CHAPTER 18 Cementless Acetabular Fixation
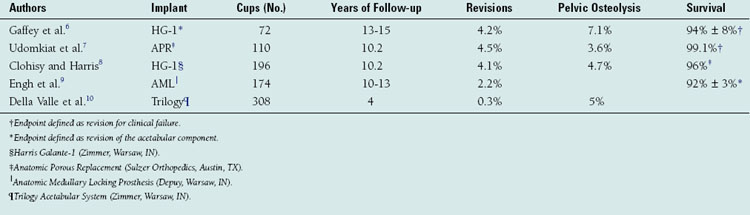
The first total hip arthroplasty was performed in 1938 in London more than 20 years before polymethylmethacrylate would be introduced as a bone cement.1 With the introduction of his cemented hip prosthesis in the 1960s, Charnley forever changed the future of total hip arthroplasty.2,3 Although the early results with cemented cups were excellent, it became clear with long-term follow-up studies that cemented acetabular components develop high rates of loosening and migration (Table 18-1).2–10 The pathologic process involved in the loosening of cemented acetabular components came to be known as cement disease.11 Many in the field believed that cement represented the major obstacle to long-term fixation, and attempts were made to eliminate the use of polymethylmethacrylate in the hope that this would limit aseptic loosening.12
It is clear that if an arthroplasty is to have durable long-term function it must develop a biologic and mechanical equilibrium with the host bone.1 In 1979, Morscher described several special requirements for an endoprosthesis to be fixed without cement.1 The first requirement is to create as small a defect as possible, such as to disrupt the physiologic biomechanics of the bone as little as possible. The design, stabilization, and mechanical properties of the prosthesis must take into consideration the forces acting on the system in all directions to avoid micromotion during physiologic loading of the implant. Lastly, the biologic nature of the bone should be respected, taking care to avoid excessive damage to the surrounding tissues during preparation and insertion.
DESIGN
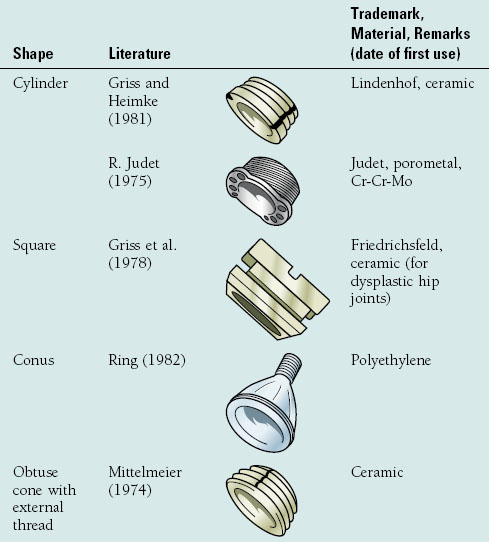
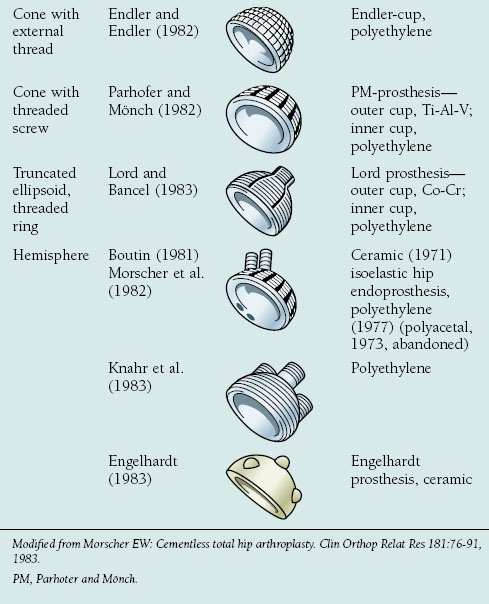
The transmission of forces in an artificial joint should be as physiologic as possible. The ideal implant therefore would be one that interferes least with the physiologic stress patterns of the native hip and pelvis.3,13 Morscher outlined the five major cup designs that have been used for cementless fixation in total hip arthroplasty since 1974 (Table 18-2).1 The five principal designs included cylindrical, square, conical, ellipsoid threaded ring, and hemispherical cups. Data regarding cementless acetabular fixation have shown the hemispherical cup with a porous ingrowth surface is the most successful design.7,14,15 A hemispherical cup provides a contact surface on which the forces that develop between the pelvis and femoral head can be transmitted in a physiologic balance between compression and shear. The hemispherical shape also eliminates undesired stress concentrations that occur with cement fixation or in cups that deviate from this design.1 Finally, this design most closely mimics the anatomy of the acetabulum and allows for the least bony resection.
INGROWTH
Bony ingrowth is paramount to the success of cementless acetabular fixation. One of the determinants of bone ingrowth is the degree of initial stability of the component.16,17 Cementless acetabular cups are manufactured with a variety of features critical to success, including geometry, surface structure, and type of adjuvant fixation, all designed to maximize stability and ingrowth.18
GEOMETRY
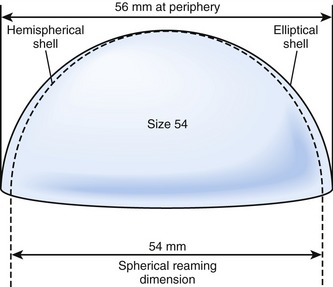
Three hemispherical cup designs have been developed in an effort to improve implant stability: true hemispherical, elliptical, and dual-geometry. Hemispherical and elliptical cups have an overall shape that is either hemispherical or slightly flared to an ellipse (Fig. 18-1). The elliptical cups have a peripheral flare to theoretically improve rim press fit.19 The dual-geometry cups are hemispherical, with the radius at the equator slightly larger than the radius at the dome.20
SURFACE AND COATINGS
The primary surface structures used in modern acetabular implants include sintered materials such as metallic beads, diffusion bonded materials such as titanium fibermetal mesh, and roughened surfaces created with grit blasting.17 These surfaces were developed to create pore sizes that optimize bone ingrowth. A pore size of 100 to 400 µm provides the greatest opportunity for ingrowth.17 Retrieval studies have shown that in spite of these designs acetabular bony ingrowth is unpredictable.21 Engh and colleagues found acetabular ingrowth averaged 32% (of the cup surface) but ranged from 3% to 84% in well-functioning hips retrieved at autopsy. They also found in areas where ingrowth had occurred that 48% of the available pore space was occupied by mature bone, a consistent finding regardless of how much of the cup surface had bone ingrowth.22 This has prompted some investigators to search for methods to not only increase the amount of bone ingrowth but also to increase the rate of bone ingrowth and improve the bone-implant attachment strength.23 Various surface coatings have been studied for this purpose.
Calcium phosphate ceramics have been found to be biocompatible, nontoxic, and capable of direct intimate bonding with bone owing to the chemical similarity to the mineral component of bone.24 Hydroxyapatite is the most studied of the calcium phosphates.23–25 Canine studies comparing porous hydroxyapatite-coated implants to porous coated implants without hydroxyapatite found a significant increase in interference attachment strength and bone ingrowth with the hydroxyapatite-coated implants at virtually all time points from 8 weeks to 52 weeks, even with gaps up to 1.0 mm.24 The authors concluded the use of a hydroxyapatite coating on the implant had a positive effect on fixation, especially when the initial gap was small. Clinical studies have found hydroxyapatite coating to be beneficial for femoral component survival, but results with hydroxyapatite-coated acetabular components have not been as promising.26,27 Two multicenter studies have found acetabular aseptic failure rates of 11% to 14% at an average follow-up of 7.9 and 8.1 years, respectively, for smooth hydroxyapatite-coated cups.26,27 The aseptic failure rates for press-fit porous cups without hydroxyapatite in these studies were 2.0% and 2.7%.26,27





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


