Chapter 14 Filler Injection of the Nose
Introduction
Nonsurgical rhinoplasty using filler injections is an effective way of augmenting or recontouring the nose, and is well indicated for treating small humps on the dorsum of the nose and short, flat, or saddle noses. As it is a minimally invasive procedure, it can be performed in the cosmetic clinical offce, with immediate results and without the need for a postoperative recovery period. Despite the temporary effect, this procedure is becoming increasingly popular because it is simple, effective, and less expensive in the short term. In-depth knowledge of the local anatomy is essential for performing this procedure. Slimming a bulbous nose, reducing a large hump, and narrowing the base of the nose all require surgery, with reductive rhinoplasty. 1 -. 3
Anatomy
Structure
The nose has a pyramidal structure made of bone and cartilage; its apex corresponds to the root and its base to the nostrils. It comprises the skin, subcutaneous tissue, muscles (interconnected by the nasal superficial muscular aponeurotic system [SMAS]), and periosteum/perichondrium.
Its foundation comprises the nasal bone, upper lateral cartilages, lower lateral cartilages (greater alar cartilage), and lesser alar cartilages. The different cartilages are linked to one another and to the bones by a resistant fibrous membrane. The lower lateral cartilages have a horseshoe shape and go around each nostril; they then divide into the medial and lateral pillars (Fig. 14.1).
The nasal septum is a vertical osteocartilaginous structure that divides the nasal cavity into two. Its posterior part is bony and formed by the perpendicular plate of the ethmoid bone and the vomer, whereas its anterior part is formed by the quadrangular cartilage or cartilage of the septum. The skin and subcutaneous tissue that cover the septum between the nostrils are called the columella.
Externally, the nose has a fixed cephalic portion and a mobile caudal portion. The bony pyramid and the cephalic portion of the upper lateral cartilages are part of the fixed nasal structures, with the thin integument loosely adhering to the underlying structures. The mobile caudal cartilaginous structures are called lobe or soft nose and contain a thicker integument that adheres more firmly (Fig. 14.4,14.5,14.7, and14.9). 4 ,. 5
Vascularization
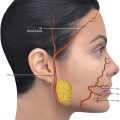
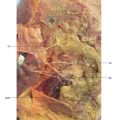
The external part of the nose is vascularized by the branches of the ophthalmic artery (branch of the internal carotid artery) and facial artery (FA) (branch of the external carotid artery). The superior portion of the nasal dorsum is supplied by the artery of the nasal dorsum (branch of the ophthalmic artery), and the inferior portion by the lateral nasal artery (LNA) (branch of the FA). The columella is supplied by the branches of the superior labial artery (SLA) (branch of the FA). The tip is irrigated by the branches of the LNA, dorsal nasal artery (DNA), and superior labial arteries (Fig. 14.6 and14.8–14.13). 5
Innervation
The skin of the nose are innervated by the branches of the infratrochlear and nasociliary nerves (branches of the ophthalmic and infraorbital nerves, respectively), and the muscles by the branches of the facial nerve (Fig. 14.6 and14.8).
Topography
The topographical reference points of the face are shown inFig. 14.2.
Thenasion (n), located in the nasal midline, is the depression of the root of the nose corresponding to the nasofrontal suture. Thesellion (s) orradix is the deepest point of the nasofrontal angle, and always located lower than thenasion. It defines the nasal root and represents the site of origin of the glabella on the nose, which is the least protruding and narrowest part of the nose. Thepronasion (prn) is the most protruding part of the tip of the nose, and thesubnasale (sn) corresponds to the junction between the columella and thephiltrum. Therhinion is the osteocartilaginous junction.
During the procedure, the injector will determine the appropriate position for each point, according to his or her sense of esthetics and considering the gender and ethnic origin of the patient, as well as the global appearance of the face. Generally, the longer a patient’s face, the more cranial the position of theradix. This marks the origin of the nasal dorsum, directly influencing the length (the more cranial, the greater the length of the nose).
The tip of the nose is delimited by a horizontal line that connects the tips of the nostrils and separates the tip of the columella; this extends from the tip of the nose to the anterior nasal spine and supports the tip of the nose.
The vertical alar plane is used as a reference for measuring the height (projection) of the nasal dorsum at the level of therhinion and the tip of the nose. The ideal height for the dorsum at the level of therhinion is between 18 and 22 mm, while the height of the tip of the nose is between 28 and 32 mm. At the level of thenasion, the height of theradix is 9 to 14 mm, measured from the anterior plane of the cornea. The length of the nose is the distance between thenasion and the tip of the nose (ideally between 45 and 49 mm). 6 ,. 7
Angles
Two angles are important when assessing the face in profile: the nasofrontal and the nasolabial. The nasofrontal angle (alpha) is formed by a tangential line to the glabella and another tangent to thepronasion, both originating from thenasion. The ideal angle is 115 to 130 degrees. The nasolabial angle (beta) is formed between the columella and the upper lip. Ideally, it measures 105 to 115 degrees in women and 90 to 105 degrees in men. Although not a substitute for esthetics, the abovementioned measures and angles serve as a guide for planning the procedure (Fig. 14.3). 6
Ethnic Variations
It is important to take ethnic variations into consideration when performing nasal filler injections. Rogers describes three basic types of ethnic noses according to historic categories and geographic location: Caucasoid (leptorrhine: long and thin), Negroid (platyrrhine: wide and flat), and Mongoloid (intermediate). When compared with the Caucasoid nose, the Negroid nose is shorter, and has a wide and depressed dorsum, broad and bulbous tip, and thick and wide alas. The columella is short and wide, the nostrils are horizontally ovoid, the nasofrontal angle is obtuse, and the nasolabial angle is acute.
The East Asian nose differs from the African in that the nasal root is flatter and narrower, the dorsum is narrower and less inclined, the tip is not bulbous, there is less protrusion of the tip, and the alas are thinner and less flared. The lower dorsum tends to make the tip appear flat and indistinct, and the eyes seem distant. Generally, with reference to corrections to the East Asian nose, the entire dorsum needs lifting, and the degree of this increase can be estimated by tracing an imaginary horizontal line over the supratarsal fold, relocating theradix there. An imaginary line between the newradix and the tip of the nose marks the site to be filled. With reference to correction of the nose of East Asian women, the contour needs to be more delicate; and the height needs to be reduced gradually up to thenasion, which should be the narrowest portion when seen from the front and the flattest when seen from the side. 8
Aging
Shaw et al 9 demonstrated. that like the orbit, the piriform aperture also increases in size with aging. Resorption is not uniform; the greatest loss occurs in the inferior portion, which is a critical area for supporting the lateral crus of the nose. This manifests clinically as a posterior shift of the ala of the nose and deepening of the nasolabial fold. The anterior nasal spine also gives way (more slowly), providing less support to the columella, with downward rotation of the tip of the nose and apparent lengthening of the nose.
Technique
Nasofrontal Angle and Nasal Dorsum
This technique is indicated for correcting small humps on the nasal dorsum, and flat, short, or saddle noses.
The artery of the nasal dorsum is a branch of the ophthalmic artery; therefore, there is a risk of intravascular injection and embolization in the retinal artery. Larger cannulas or an injection with a perpendicular needle should be used in the supraperiosteal plane.
When marking the new location of theradix, the supratarsal fold can be taken as a reference in order to establish a nasofrontal angle of approximately 135 degrees.
The entry point for the cannula for a filler injection can be in the midline of the face. For the deep dermis, you can use a filler agent or volumizer. For the subcutaneous application plane, use a 22 to 25 G cannula; for the supraperiosteal plane, use a needle, performing a perpendicular injection of small boluses. Inject slowly, always after aspiration (Fig. 14.15,14.16,14.23, and14.24).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


