CHAPTER 32 Preoperative Radiographic Evaluation and Classification of Defects
EVALUATION
Plain Radiographs
Aseptic Loosening
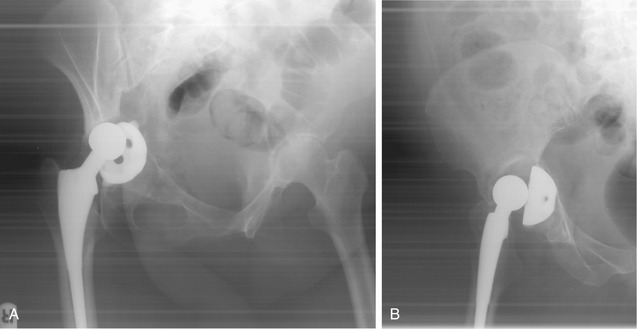
Serial plain films remain the most reliable method of detecting loosening of both cemented and uncemented THAs.1 In cemented THAs, loosening is defined using the criteria described by Harris and McGann (Fig. 32-1).2 In this classification, femoral component loosening is categorized as definite (component migration or cement fracture); probable (complete radiolucency at the cement-bone interface); or possible (radiolucency at 50% to 100% of the total cement-bone interface). Acetabular component loosening is defined as definite (component migration or cement fracture) or impending (continuous 2-mm bone-cement radiolucency). Of note, these radiographic appearances have been found to correlate more accurately with femoral than with acetabular loosening.1 Metal-cement radiolucency may represent initial poor cementation and if stable is not indicative of loosening. Debonding of the stem from the cement mantle may be demonstrated by the development of a radiolucent zone. Certain tapered cemented stems, such as the Exeter (Howmedica, Rutherford, New Jersey), may subside without cement mantle failure, leaving a radiolucency above the shoulder of the implant laterally (Fig. 32-2). The presence of these radiolucencies is described according to the methods of Gruen3 and DeLee and Charnley4 for the femoral and acetabular components, respectively (Fig. 32-3).


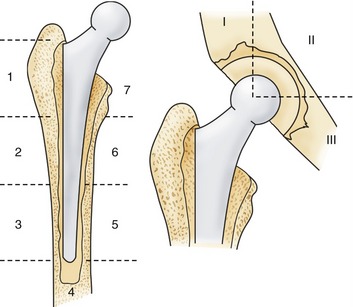
Uncemented implant stability can be assessed using criteria described by Engh and colleagues.5 Osseointegration of cementless stems is defined using major and minor criteria. Major criteria are presence of reactive lines and endosteal “spot-welds” around the porous-coated part of the stem. Minor criteria for osseointegration include calcar atrophy, the absence of bead-shedding, and the absence of a distal pedestal (Fig. 32-4). A pedestal appears as endosteal sclerosis that extends into the medullary canal at the tip of the femoral component (Fig. 32-5). Isolated pedestal formation does not indicate instability when not associated with radiolucent lines. Component migration is the only reliable sign of acetabular component instability.1


Serial radiographs should also be scrutinized for wear of the acetabular polyethylene liner, which, if marked, should prompt the observer to assess for associated osteolysis. Severe osteolysis may be asymptomatic but may be associated with the risk of pathologic fracture and component loosening. If 50% of the shell circumference has evidence of osteolysis on anteroposterior (AP) or lateral radiographs, surgical intervention may be indicated.2
Septic Loosening
Certain plain radiographic features are suggestive of septic loosening, particularly if rapidly progressive. These include endosteal scalloping, osteopenia, generalized osteolysis, and periosteal new bone formation (Fig. 32-6).

Aspiration and Arthrography
Isolated hip arthrography has little clinical use in the absence of joint aspiration as part of the workup to exclude septic loosening.1,7 Arthrography as a method of assessing component loosening probably overestimates acetabular loosening while having a higher false-negative rate on the femoral side. This technique is even less reliable when used to evaluate uncemented components.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


