CHAPTER 17 Combined Lymphatic and Venous Failure: Phlebolymphedema
KEY POINTS
Lymphedema resulting from venous failure is frequently misdiagnosed.
A high frequency of lymphatic dysfunction is found in chronic venous disease.
If diagnosed, the edema may be reduced with venous outflow stenting and adjunctive measures, such as compression and risk factor modification.
Intravascular ultrasound is an effective way to image venous outflow obstruction not visualized on contrast venography.
Lymphedema caused by chronic venous disease is often characterized as secondary lymphedema and is often difficult to differentiate from primary lymphedema. In reality, the condition is best referred to as phlebolymphedema, 1 because it represents a combined central (or local) venous insufficiency combined with lymphatic insufficiency.
Other causes of secondary lymphedema include filariasis (which is the most common cause in tropical countries), surgical intervention associated with cancer treatment, radiation, or recurrent infection. 2 If secondary causes are eliminated with a comprehensive evaluation of the patient with a swollen limb, the assumption is that the lymphedema is primary. However, what is often overlooked is the high frequency (20% to 30%) of lymphatic dysfunction found in patients with chronic venous disease. The major causes of lymphatic damage develop from an elevated capillary and venous pressure (resulting from either right-sided heart failure, immobility, or venous obstruction) and chronic fluid overload on the tissues. 3 – 5
Lymphedema resulting from venous failure may improve with interventions designed to decrease venous hypertension, but only if the correct diagnosis is made. Therefore a deep understanding of the cause of limb swelling is needed to ensure that patients with lymphedema are diagnosed with primary lymphedema only after a thorough evaluation. In this respect, it is essential that lymphologists and phlebologists work together in a team treatment capacity. 6 , 7
Mechanism
Primary or secondary lymphedema generally occurs as a result of the accumulation of interstitial (but not always) protein-rich fluid, whereas the edema noted in pure venous disease is generally low-protein. When venous insufficiency occurs, however, venous hypertension may overload the capacity of the lymphatics to drain from the limb, resulting in chronic lymphatic insufficiency. Thus a mixed lymphedema and venous edema results.
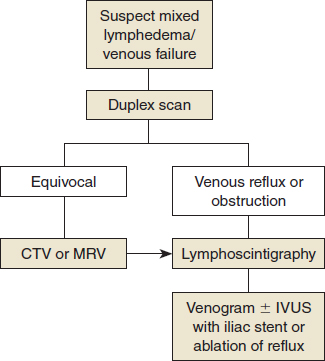
Diagnosis
Limb swelling and/or cellulitis is the most common presentation of this combined failure, although lipodermatosclerosis, fibrosis and papillomatosis, and ulceration along the malleolus may also occur. However, in most patients in whom phlebolymphedema is unrecognized, the hallmark signs of venous hypertension, such as ankle hyperpigmentation and corona phlebectatica, although frequently seen, may not be obvious and sometimes lead to the misdiagnosis of primary lymphedema. In addition, clinical signs that are characteristic of lymphedema may be seen, such as pitting edema, squaring of the toes with swelling, and edema over the dorsum of the foot. In many patients, however, clinical findings are too nonspecific to make a definitive diagnosis without further imaging studies, 8 although even the latter (MRI or CT) are often unable to provide a clear differentiation of the various forms of chronic edema. 9
Noninvasive Studies
VENOUS PLETHYSMOGRAPHY
Venous plethysmography with air, strain-gauge, or photoplethysmography may be one of the early studies performed when evaluating the swollen limb. Typically findings are correlated with ultrasound for improved diagnostic sensitivity. Although studies have shown value in assessing venous functional changes and quantifying the results of surgical intervention, 10 , 11 there is no clear role for venous plethysmography, in addition to duplex ultrasound. 12
IMAGING
Duplex Imaging
Although duplex imaging is often the primary imaging modality for both screening and the diagnosis of venous compression, it may not be sensitive enough to identify common iliac vein lesions. When performed in the upright and supine positions, duplex imaging may identify venous insufficiency or venous obstruction or reflux and quantify the degree of reflux. The criteria for valvular incompetence include a valve closure time greater than 1 second for femoral and popliteal veins and 0.5 second for the great saphenous, small saphenous, tibial, deep femoral, and perforating veins. 12 When ultrasound is used to identify outflow obstruction, however, the degree of iliac vein stenosis may be underestimated, and adjunctive imaging, such as CT, MR venography, or intravascular ultrasound (IVUS), may be necessary. 8 , 13
Nucleotide Lymphangiography
In both primary and secondary lymphedema, lymph node uptake may be delayed or absent, as demonstrated on nucleotide lymphangiography, even after prolonged observation periods. 14 , 15 Lymphoscintigraphy may be more useful to assess improvement postoperatively, as will be discussed. When performed, an injection of technetium-99m sulfur colloid is given between the subcutaneous space of the first and second toes, and images are taken at scheduled intervals to assess movement of the colloid. The progress may be monitored for 2 hours or more, depending on the progress of the lymph drainage and the region of interest. The images are assessed for pooling of the tracer or reflux into the limb and the rate of movement up the limb (Fig. 17-1). Thus qualitative and quantitative information can be gained from the same imaging strategy. Typically, normal lymph drainage will allow movement of the colloid and visualization of the lymph nodes by 20 minutes. 8 However, drainage is often affected by patient movement, facilitating lymph drainage (or not) during the observation period. Values still vary because of the lack of a standard protocol. 9
Raju et al 8 also recommend the use of triple-dose lymphangiography in which 1.8 mCi (compared with 0.6 mCi in standard lymphoscintigraphy) is injected to overcome the risk that a large fluid collection could dilute the isotope and interfere with lymphatic imaging. In their series, Raju et al 8 report 71 limbs in all clinical, etiology, anatomy, pathophysiology (CEAP) classifications of chronic venous disease that had delayed or absent node visualization on standard lymphoscintigraphy. All 71 limbs underwent triple-dose lymphangiography. Of these 71 limbs, 10 were normal and 16 were abnormal in CEAP C3. 8
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


