Case 63 Ethics
63.1 Introduction
Medical ethics lies at the heart of medicine. The mission statement of the American Board of Plastic Surgery (ABPS) reads, “The mission of the American Board of Plastic Surgery, Inc. is to promote safe, ethical, efficacious plastic surgery to the public by maintaining high standards for the education, examination, certification and continuous certification of plastic surgeons as specialists and subspecialists.”s. Literatur This chapter will aim to review important principles in medical ethics and apply them to clinical cases pertaining to plastic and reconstructive surgery.
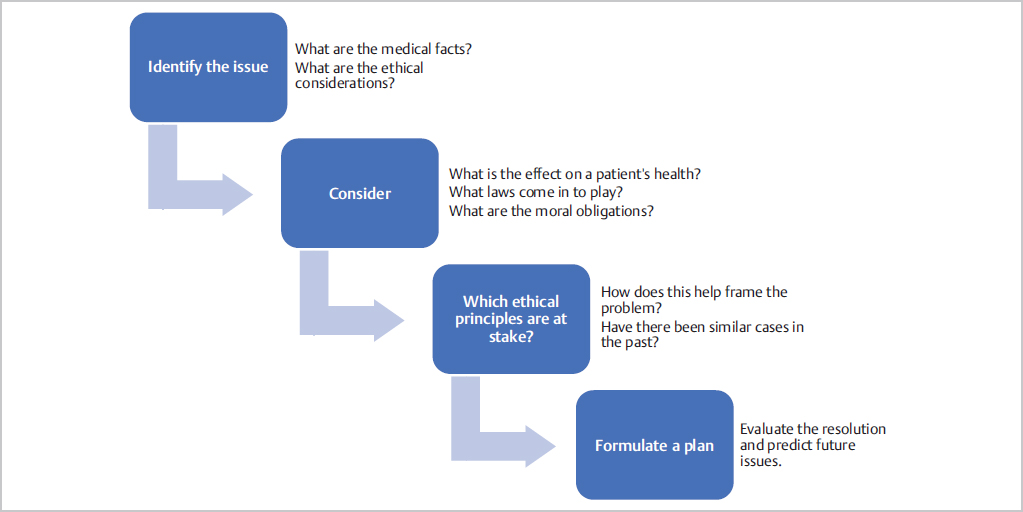
The American Board of Plastic Surgery strives to certify competent, ethical, and safe surgeons. Some may even argue that ethical standards are one of the most important testing principles of the Oral Board Examination. It is a guarantee that there will be ethical scenarios in the Oral Board Examination, so you will need to be prepared to work through these. Just like the clinical scenarios of the examination, we recommend working through the problems in a stepwise fashion (see Fig. 63-1)
Identify the issue
What are the medical facts?
What are the ethical considerations?
Considerations
What is the effect on the patient’s health?
What laws come into play?
What are the ethical obligations to the patient?
Which ethical principles are at stake?
How does this help frame the problem?
Have there been similar cases in the past?
Formulate a plan
Evaluate the resolution and predict potential future issues
In the Oral Board Examination, there most likely will be a future issue, so be prepared for your resolution to not work as planned
63.2 Application of Medical Ethics to Plastic and Reconstructive Surgery
Case 1: A patient sees a new surgeon for revision of a previous rhinoplasty that had some postoperative complications and a subjective poor result. The patient expresses the desire to sue his or her previous surgeon and would like you to revise the previous surgeon’s “mess ups.”
The AMA Code of Ethics (Opinion 9.031) cites an ethical obligation to report impaired, incompetent, or unethical colleagues.s. Literatur This obligation stems from the responsibility to protect patients from harm. Depending on the situation, the reporting is usually escalated in a stepwise fashion. “Impaired” is defined as conditions that interfere with the ability to engage safely in professional activities.s. Literatur With regard to incompetence, the Code recommends that incompetence that poses an immediate threat to the safety of patients should be reported directly to the state licensing board.
Likewise, the code of ethics of the American Society of Plastic Surgeons (ASPS) states that members “should expose, without hesitation, illegal or unethical conduct of fellow Members of the profession.”s. Literatur
In the case above, if the new surgeon does not believe that the patient experienced impaired, incompetent, or unethical treatment, then the best course of action is to focus on developing a therapeutic relationship with the patient and to avoid engaging in speculation regarding prior care.
Tell the patient that you will not focus on what happened in the past, but will view the problem with a fresh set of eyes and will focus on the resolution of the problem.
Even with blatant signs of malpractice, discussions about other physicians’ practices should be avoided until risk management and/or legal counsel is involved.
It is a good idea to consider multiple preoperative consultations with this patient to ensure that he or she is fully aware of what procedure will be performed and that the expectations are reasonable. The patient also needs to understand the possible risks and benefits of the proposed procedure.
The consulting plastic surgeon is not obligated to operate on this patient. If you decide that you do not want to perform the procedure, give the patient the names of other plastic surgeons who may be better suited to treat the issue.
A word on malpractice law: There are criminal law and civil law.s. Literatur To be found guilty in a criminal case is to be found guilty of crimes against society and is associated with prison and monetary damages. To be found guilty in a civil case is to be found liable to the individual plaintiff and is associated with monetary damages. Most medical malpractice cases are civil lawsuits.s. Literatur However, there is a possibility of “criminal negligence” if the opposition can prove that the physician acted so recklessly that there was “implied intent” of harm. Thankfully, allegations of criminal negligence against physicians are uncommon. The most expensive medical malpractice allegations includes. Literatur:
Improper performance
Errors in diagnosis
Failure to supervise or monitor—especially important to note for surgeons in teaching hospitals
Medication errors
Case 2: During preoperative consultation for a breast reconstruction, it appears to the surgeon that a patient has unreasonable expectations or an incomplete understanding of the risks and benefits of surgery.
The ethical consideration at stake in this case is the ability of the patient to participate in informed consent, which falls under the principle of Respect for Personhood.
If the patient is incorrectly or incompletely informed about the procedure, the surgeon has an ethical obligation to inform the patient adequately prior to obtaining consent.
If the patient is incapable of giving consent (i.e., lacking capacity), then attempts must be made to obtain proxy consent in order to respect the patient. Traditionally, the capacity for giving consent is considered include the following four elementss. Literatur:
The patient is able to communicate a choice.
The patient understands the relevant information.
The patient appreciates the medical condition and/or consequences of treatment.
The patient can manipulate information rationally.
A physician’s duty to respect personhood goes beyond the delivery of information.s. Literatur Physicians must attend to how the information is received and understood. A physician should aim to understand the rationality behind a patient’s beliefs and help a patient to deliberate more effectively.
This scenario is very common in a plastic surgeon’s practice. There are many strategies that you can employ in your discussions with the patient, but the end goal is that you and the patient are “on the same page” and the expectations are completely understood.
The patient should return multiple times for a preoperative consultation to have ongoing discussions about the proposed procedure and the potential complications and/or deformities that could occur.
The patient should be shown photos of the proposed procedure so that she is fully aware of the potential scars and cosmetic outcome.
Case 3: A surgical procedure is declined by insurance. The patient requests that the surgeon to adjust his or her assessment and document different findings in order to get insurance approval.
Accurate documentation is not only an important component of good patient care, but an ethical obligation on the part of the surgeon. Adjusting findings in order to obtain insurance coverage could be considered insurance fraud and is strongly discouraged.
The physician should politely decline to falsely adjust findings and instead focus on developing an alternative strategy with the patient.
One way to approach the conversation is to say that falsification of the medical records could result in the loss of your medical license. When patients hear this, they tend to understand your hesitation and comfort level with what they are asking you to do for them.
Focusing on alternative methods to approach the problem helps build trust with the patient that you are a sound and ethical surgeon.
Case 4: A patient’s insurance has approved a panniculectomy. The patient would like an abdominoplasty but cannot afford to pay for it out-of-pocket. The surgeon considers doing the abdominoplasty work for free. What are the ethical considerations regarding this decision?
There are several considerations here:
Physicians have a responsibility to help ensure that the needs of the poor are met (see Opinion 9.065 of the Code of Ethics).s. Literatur
An abdominoplasty is not medically necessary and thus conveys no substantial moral obligation on the physician.
The physician is able to provide services free of charge but is under no obligation to do so.
If the physician chooses to perform the abdominoplasty portion of the procedure for no charge, the patient has to understand that he or she will still be required to pay for the extra anesthesia required for prolonging the case.
Another consideration is for potential complications that might occur from the abdominoplasty. Insurance will most likely not cover the fees required to fix the complications.
Case 5: A healthy patient comes in requesting to have his facial appearance changed to better resemble the features of an animal. The surgeon’s own assessment and that of a psychiatrist deems him to have capacity. What are the surgeon’s ethical obligations in this situation?
This hypothetical case raises the topic of the limits of patient’s self-determination. As described above, the clinical relationship should not be understood as patient’s “autonomy” versus physician’s “paternalism.” Rather, the patient-physician relationship is a joint venture with a common goal: the patient’s well-being.
In a case like this, the physician should attempt to present specialized information in a simplified manner and engage the patient in a dialogue to ensure patient’s understanding of the immediate and long-term sequalae of the request.s. Literatur The surgeon should investigate the rationale behind the request but is under no ethical obligation to perform a surgery to accommodate a request that he or she deems neither necessary nor reasonable.
The principle of beneficence presupposes that persons other than the patient himself/herself is able apprehend what ought to be good for the patient. Hence, due diligence and discernment are an ethical obligation on the part of the surgeon when entertaining requests by patients. A request should not be fulfilled simply on the basis that it is what the patient wants.
Ethicists have attempted to show that, even if individual choice is given absolute value (a dubious position), paternalism in some forms can still be justified.s. Literatur Furthermore, Opinion 2.19 of the AMA Code states: “Physicians should not provide, prescribe, or seek compensation for medical services that they know are unnecessary.”s. Literatur
The stronger moral imperatives in this case include exposing the patient to unnecessary risk of harm (nonmaleficence) and pursuing the patient’s well-being (beneficence), which may require more inquiry as to the reasons behind the request.
This patient can be referred to another psychiatrist to obtain a second opinion about capacity.
Risk management can also be involved prior to any surgical intervention.
Case 6: A patient is admitted to the hospital in fulminant septic shock due to an infected limb. The patient is not conscious but has on multiple occasions expressed that he or she would rather die than live without a limb. The patient’s family is present and requests amputation of the limb. The multidisciplinary care team agrees that, medically, amputation of the infected limb would be an important step to controlling the infection. What are the ethical considerations?
If faced with this situation, the hospital’s Risk Management, Ethical Committee, and Psychiatry teams need to be involved immediately. This is not a decision that should be made solely on the plastic surgeon’s assessment and plan.
The distinction between withholding life-sustaining treatment and physician-assisted death/suicide is one around which there is now a significant consensus in law and ethics. The consensus is that it is not a moral violation to withdraw or withhold medical treatment that has been refused in a valid manner.s. Literatur This consensus also accepts a distinction between withholding/withdrawing life-saving care and physician-assisted suicide. According to the Opinion 2.20 of the AMA Code, “There is no ethical distinction between withdrawing and withholding life-sustaining treatment.”s. Literatur
The debate was initially spurred by the case of Karen Ann Quinlan in 1976, a young woman who remained in a persistent vegetative state and whose parents argued, against the wishes of her husband, for the removal of life-sustaining treatment (i.e., ventilator). The concept of “extraordinary means,” which has roots in Catholic moral theology, played a big role in this case and essentially elaborates that patients and families are under no ethical burden to pursue unduly burdensome treatment in order to prolong life. The legal consensus on this topic was formed around several decisions by the U.S. Supreme Court, especially after the Cruzan Case of 1990.
With regard to the case at hand, the patient’s wishes are known. Amputating one or more limbs to sustain his or her life would amount to extraordinary means. Withholding this would not—legally or ethically—amount to wrongdoing by the physicians involved in this care. However, there are many social complexities. Physicians should always seek consensus with and among family members. Involving the institution’s ethics committee early on is certainly warranted in this situation.
Case 7: A patient requests an elective surgical procedure. The surgeon feels that performing this procedure would conflict with his or her personal beliefs. What are the surgeon’s ethical obligations to the patient in this case?
Principle VI of the AMA Code states, “A physician shall, in the provision of patient care, except in emergencies, be free to choose whom to serve, with whom to associate, and the environment in which to provide medical care.”s. Literatur
Most states have legal provisions (so-called “conscience clauses”) allowing physicians to refuse provision of certain types of care based on moral/religious grounds. The Department of Health and Human Services (HHS) has in recent years put forth regulations that do not require physicians to provide referrals to providers who will provide the care the patient is seeking.
Legal requirements aside, the surgeon in this case does have ethical obligations to the patient which include beneficence and justice. Furthermore, professionalism requires courtesy that extends beyond one’s personal beliefs. In most cases, it is in the best interest of the patients that they be referred to an accommodating provider or that they be counseled regarding the options that are available to them in this situation. As one bioethicist put it, “Accepting a collective obligation does not mean that all members of the profession are forced to violate their own consciences. It does, however, necessitate ensuring that a genuine system for counseling and referring patients is in place, so that every patient can act according to his or her own conscience just as readily as the professional can.”s. Literatur
Case 8: What are some of the ethical considerations of a plastic surgeon who is active on social media?
The ASPS Code of Ethics explicitly prohibits any form of public communication that contains “a false, fraudulent, deceptive, or misleading statement or claim.”s. Literatur
This includes images that have been altered—post-production or by use of photographic techniques such as lighting and perspective—so as to misrepresent a condition or improvement. The Code condemns any public communication that “is intended or is likely to attract patients by use of exaggerated claims.”s. Literatur Surgeons should also disclose if the results shown are not typical.
Informed consent should be acquired, and part of this requires that the patient understands that images or videos posted online are potentially irrevocable, even if deleted by the person who uploaded them.
Social media posts that do not honor the profession of the surgeon and which, most importantly, do not honor the patient-physician relationship, are considered “medutainment” and should be avoided.s. Literatur Some authors have shown that public perception of the importance of a plastic surgeon’s role in patient care is extremely low, and that “medutainment” further undermines the professional reputation of plastic surgery.s. Literatur Plastic surgeons must be especially cognizant of “sexualization” of the body, which is much more likely to occur in the context of social media as compared to journal articles.
Any public communication that “appeals primarily to layperson’s fears, anxieties, or emotional vulnerabilities” is also condemned by the ASPS Code.s. Literatur
Naturally, interacting with social media requires corresponding compliance with the Health Insurance Portability and Accountability Act (HIPAA). It also requires familiarity with institutional policies, which may vary.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


