CHAPTER 13 Pathophysiology of Secondary Lymphedema
KEY POINTS
The transport capacity of the lymphatic drainage system may be reduced as a result of surgery and/or radiotherapy for malignant tumors or after severe accidents, subsequently leading to lymphedema.
The pathophysiology and pathomorphology of secondary lymphedema include the degree of damage, stage of the disease, and presence of comorbidities.
Recognition of the stage of lymphedema is crucial to early treatment, whether surgical or conservative, to normalize the disturbed homeostasis.
Secondary lymphedema occurs after damage to the lymphatic drainage system and is most commonly associated with oncologic treatment (for example, after diagnostic or therapeutic lymphadenectomies or radiotherapy). Secondary lymphedema may also be a sign of malignant disease. Extensive soft tissue trauma and chronic inflammatory processes are the next most common causes of secondary lymphedema. The most commonly affected areas are the limbs; the least common are the head, trunk, and/or genitals.
The lymphatic drainage system comprises the lymph capillaries (initial lymph vessels), precollectors, prenodal and postnodal collectors, and lymph trunks. 1 The main tasks of the lymphatic drainage systems are as follows 2 , 3 :
Regulation of interstitial fluid volume
Maintenance of the normal metabolism of cells and extracellular matrix (ECM)
Removal of waste products
Ensure the circulation of lymphocytes
Migration of tissue macrophages, dendritic cells, and so forth
Elimination of cellular debris, including chemical components, such as inflammatory mediators, from injured tissue
When the physiologic function of the lymphatic drainage system is damaged, the homeostasis of the interstitium becomes disturbed both in the cellular and extracellular compartments. The disturbances of the complex relationships between the cellular compartment (fibroblasts, lymphocytes, macrophages, mast cells, and vascular and neurogenic structures) and ECM (collagen, glycoprotein, protein-glycan, glycosaminoglycans such as hyaluronan, chondroitin sulfate B, heparan, keratan sulfate, and other humoral substances and enzymes) lead to the remodeling of skin and subcutaneous tissues. Another important aspect is the influence on the immune system as a consequence of the impaired circulation of the lymphocytes. 4
Pathophysiology and Pathomorphology
The pathophysiology and pathomorphology of the secondary damaged lymphatic drainage system depend on several factors:
Degree of damage
Stage of the disease
Presence of comorbidities
DEGREE OF DAMAGE
Acute Lymphedema
Acute lymphedema is a rare condition that occurs most often after radical surgery (predominantly for pelvic malignancy) or severe accidents with soft tissue damage. The degree of damage to the lymphatic system can be so extensive that only a decreased number of functional lymph vessels remain. Their ability to regenerate is exceeded, and transport capacity in the lymphatic drainage system is dramatically reduced, with the consequence that lymphedema occurs and remains manifest.
STAGE OF THE DISEASE
Clinical Staging of Secondary Lymphedema
In clinical practice, the stages of lymphedema are defined by a physical examination of the extremities and staged according to the parameters outlined in Box 13-1.
BOX 13-1 Staging of Lymphedema
Latency: There is reduced transport capacity, with no clinical signs of swelling.
Stage 1: Pitting edema subsides with limb elevation.
Stage 2: Elevation of the limb is barely effective; in addition to pitting edema, there is hardening of the tissue resulting from fibrosis.
Stage 3: Lymphostatic elephantiasis, or large volume of the limbs, appears in either column or lobular form. Attendant symptoms are congestive dermatitis, trophic skin changes, and fat deposition.
Pathophysiologic Staging of Lymphedema
Latency
If the damage is less severe, sufficient numbers of functional lymph vessels remain and cope with the lymphatic load despite the reduced transport capacity. This condition refers to a latent or subclinical stage of lymphedema, in which swelling is not present despite the impaired lymph transport capacity. This stage of latency is characterized by increased lymph transport in the remaining functional lymph vessels, resulting from the activation of intrinsic factors. Stretching of the lymph vessel walls leads to increased lymphangion pulsation. 5 Over time, these compensatory mechanisms become insufficient. Tissue fluid begins to accumulate, with pathologic changes to the lymph vessels themselves and the connective tissue. The transport capacity of the lymphatic drainage system is further compromised and lymphedema occurs. The latency stage can last for several months to years.
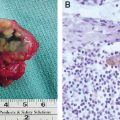
Stage 1 In stage 1, the examination of tissue samples under a light microscope reveals indirect signs of raised fluid content. Tissue samples are transparent and can only be lightly stained with hematoxylin-eosin and Giemsa. The electron microscope image of stage 1 lymphedema is characterized by dislocation and compartmentalization of collagen fibers. Immunohistologic changes in stage 1 are rarely mentioned in the literature, but it must be assumed that the ECM reacts in a multitude of ways to the increased tissue fluid load. It can also be assumed that glycosaminoglycans (hyaluronic acids) play an important role in the deposition of lymph fluid. 1 , 6
Stages 2 and 3 Pathomorphologic and pathophysiologic alterations in stages 2 and 3 of lymphedema are shown in Table 13-1. Examination of tissues under a light microscope reveals a high density of tissue through raised fiber content and increased cellular density, which surrounds the nerves, blood and lymph vessels, smooth muscle fibers, and fascia. Elastic fibers in particular remain in fragmented or granular forms. Furthermore, the inflammatory tissue changes lead to an increased deposition of adipose tissue. In chronic lymphedema of the skin, the dermis becomes thicker, extending cones of tissue in a wartlike manner not only toward the surface of the skin, but also into the subcutaneous adipose tissue structures. Collagen and lipid deposition lead, among others, to alterations in the hydraulic conductivity of the tissue. 7 – 9
It is unknown which factors in secondary lymphedema determine whether collagen fibrils will increase and thus predominantly lead to epifascial tissue fibrosis, including the deep fascia, with hardening of the skin and subcutis, or whether the deposition of fatty tissue will dominate, leading to a more voluminous lymphedema remaining soft on palpation. Based on my own animal experiments on chronic lymphedema in rabbits and laboratory rats, I found that 28 to 30 days after surgery, midgrade epifascial fibrosis with consecutive hardening of the skin and subcutis occurred in 50% of the animals, extreme fibrotic processes with severe hardening of the fascia occurred in 17%, and fatty deposition in the tissue was present in 33% of the animals. I had similar findings in human patients with secondary lymphedema based on clinical and ultrasound examinations, particularly with computed tomography. 10 I suspect that gender plays a role (and subsequent hormonal influences). The nutritional status of the patient also influences the pathophysiology of lymphedema.
Related posts:
 CHAPTER 15 Filaria
CHAPTER 15 Filaria
 CHAPTER 17 Combined Lymphatic and Venous Failure: Phlebolymphedema
CHAPTER 17 Combined Lymphatic and Venous Failure: Phlebolymphedema
 CHAPTER 16 Lymphedema in Pediatric Patients
CHAPTER 16 Lymphedema in Pediatric Patients
 CHAPTER 12 Pathophysiology of Primary Lymphedema
CHAPTER 12 Pathophysiology of Primary Lymphedema
 CHAPTER 19 Sentinel Lymph Node Biopsy Outcomes
CHAPTER 19 Sentinel Lymph Node Biopsy Outcomes
 CHAPTER 14 Dermatologic Implications of Secondary Lymphedema of the Lower Leg
CHAPTER 14 Dermatologic Implications of Secondary Lymphedema of the Lower Leg
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


