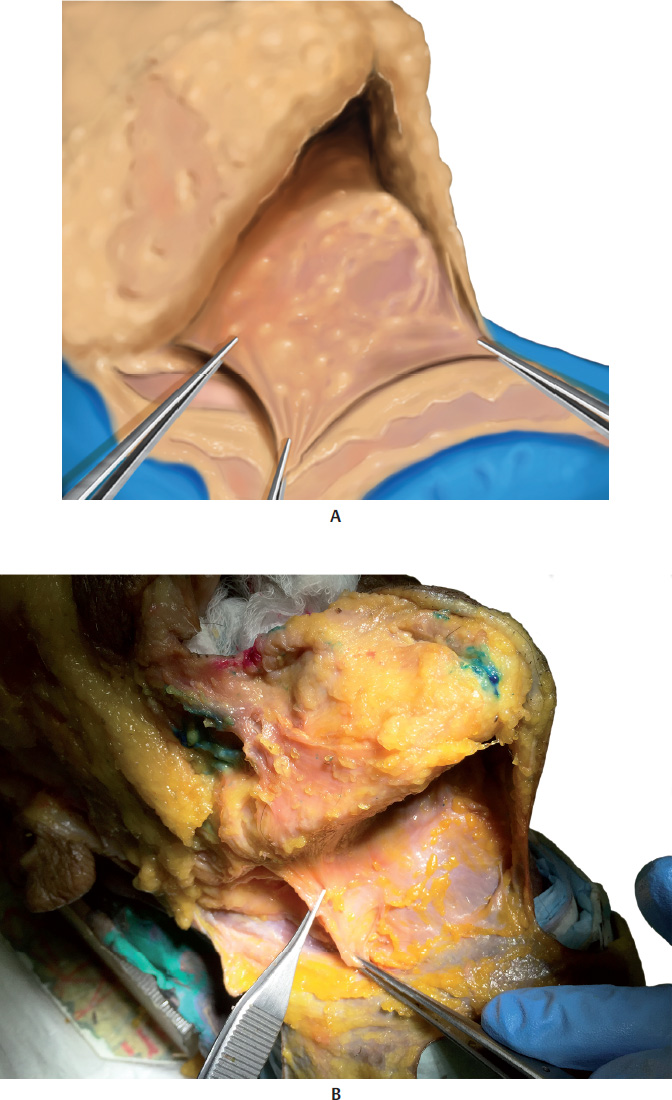
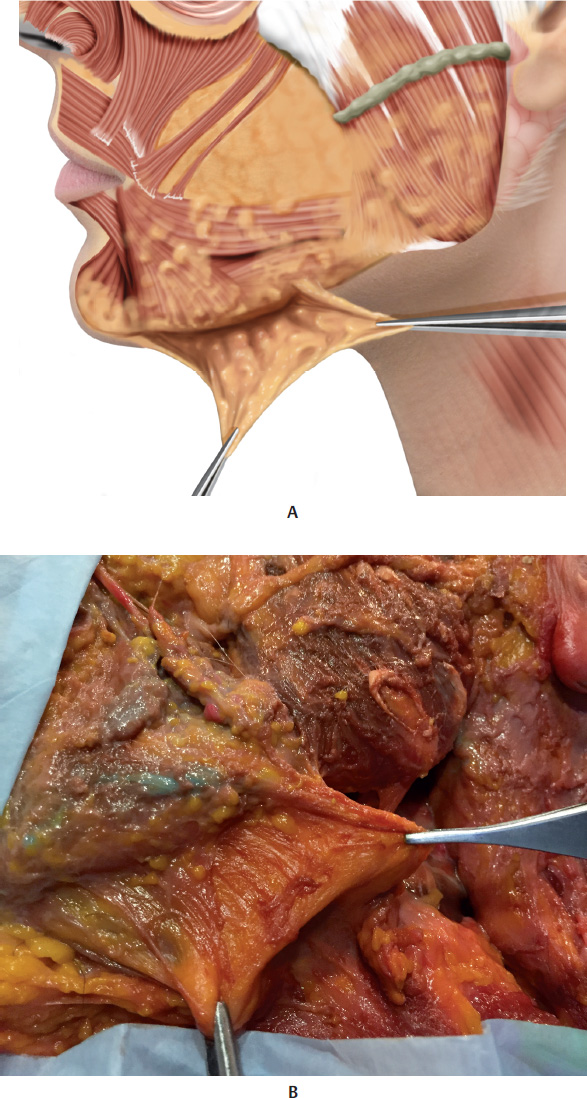
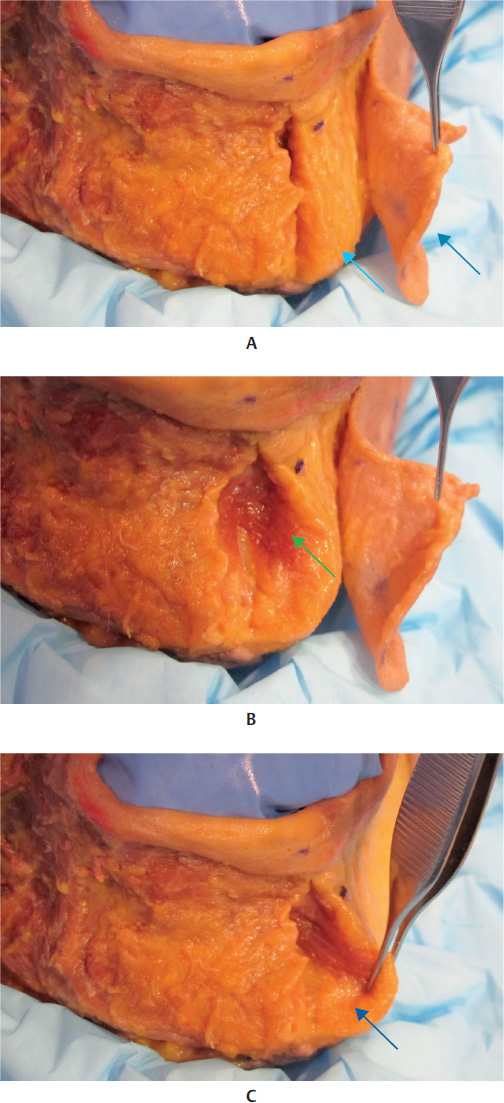
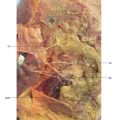
Reece, Pessa and Rohrich identified four clinically relevant fat pads in the mandibular region: two fat pads above the mandibular edge, called the superficial and deep mandibular fat pads, one submandibular fat pad, and another fat pad covering the parotideomasseteric fascia (temporolateral). A membranous septum separates the two fat pads located above the mandibular edge of the submandibular fat pad, and is called the mandibular septum. Anteriorly, this is a continuation of the mandibular ligament, which can then be found behind the depressor muscle of the angle of the mouth (DMAM) before it inserts into the skin. The fibers of the platysma muscle entwine with the mandibular septum and adhere to the anterior edge of the mandible. 6 –. 8
The aging process of the mandibular contour is caused by different mechanisms: atrophy of the superior and inferior mandibular fat pads, with the impression of accentuation in the submandibular fat pad, dehiscence of the mandibular septum with ptosis of the superior and inferior fat pads toward the neck, bone resorption, and flaccidity of local skin (Fig. 17.1–17.20,17.23,17.24, and17.43).
Technique
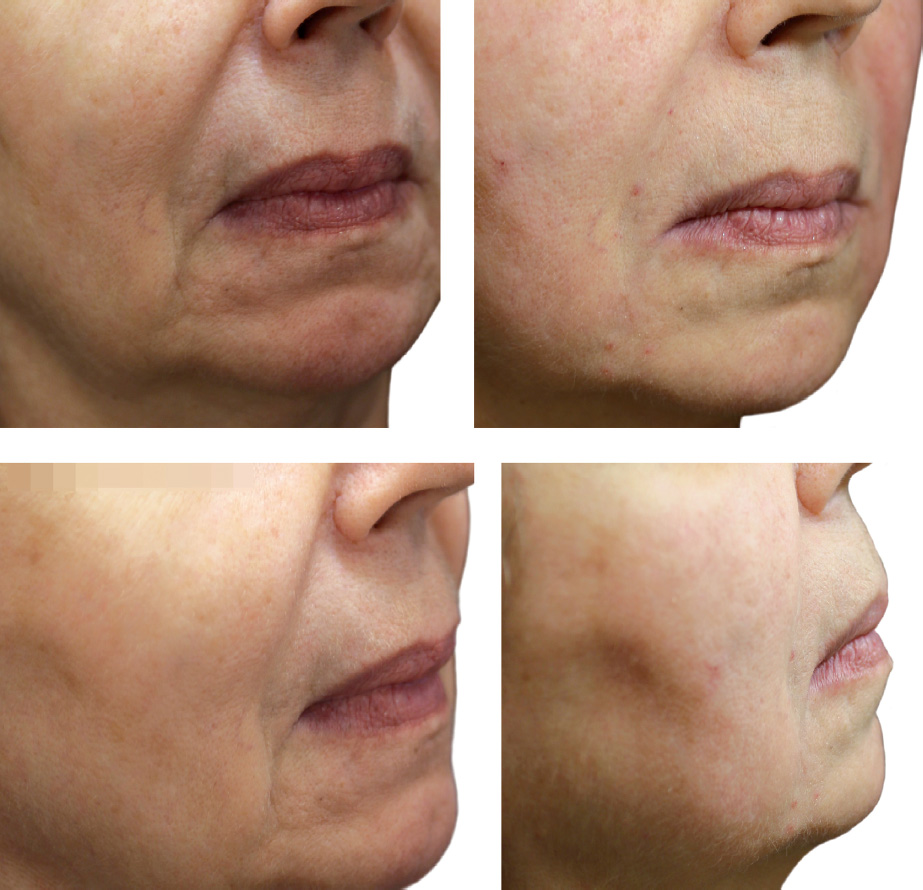
The ideal candidates for this technique include individuals with slight to moderate loss of facial contour. The procedure can also be performed on male patients, to reinforce a region that expresses virility. This augmentation is also indicated for women who have a heart-shaped face, when the wish is to emphasize the lower limit of the face.
For the chin area, the most suitable candidates are those who since youth have needed a chin augmentation (brachyfacials or profile class II) and are reluctant to have definitive implants. Patients who over the years have suffered a change in the format of their chins and require rejuvenation and redefinition of this area are also suitable as candidates.
We prefer to use microcannulas for filling this area. 9 ,. 10 Mi crocannulas have a blunt tip, which offer greater safety as they reduce the risk of injuring vessels and nerves, although the procedure is not completely free of complications: 22 G and 25 G cannulas measuring 40 to 50 millimeters in length are indicated for injecting more viscous HAs, which are considered to bevolumizers.Another important advantage of microcannulas is that the injector can precisely locate the correct injection plane, which is the subdermal plane, and in some cases, the supraperiosteal plane. The blunt tip of the microcannula, which has no cutting capacity, cannot penetrate the dermis, but slides easily in the subdermal plane. Although the areas to be corrected and the respective treatment techniques are described separately, one must not forget that two or three regions can be combined at the same time.
We use three different techniques for treating the mandibular contour depending on the patient’s needs. These are described below.
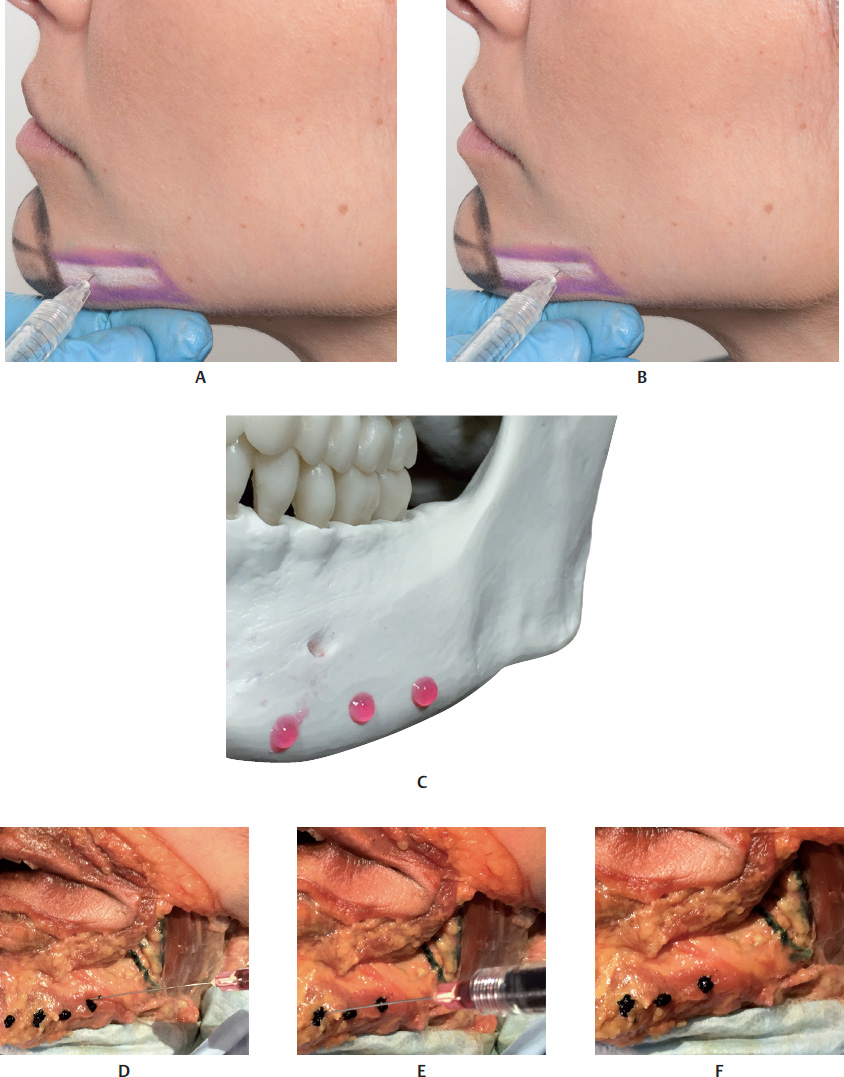
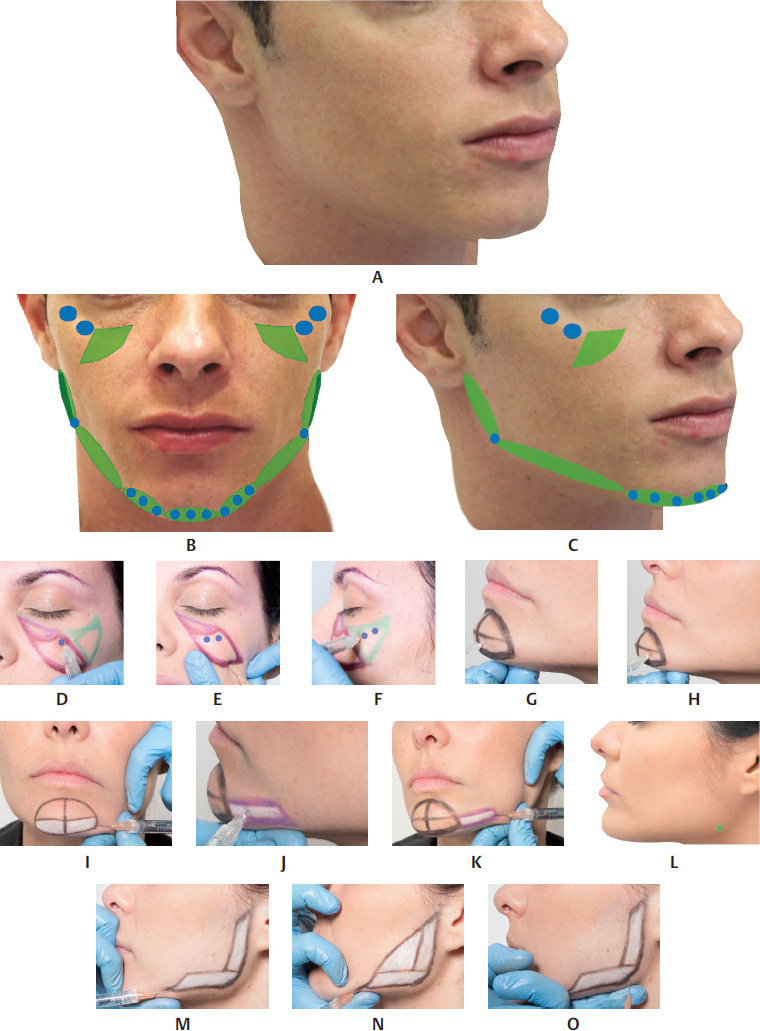
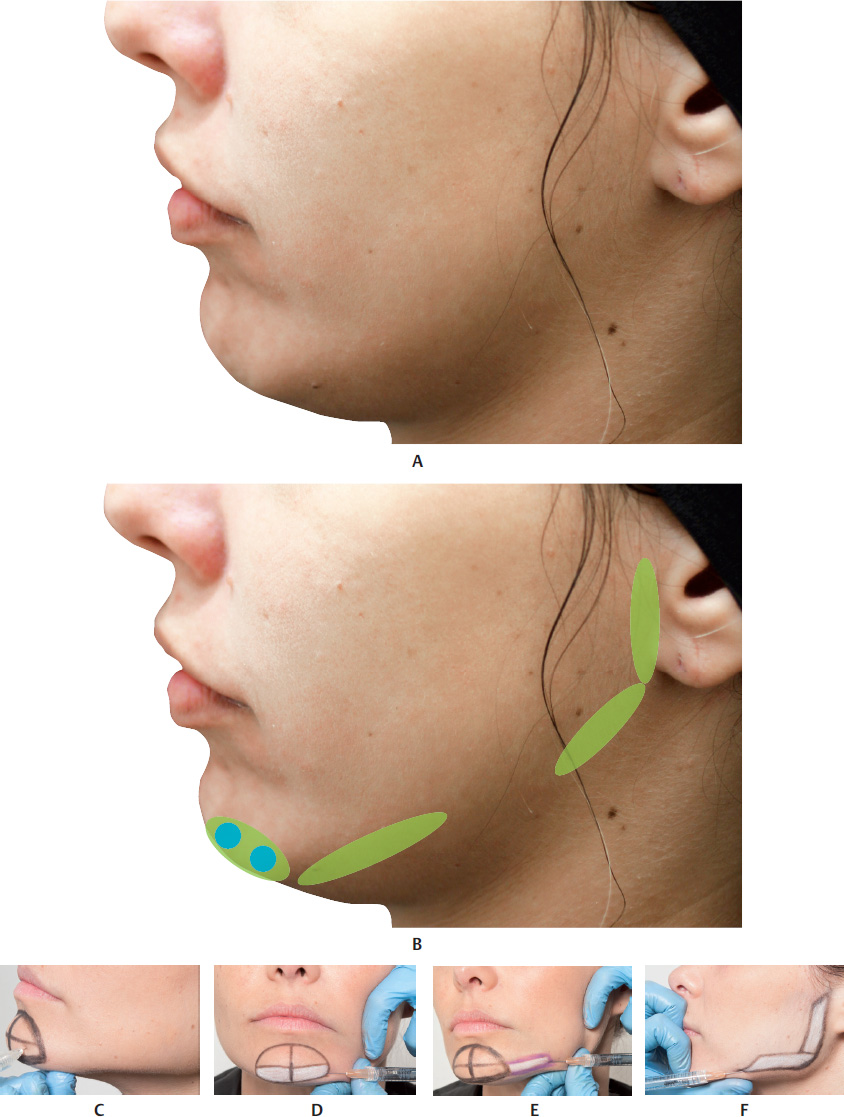
Filler Injection of the Mandibular Angle and Mandibular Ramus
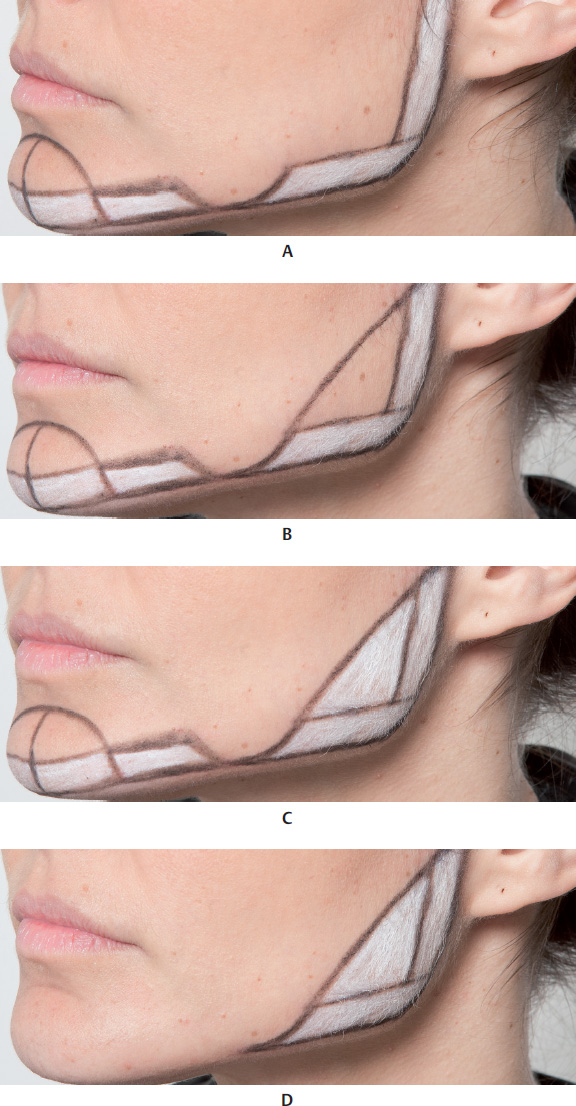
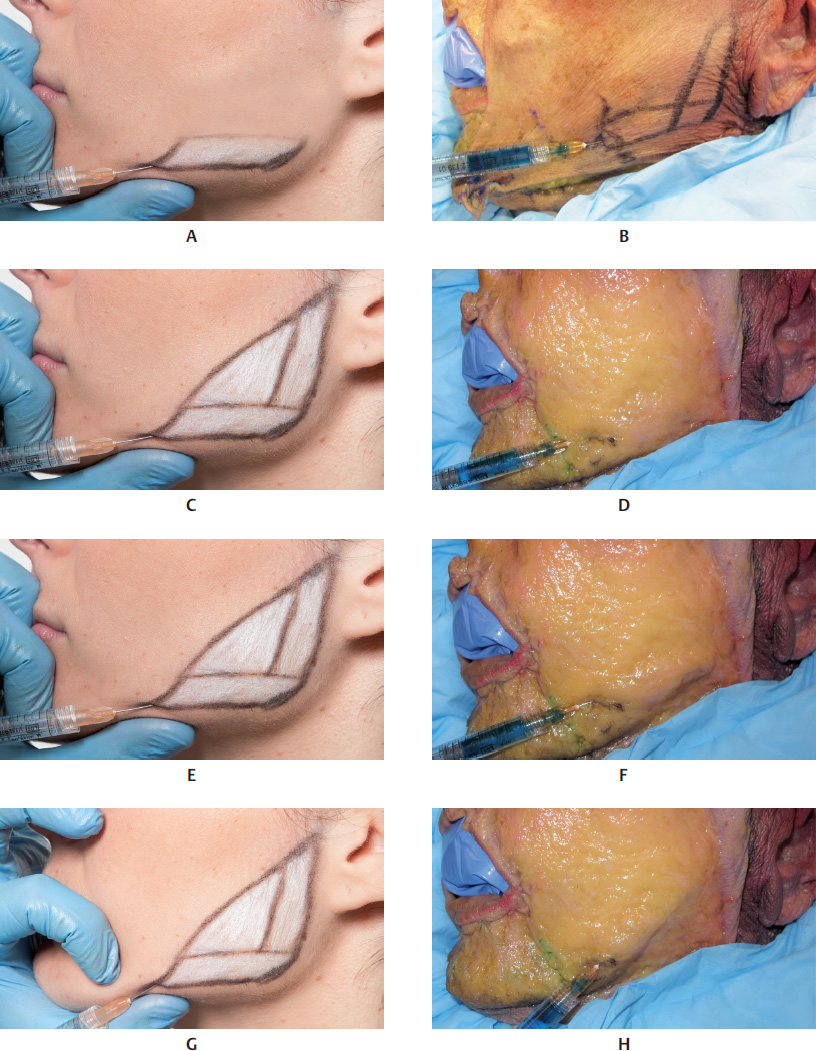
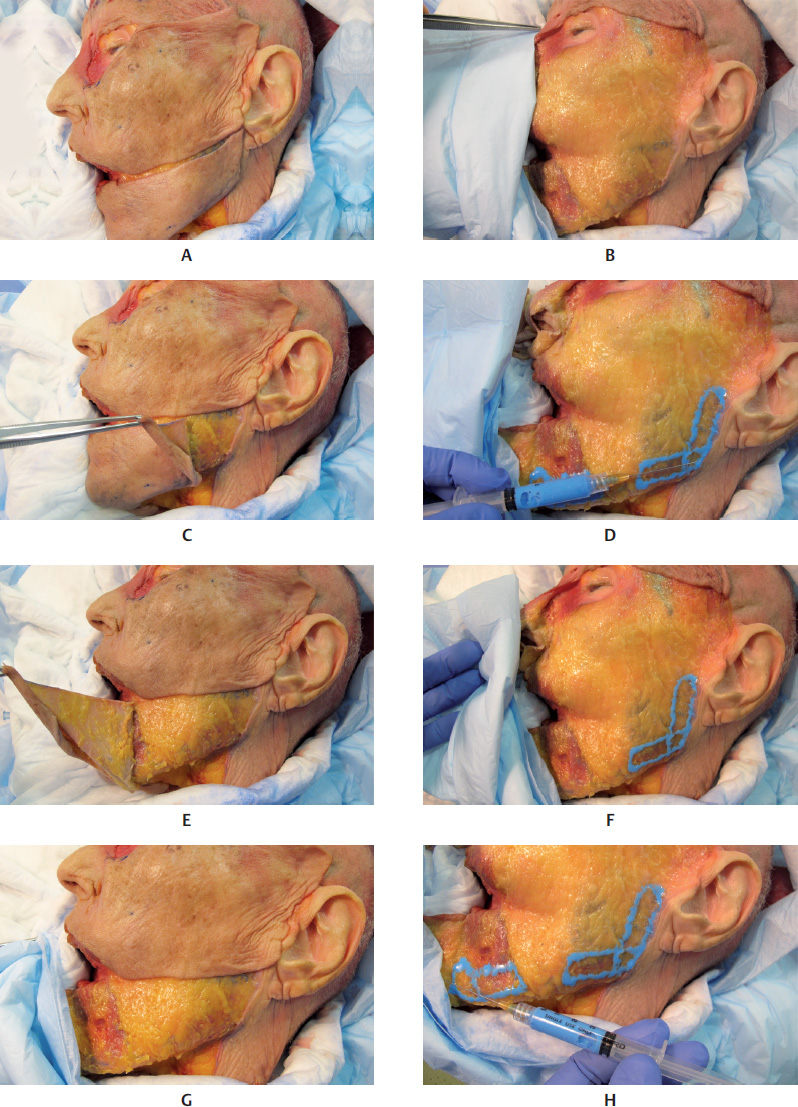
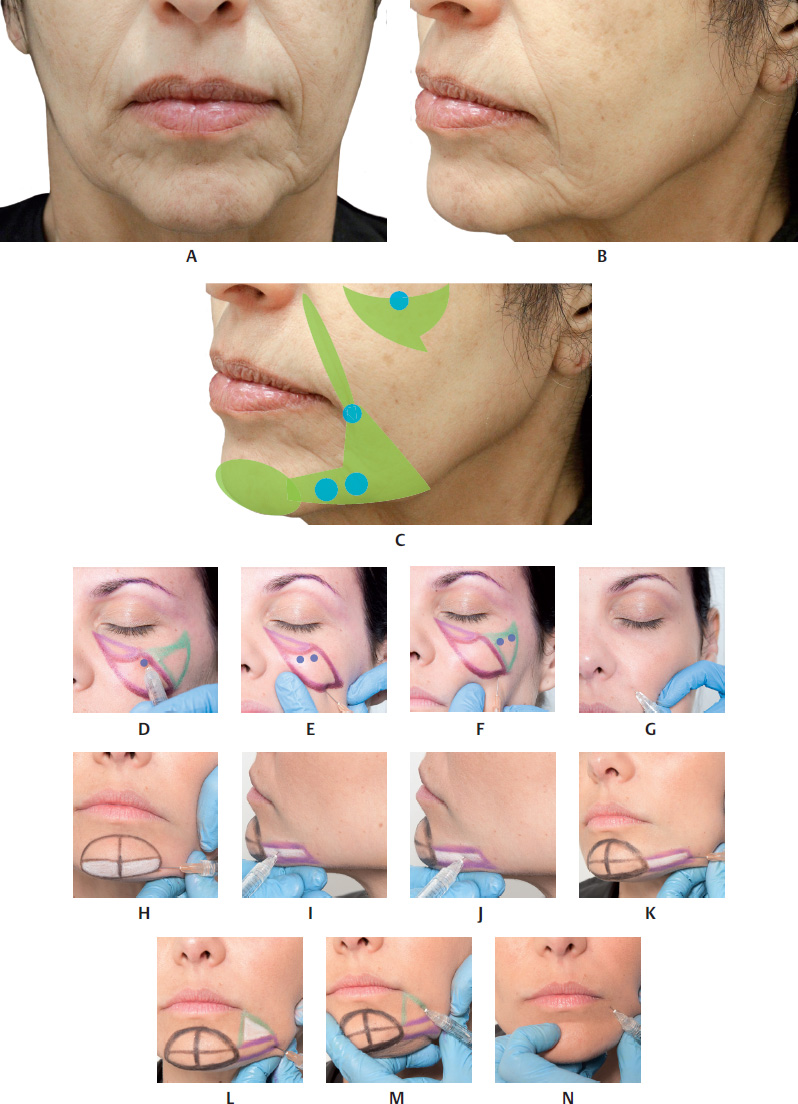
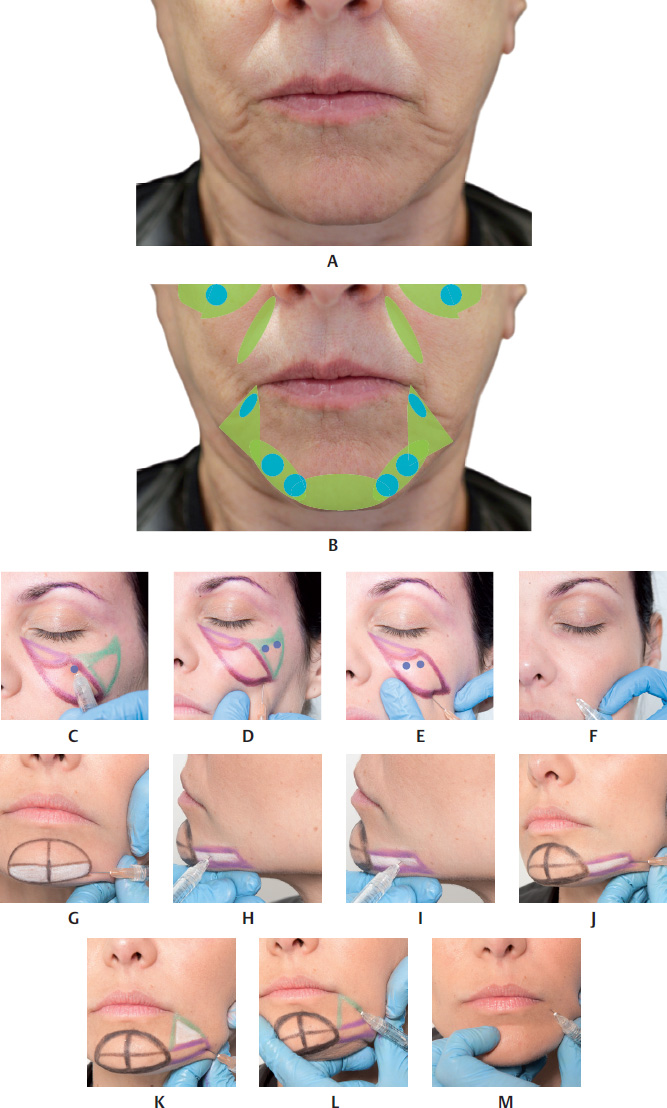
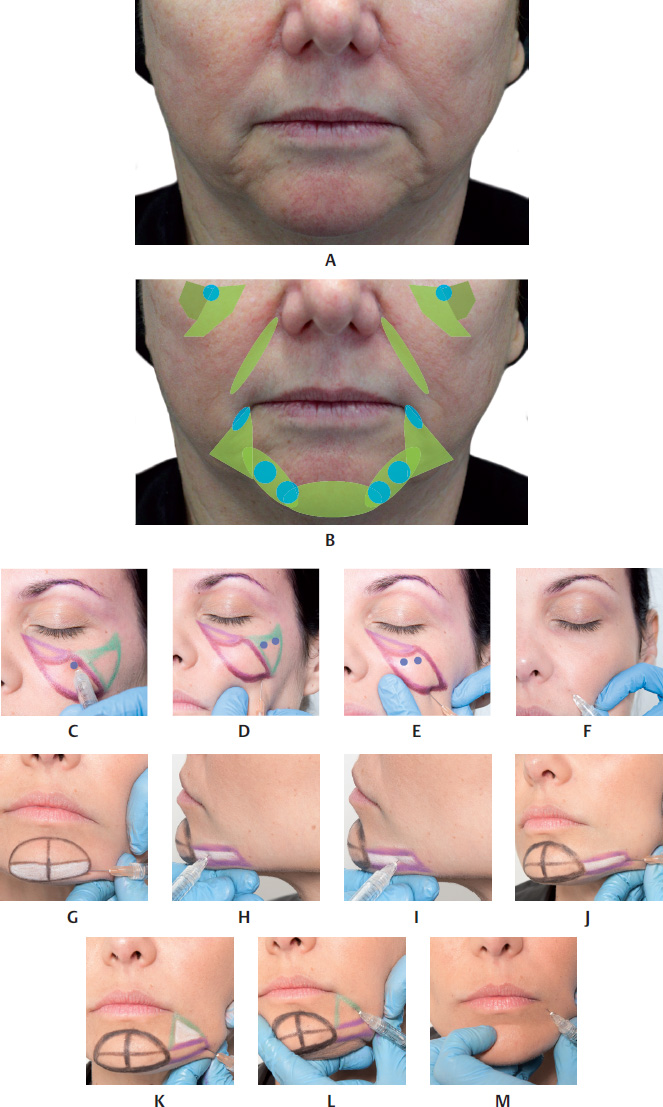
To mark the area, palpate the mandibular angle and draw two lines measuring approximately 3 cm from the mandibular angle: one on the body and one on the ramus. Then, draw a line joining the two extremities, marking the upper limit of the area to be filled.
Create an orifice with a 21 G needle, inserting the bevel very superficially, just enough to pass the fibrotic tissues of the dermis. The entry point can be made in two places: the mandibular angle or at the end of the horizontal line. The injector must pay particular attention because the FA courses along the inferior edge of the body, in front of the anterior margin of the masseter muscle. Insert the microcannula up to the mandibular angle in the subcutaneous plane, where HA should be injected with a retrograde injection. Then, change the direction of the microcannula so that it points toward the mandibular ramus, in the subcutaneous plane, and perform a retrograde injection of the product, filling the previously marked area. After filling, mold the area treated by exerting pressure with the index finger against the mandibular bone (Fig. 17.22,17.39,17.40, and17.42).
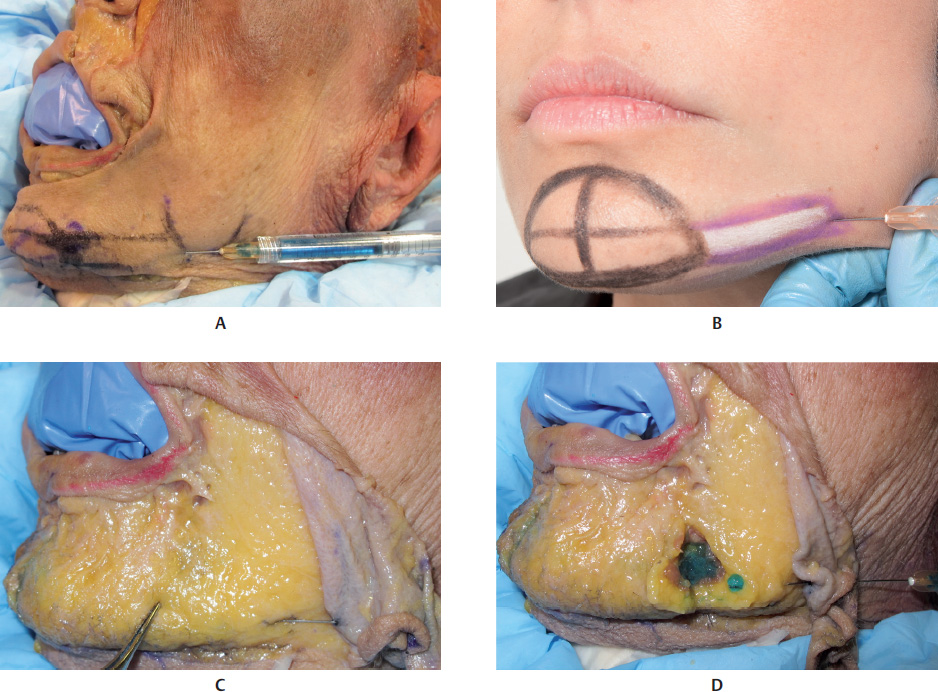
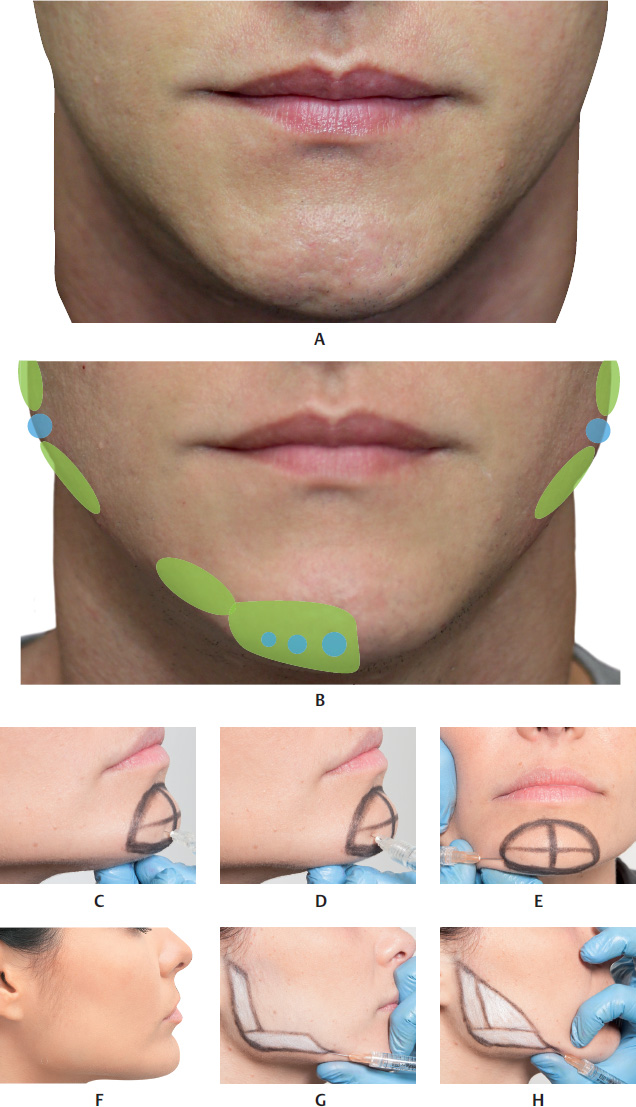
Redefining the Mandibular Line
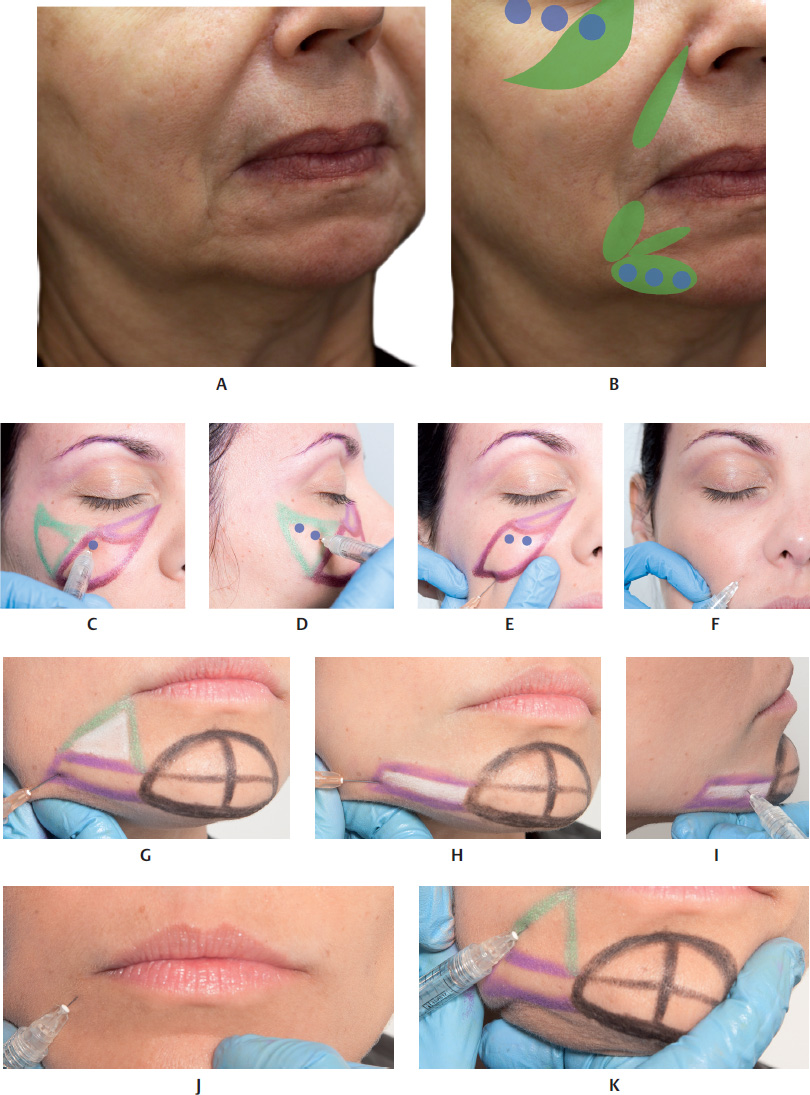
To redefine the mandibular line, mark around the area of ptosis on the mandibular line that is the cause of flaccidity of the skin or movement of the fat pad. After marking the area of ptosis, which should not be filled, draw two parallel horizontal lines marking the mandibular contour up to the mandibular angle. Then, apply an anesthetic bleb (optional) and make an orifice at the site indicated by inserting the abovementioned microcannula in the direction of the mandibular angle, in the subcuta neous plane, and inject the product via retrograde injection. If it is necessary to increase the length of the face, the region below the mandibular septum should also be filled. The filled area should then be molded by exerting moderate pressure (Fig. 17.21,17.22,17.37, and17.38).
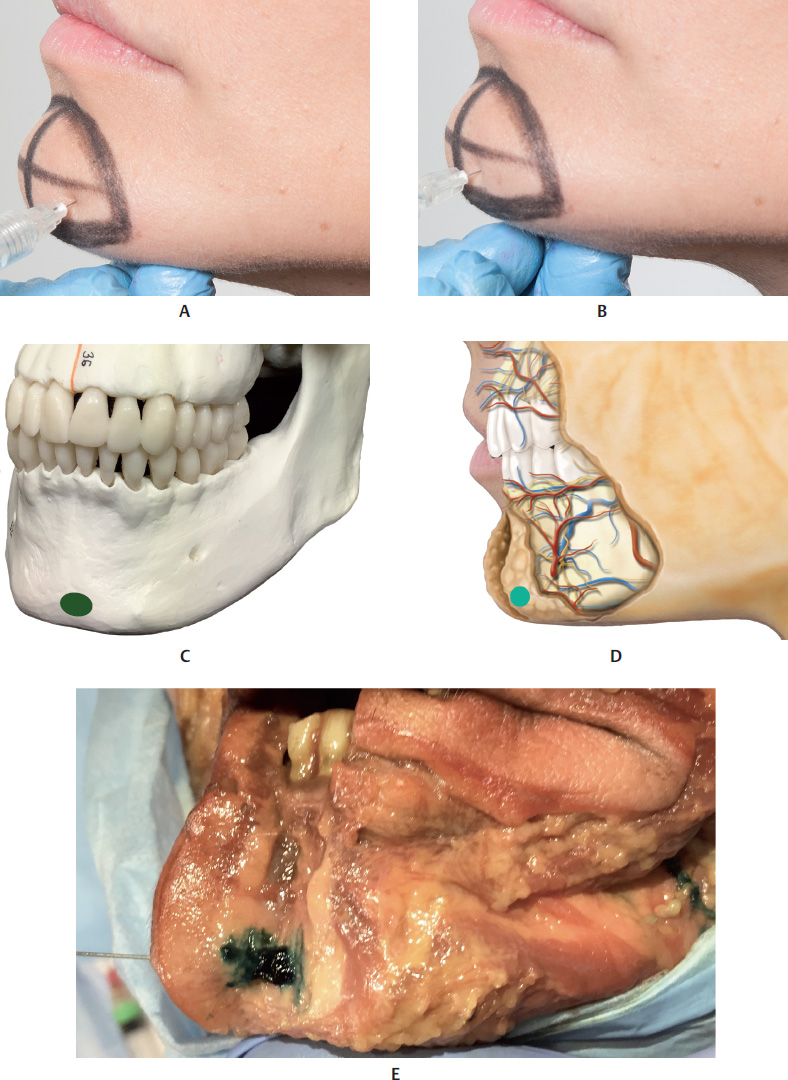
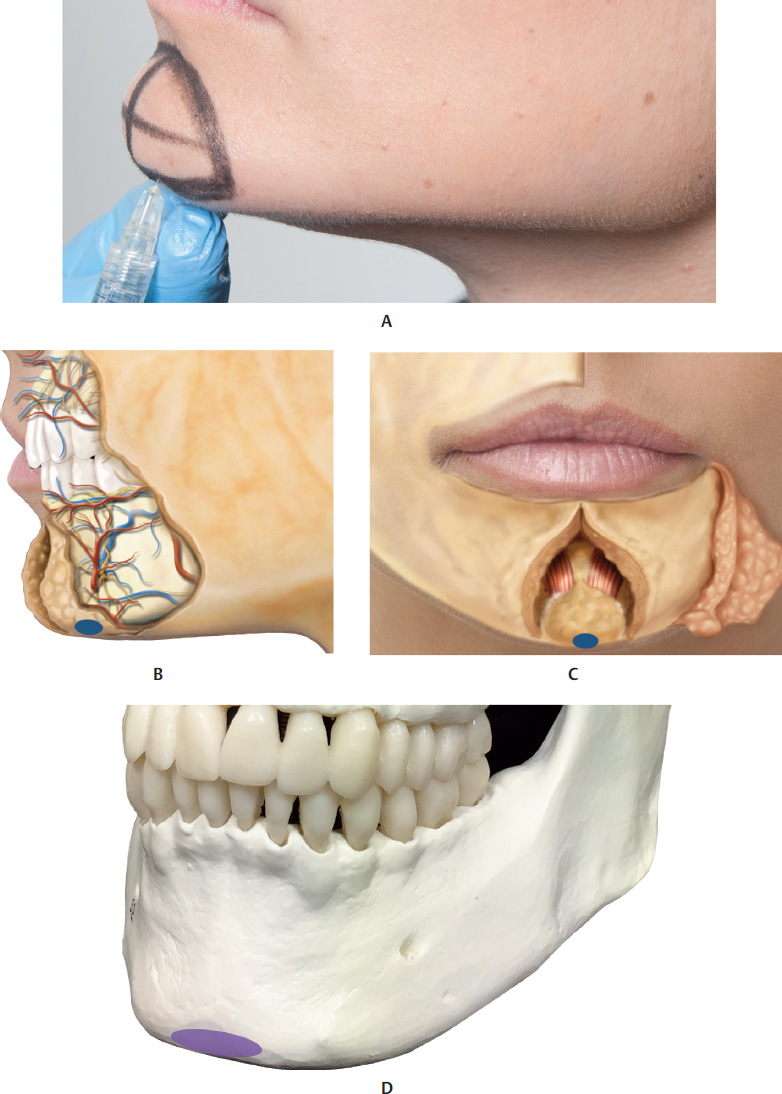
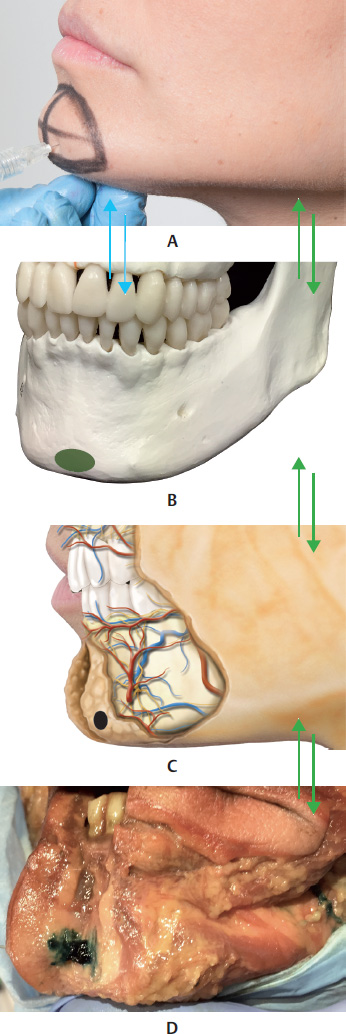
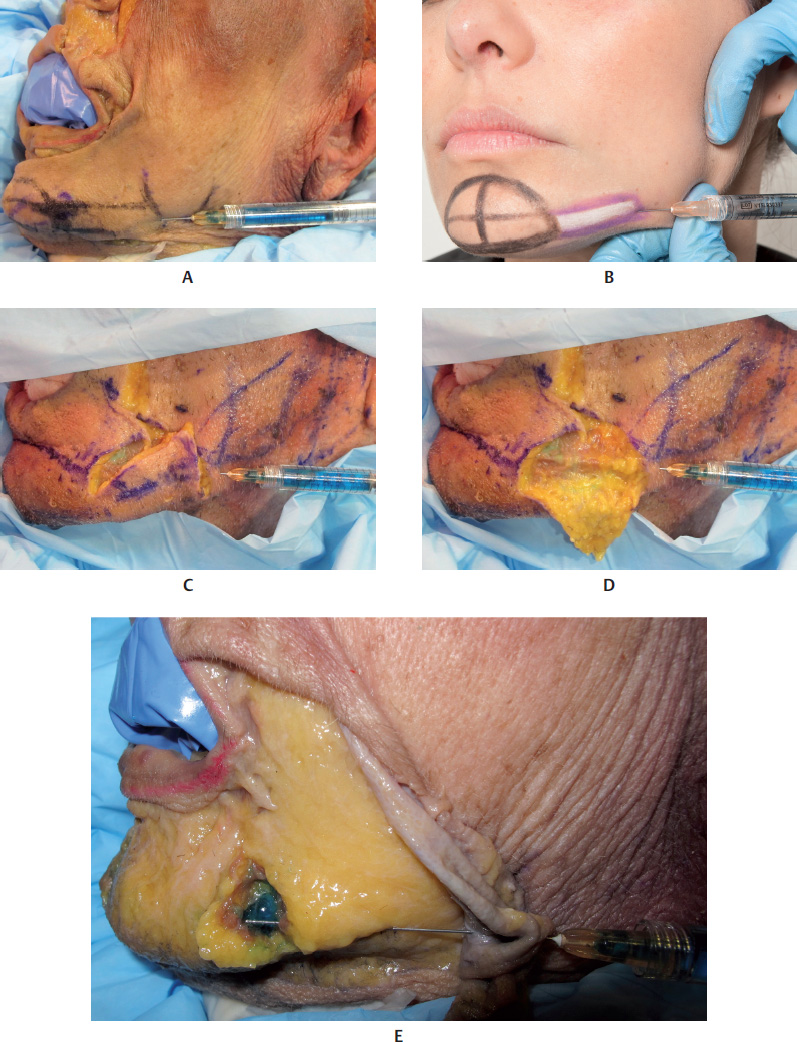
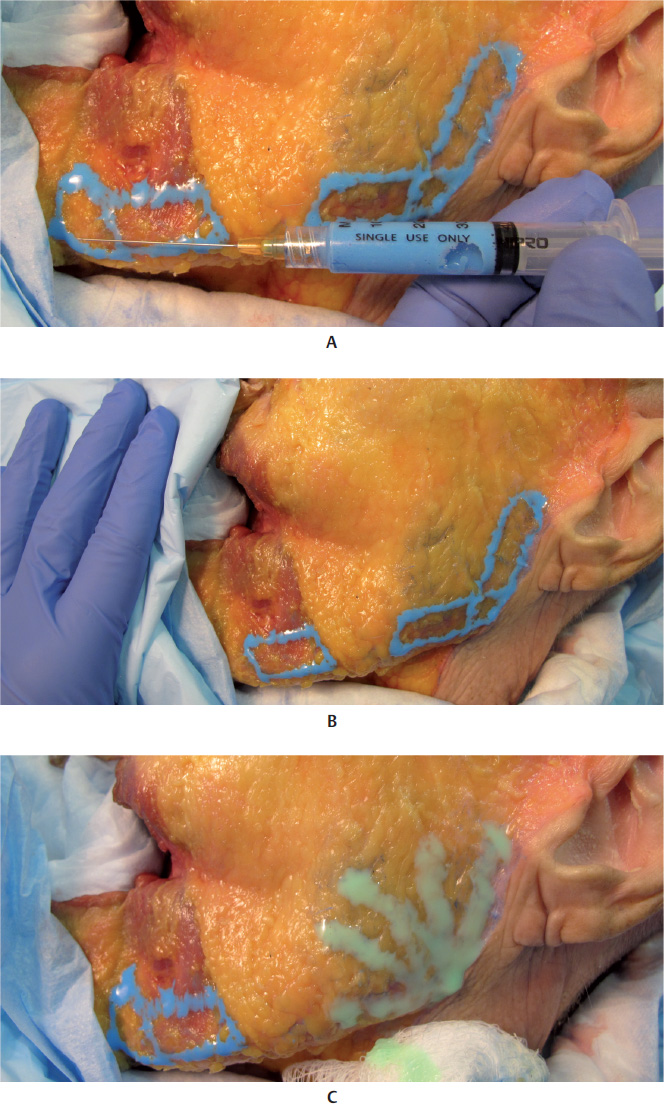
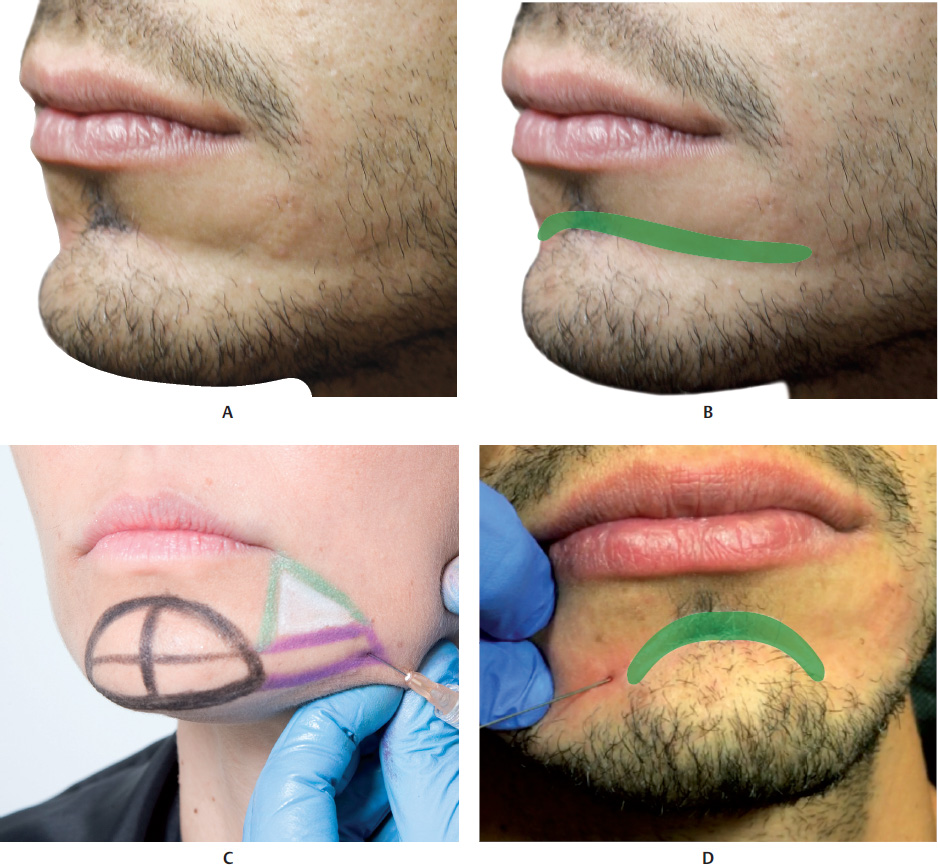
Lateral Mental Region
In some people, aging causes lateral volume loss in the mentalis muscle, and this worsens with the loss of dermal collagen with ptosis caused by the subcutaneous fat shifting.
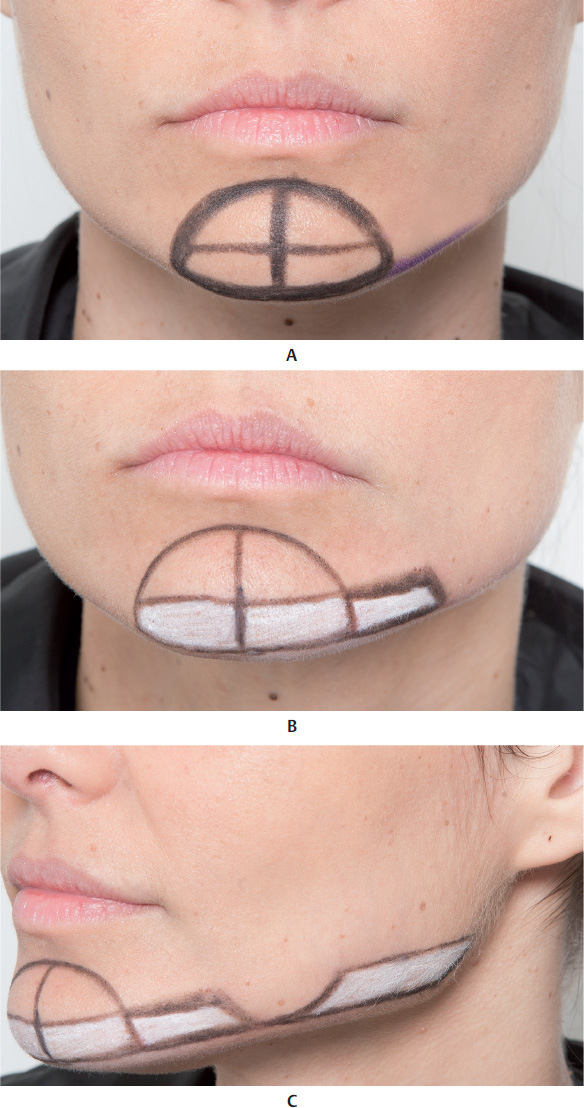
To mark the region to be filled, draw a semicircle on the mental region and another semicircle on the area affected by ptosis on the mandibular line. Draw a line on the mandibular edge joining the two abovementioned markings, and 2 cm above that, draw another parallel line, delimiting the space to be treated.
For filler injections with a microcannula, apply an anesthetic bleb (optional), create an orifice with the needle and then introduce the microcannula between the two parallel lines and f ill the space marked with a retrograde injection technique. Finally, mold the filler by exerting pressure with your index finger against the mandibular bone. This filler injection is applied above the periosteum in the deep subcutaneous plane (Fig. 17.21,17.22,17.31–17.35, and17.41).
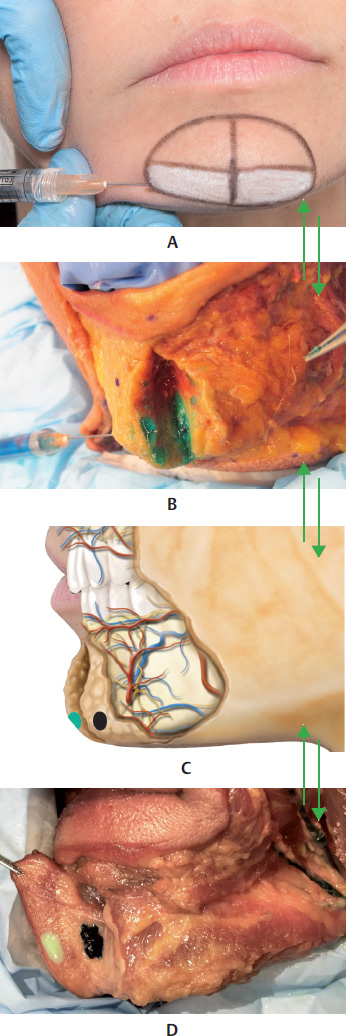
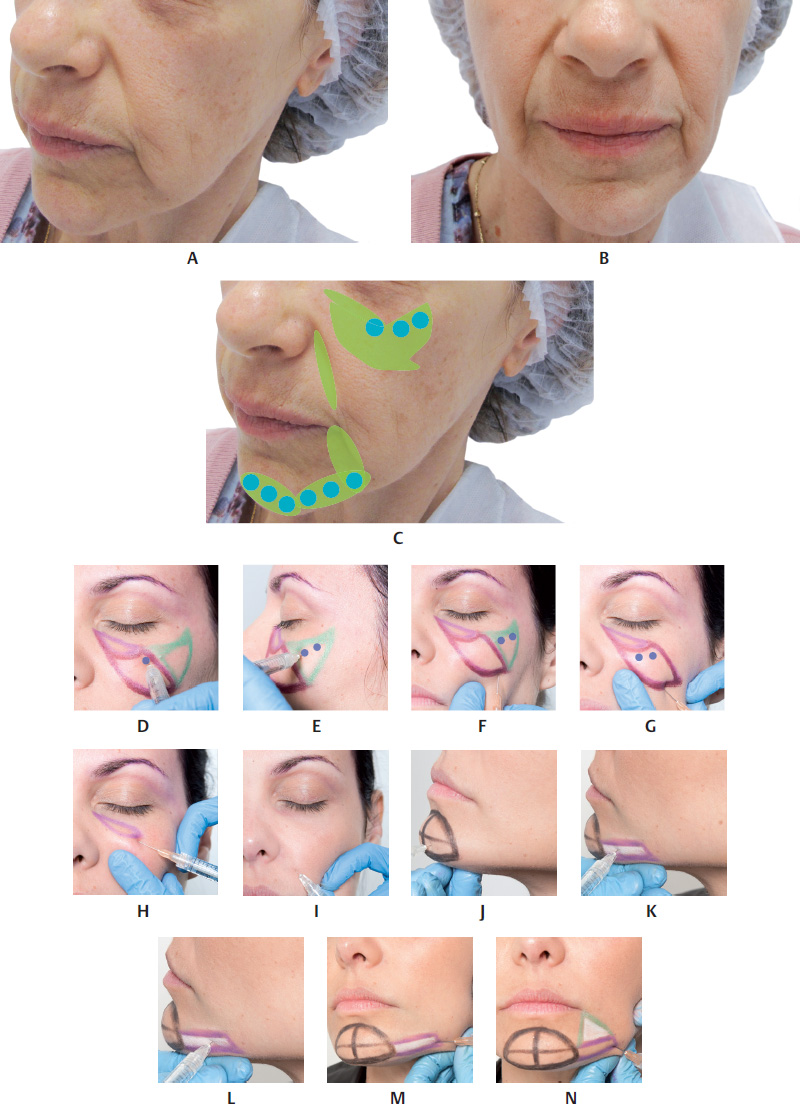
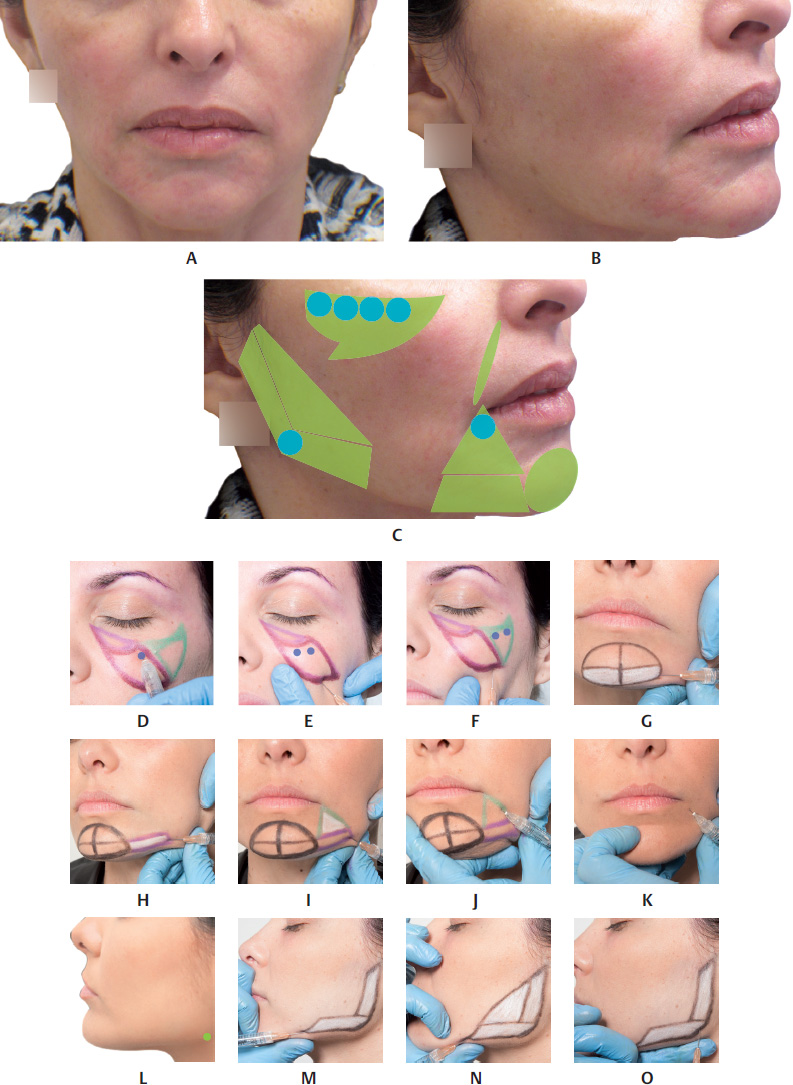
Chin
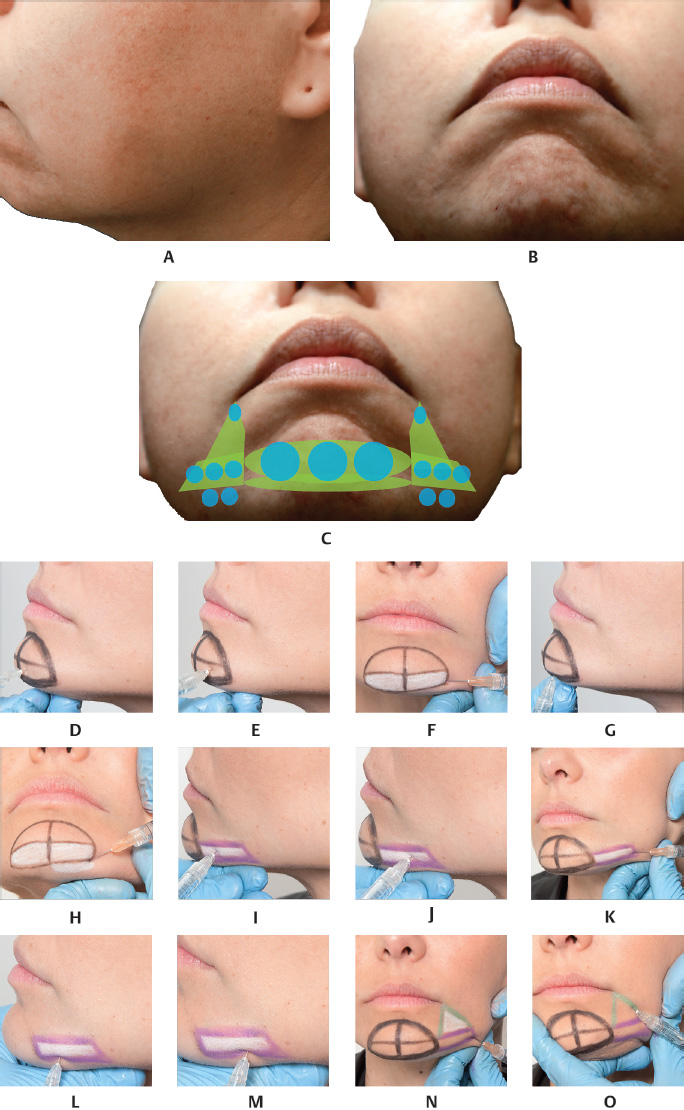
When the patient has a type II facial pattern at the orthodontic evaluation, i.e., a retrognathic chin, orthodontic treatments can be used and orthosurgical correction may be necessary. Filler injections may be indicated to help lessen this structural defect, together with a joint assessment by a dental surgeon. Another indication applies to patients without retrognathia but a disproportionately small chin.
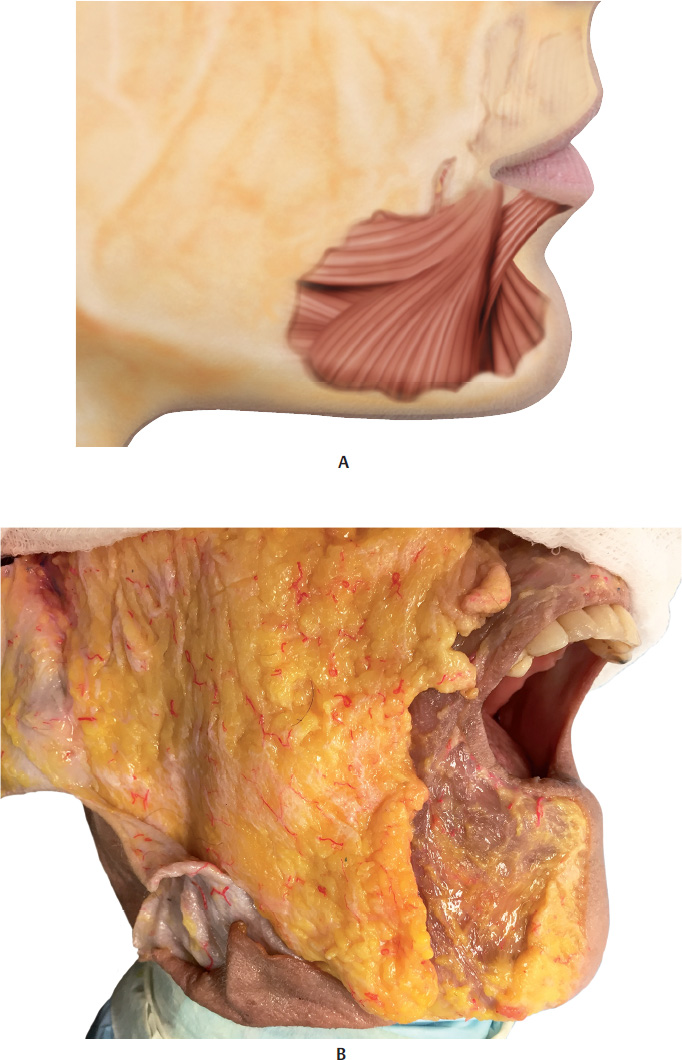
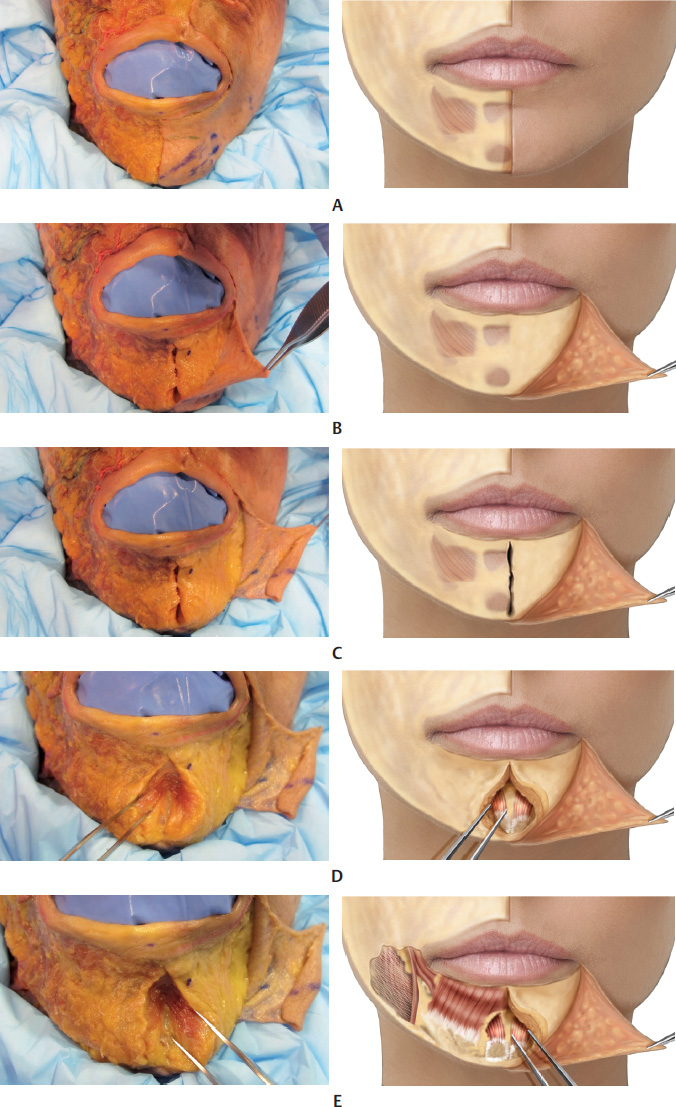
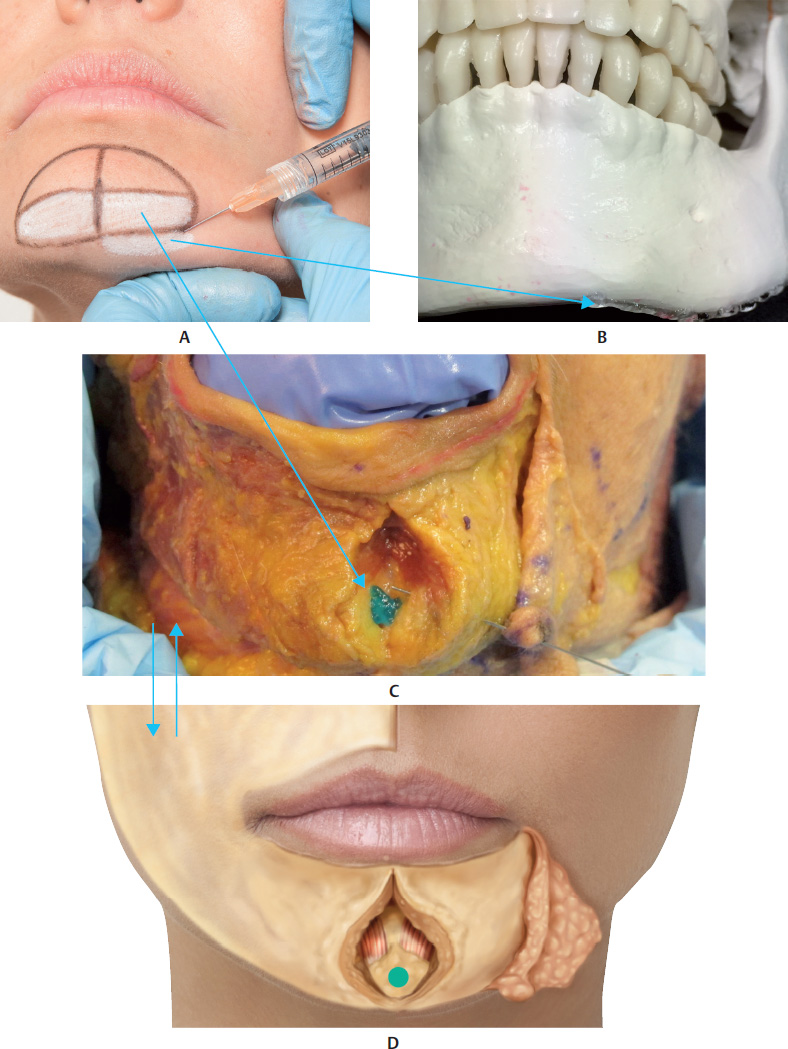
The mental region is composed of three tissue layers: the skin, the muscular-adipose layer, and the central periosteum of the mandible. The muscle layer comprises three muscles: the DMAM, the depressor muscle of the lower lip, and the mentalis muscle, which fuse inferiorly with the platysma. The mentolabial sulcus can be seen in the midline, formed by a fibroelastic lamina that extends from the mandibular symphysis to the skin. Deep in the mentalis muscle, there are two fat pads separated by this sulcus, which do not cross the midline.
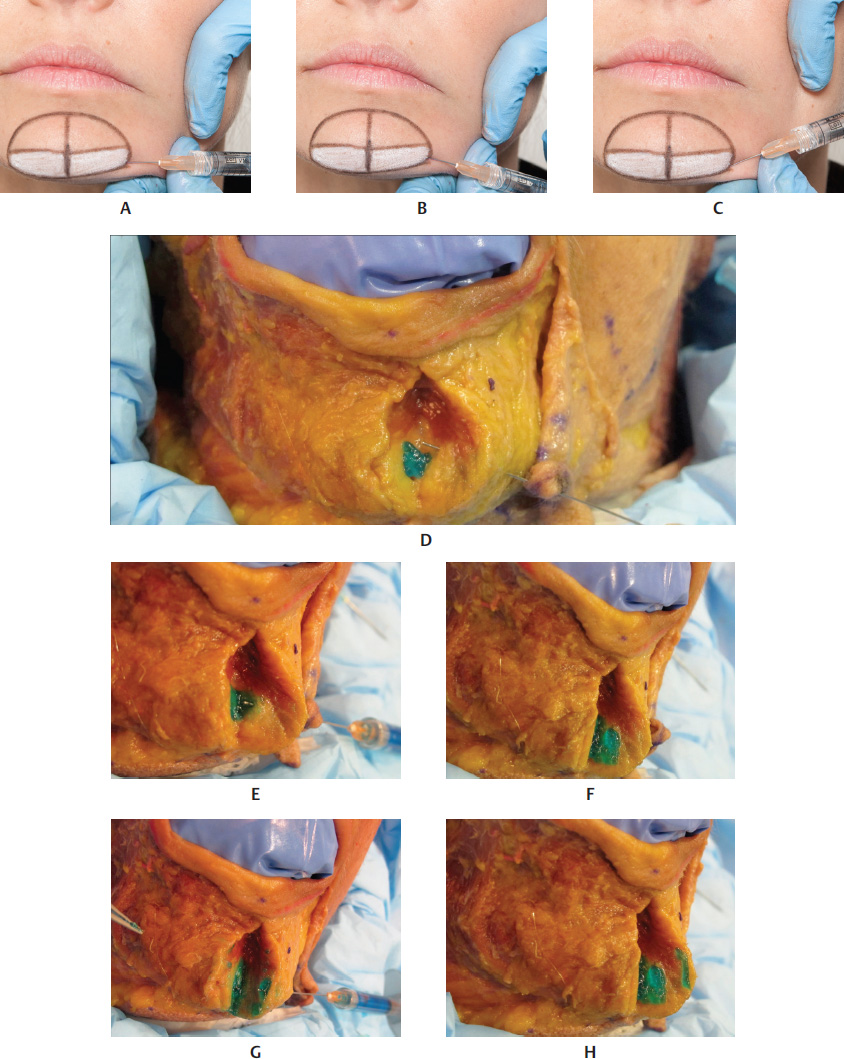
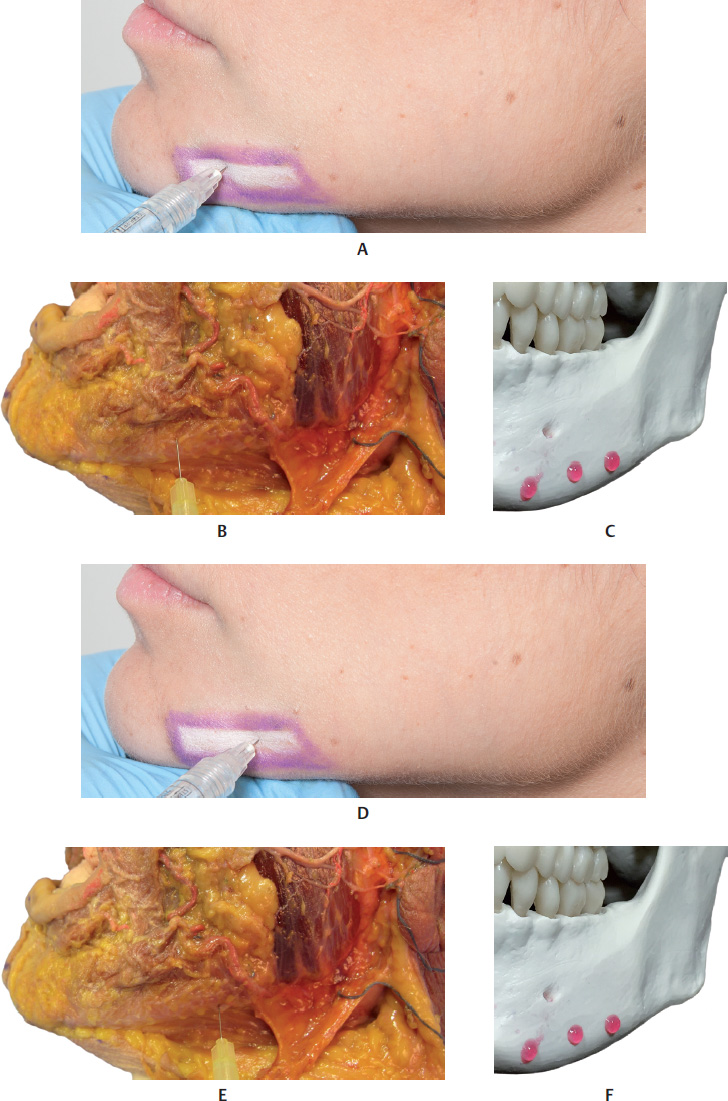
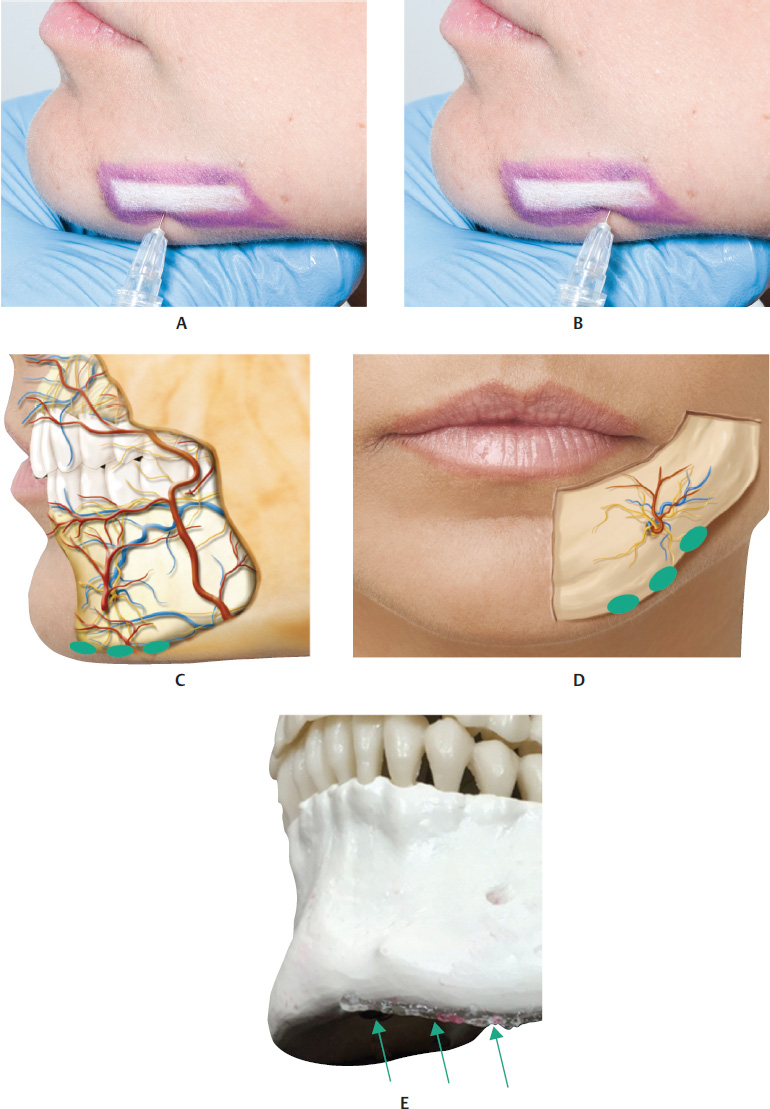
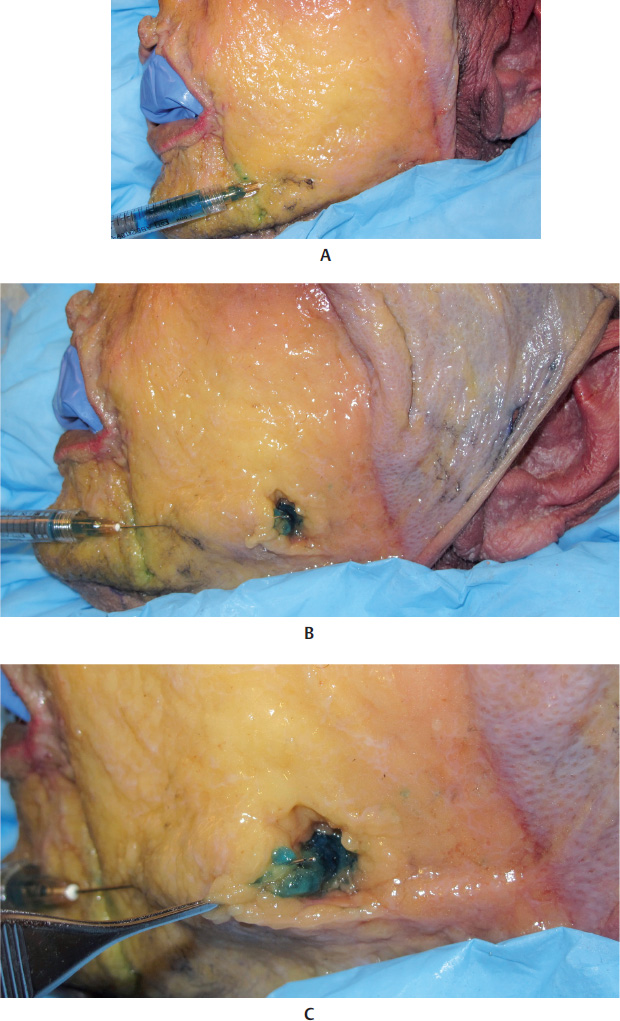
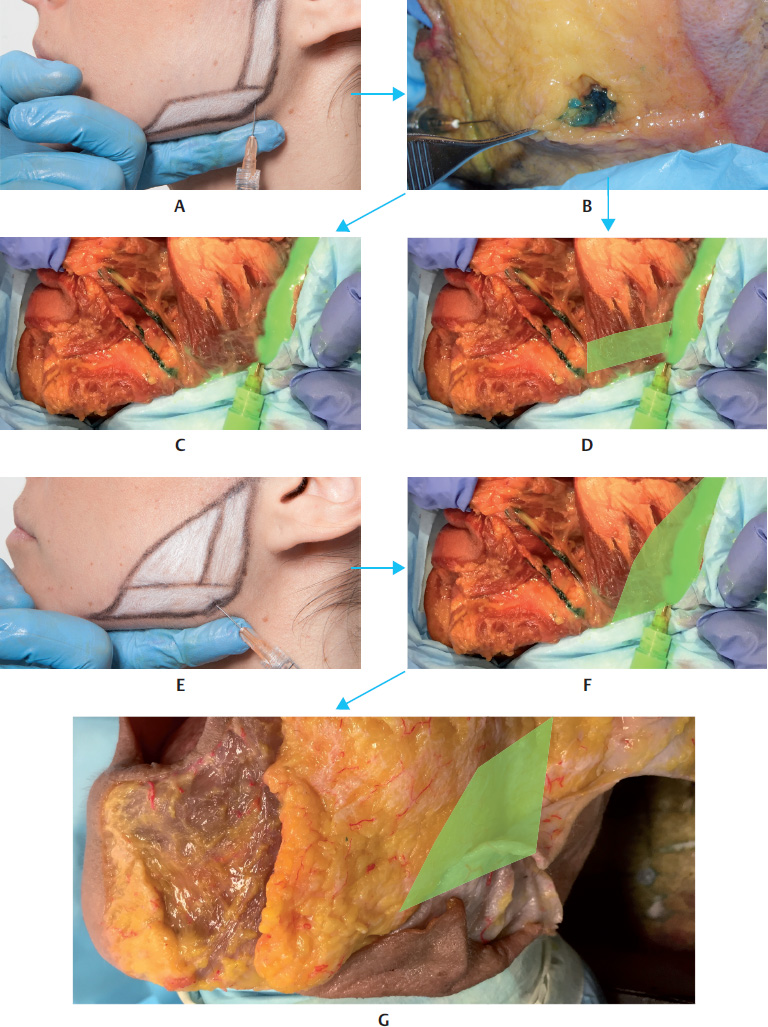
An entry point can be created in up to three different sites for inserting a microcannula or a needle. One option for the orifice is a site located inferiorly to the mental area, inserting the microcannula or needle into the supraperiosteal plane and injecting the product. Another possibility is to insert the needle into the same points marked for the application of botulinum toxin, surpassing the muscle and applying the product to the supraperiosteal plane. For this possibility, we recommend using needles only. Aspire and inject slowly.
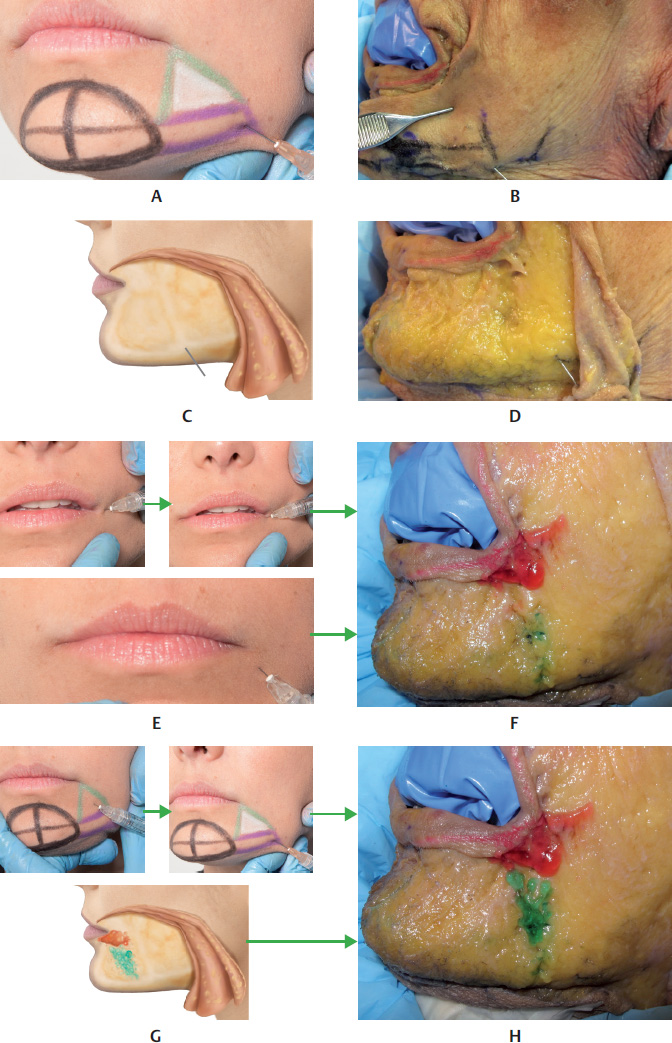
Start by marking the mental area, drawing a line around the chin in the shape of a semicircle up to the mandibular bone bilaterally. Then, draw a vertical line in the middle of the previously marked area, between the two bellies of the mentalis muscle. Palpate the bone base of the area marked and draw a horizontal line up to the semicircle. Then, draw a parallel line 1.5 cm above the previous one. This rectangular figure is the region suggested for the HA filler injection. After asking the patient to contract the chin, we suggest marking two points, one on each belly of the mentalis muscle, for applying 2 to 3 units of botulinum toxin to each point at the same time as the filler injection.
After creating an orifice with the needle, insert the microcannula, reaching the supraperiosteal plane, sliding it to the center of the rectangle on the side that is being treated. At this point, holding the microcannula still, inject between 0.1 and 0.3 ml of the product. In some cases, in order to harmonize the area treated, move the microcannula and inject another 0.1 ml of the product via retrograde injection into the subcutaneous plane above the muscle, in the corresponding rectangular area. Remove the microcannula and mold the region treated using firm and precise movements (Fig. 17.21,17.22,17.25–17.30, and17.41).
References
1 Carruthers A, Carruthers J, Monheit GD, Davis PG, Tardie G. Multicenter, randomized, parallel-group study of the safety and effectiveness of onabotulinumtoxinA and hyaluronic acid dermal fillers (24-mg/ml smooth, cohesive gel) alone and in combination for lower facial rejuvenation. Dermatol Surg 2010;36(Suppl 4):2121–2134 2 Jefferson Y. Skeletal types: key to unraveling the mystery of facial beauty and its biologic significance. J Gen Orthod 1996;7(2):7–25 3 Reis SAB, Abrão J, Filho LC, Claro CAA. Análise facial subjetiva. Rev Dent Press Ortodon Ortop Facial 2006;11(5):159–172 4 Carruthers JD, Glogau RG, Blitzer A; Facial Aesthetics Consensus Group Faculty. Advances in facial rejuvenation: botulinum toxin type a, hyaluronic acid dermal fillers, and combination therapies—consensus recommendations. Plast Reconstr Surg 2008; 121(5, Suppl):5S–30S, quiz 31S–36S 5 Goss CM. Gray anatomia. 29a edição. Rio de Janeiro: Guanabara Koogan; 1988 6 Reece EM, Pessa JE, Rohrich RJ. The mandibular septum: anatomical observations of the jowls in aging-implications for facial rejuvenation. Plast Reconstr Surg 2008;121(4):1414–1420 7 Reece EM, Rohrich RJ. The aesthetic jaw line: management of the aging jowl. Aesthet Surg J 2008;28(6):668–674 8 Hazani R, Chowdhry S, Mowlavi A, Wilhelmi BJ. Bony anatomic landmarks to avoid injury to the marginal mandibular nerve. Aesthet Surg J 2011;31(3):286–289 9 Braz AV, Mukamal LV, Costa DLM. Manejo cosmético del tercio médio e inferior de la cara. In: Atamoros FP, Merino JE, eds. Dermatologia Cosmética. Cidade do México: Elsevier Masson Doyma; 2011 10 Belmontesi M, Grover R, Verpaele A. Transdermal injection of Restylane SubQ for aesthetic contouring of the cheeks, chin, and mandible. Aesthet Surg J 2006;26(1S):S28–S34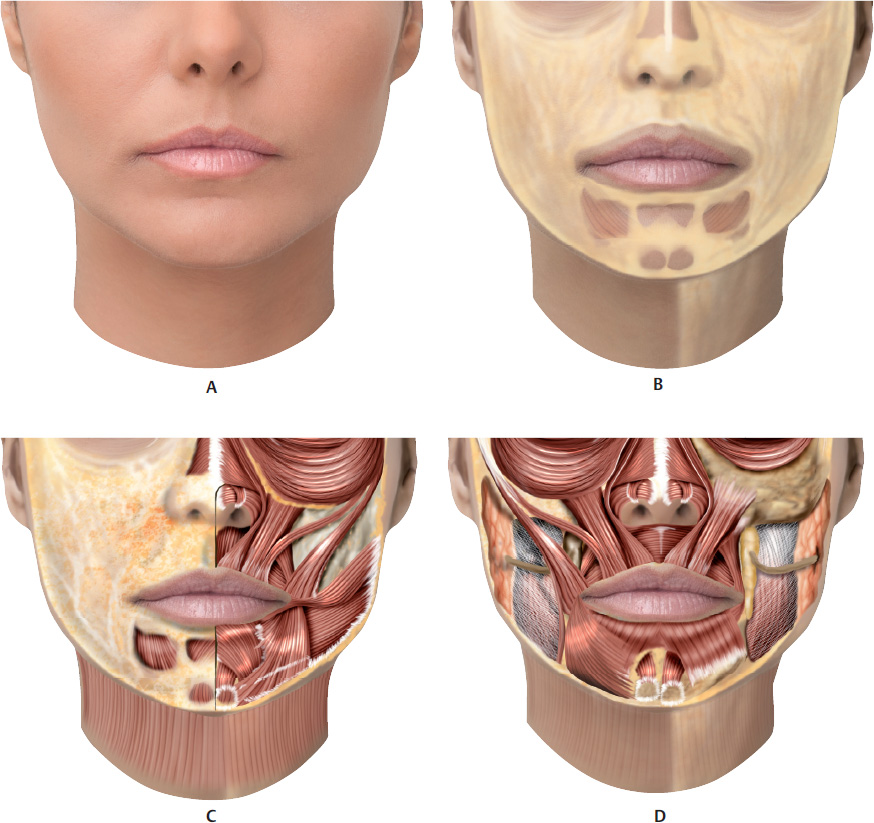
















Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


