CHAPTER 25 Total Hip Arthroplasty in Patients with Metabolic Diseases
KEY POINTS
 Account for the effects of the metabolic disease on the patient’s overall physiologic condition. Consider how this affects skeletal healing, ingrowth of bone, remodeling and mechanics, selection of implants, and risks of complications.
Account for the effects of the metabolic disease on the patient’s overall physiologic condition. Consider how this affects skeletal healing, ingrowth of bone, remodeling and mechanics, selection of implants, and risks of complications.

METABOLIC DISEASES
Sickle Cell Hemoglobinopathies
In sickle cell hemoglobinopathies there are three main orthopedic issues as a result of the disease process that the surgeon must consider: marrow hyperplasia, osteonecrosis, and pyogenic infections.1 The underlying cause of marrow hyperplasia in the patient with sickle cell disease is a result of repetitive end organ necrosis and infarcts. When the spleen is significantly infarcted, the marrow increases hematopoiesis, leading to marrow hypertrophy, in turn resulting in thinning of the cortex of long bones. As the process continues, the blood supply is compromised in small areas, resulting in ischemia and bone infarctions. These areas of bone infarcts become patchy areas of sclerotic bone and eventually lead to canal stenosis or even obliteration. In addition, because of these changes to the bone marrow, compromising its blood supply, as well as the presence of an autoinfarcted spleen, these patients are also at increased risk for pyogenic infections with Streptococcus pneumoniae, Salmonella, and Klebsiella (which can spread hematogenously and seed bone). Despite this, Staphylococcus aureus is still the most commonly reported pathogen in patients with sickle cell disease who undergo total hip arthroplasty and acquire an infection.2
Several studies have reported comparable results of total hip arthroplasty in patients with sickle cell disease using cemented and uncemented components.3,4 The more recent studies support the use of uncemented components with favorable outcomes.5 There are limited numbers of patients in these studies and, because there are no prospective randomized trials, definitive knowledge regarding which method is superior is unclear. We use uncemented components and thus will focus our discussion on the use of this technique.
Paget Disease
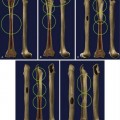
Paget disease is a metabolic bone disorder that primarily affects individuals of Anglo-Saxon ancestry. Although there is evidence to suggest its etiology is a slow viral illness affecting patients with a genetic predisposition, definitive proof of this has not been established.6 In Paget disease there is a marked increase in bone resorption and formation in one or more isolated anatomic areas (e.g., monostotic or polyostotic Paget disease). The most common locations occur around the hip and include the proximal femur as well as the acetabulum and pelvis. There are two main phases of the disease: lytic and blastic. During the active lytic phase there is an increase in the vascularity to the bone (Fig. 25-1), which is associated with increased bone pain. This is very important to the overall physiology of the patient because this demand for oxygen and shunting of blood to the bone may overload the circulatory system, resulting in high-output cardiac failure.7 Implant fixation can also be affected by this hypervascularity, such as in preventing good fixation with cemented components. By using serum alkaline phosphatase and urinary markers of bone collagen, turnover activity of the disease may be quantitated. This can help the surgeon or medical consultant to control disease activity before operative intervention.
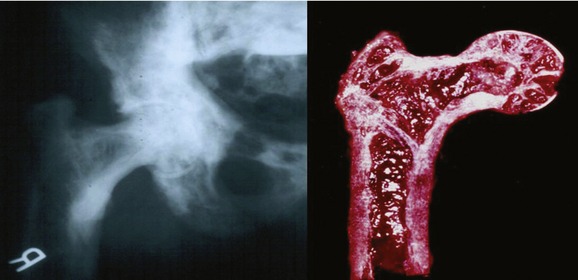
Pagetoid bone is also susceptible to bone deformities, such as coxa vara and femoral bowing, which should be clearly defined with proper preoperative radiographs, particularly if a long-stemmed prosthesis is to be used or if an osteotomy is planned (Fig. 25-2).

Osteoporosis
Very few studies have carefully evaluated the impact of osteoporosis on outcomes of total hip arthroplasty.8–10 However, whereas studies specific to osteoporosis are limited, several investigations have evaluated the outcomes of total hip arthroplasty in the elderly. In these reports, patients were not stratified by bone density but rather by proximal femoral morphology.9–11 Although it has been suggested that severe osteoporosis should influence prosthesis selection and whether to use cemented or uncemented components,8 no definitive investigations have addressed these concerns.
More recent studies suggest that uncemented stems are as efficacious as cemented stems and this is our implant of choice.11
Dorr and colleagues described the effects of osteoporosis on the proximal femur as a means of understanding the potential impact of aging and metabolic bone disease in preparation for total hip arthroplasty. They correlated radiographic findings with histologic changes as they classified the morphology of the proximal femur. The classification system consisted of three morphologic types with type A representing one found in younger male patients with thick cortices, type C representing the femur of an older patients with thinner cortices and a wider intramedullary canal often found in elderly women, and type B as a transitional stage between the two. These findings indicated that as canal widening occurs the endosteal cortex becomes more porous and progresses to the periphery.9 The concern with using cementless stems in this population is that the resorption will prevent adequate bony ingrowth and result in aseptic loosening and pain.
As individuals age and bone loss occurs there is a loss of the trabecular scaffolding that adds support to the cylindrically shaped cortex. As endosteal bone loss increases, periosteal bone apposition occurs as a compensatory mechanism to protect the diaphysis mechanically. As a consequence, the geometry of the femoral diaphysis is altered such that the femur widens and resembles a stove pipe with thin cortices: the type C femur of the Dorr classification.9 However, despite the protection afforded the femur when loaded in torsion or bending, the so-called hoop stresses induced by broaching and implantation of the prosthesis are not influenced by cortical expansion.12 Instead, the osteoporotic and aged femur is susceptible to fracture during the operation and thus care must be exercised at key times, such as when the hip is dislocated in preparation for femoral and acetabular preparation and when the femur is machined to accommodate the stem component.
Renal Disease
Because the kidney plays a major role in maintaining mineral hemostasis of bone, renal disease significantly alters the metabolic activity of bone. Arthroplasty surgeons need to be familiar with the osseous changes secondary to renal failure because these metabolic changes affect the quality of bone. Two types of osteodystrophy have be described similar to the phases of Paget disease, a high-turnover and a low-turnover osteodystrophy.13 Classic renal osteodystrophy is a high-turnover state in response to secondary hyperparathyroidism with high levels of parathyroid hormone being produced. These high levels of parathyroid hormone cause an increase in osteoblast and osteoclast activity. Low turnover renal osteodystrophy occurs because of the advances in treating renal disease. It occurs in patients whose disease is being treated adequately and who have normal levels of parathyroid hormone and adynamic bone.14 The defect here is believed to be due to the inability to excrete aluminum. Aluminum impairs osteoblastic proliferation and maturation, resulting in these adynamic or aplastic bone lesions.
Regardless of the cause, as a result of renal disease the arthroplasty surgeon will encounter skeletal deformity due to osteomalacia and heterotopic calcifications. These patients often present with pain and weakness and may have extraskeletal manifestations such as periarticular calcifications. There is a high incidence of total hip arthroplasty in patients on dialysis or with kidney transplants. Osteonecrosis is the leading diagnosis for a total hip arthroplasty in this patient population.15 As a result of the soft osteomalacic bone, cemented femoral stems have been recommended. Loosening has been a problem identified with total hip arthroplasty, and high revision rates (46%-58%) have been reported, with a mean follow-up of 8 years.16,17 Understanding renal disease and its musculoskeletal significance is very important for arthroplasty surgeons, and recognizing that a total hip arthroplasty in this patient group in not a routine total hip replacement is critical.