Case 54 Flexor Tendon Laceration
54.1 Description
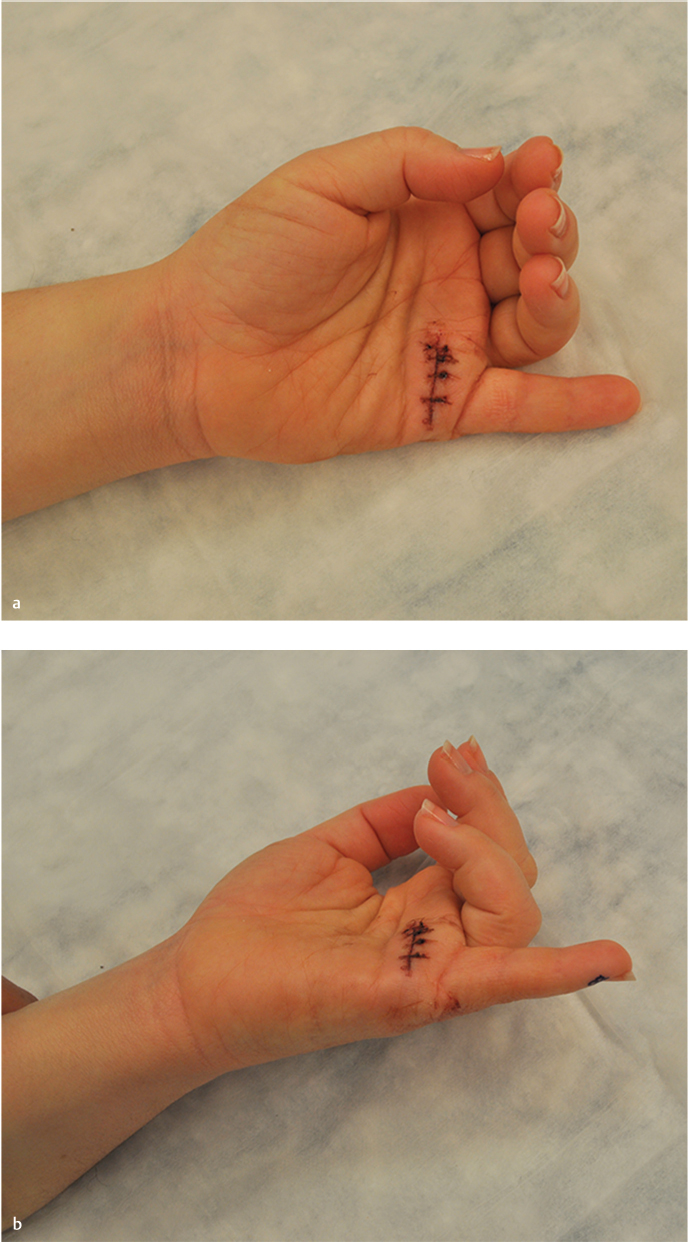
Abnormal resting cascade of the hand involving the left small finger
Laceration over the volar distal palm, distal to the distal palmar crease, likely in proximal zone 2
Images show lack of active flexion of the distal interphalangeal joint (DIP) and proximal interphalangeal (PIP) joint and loss of cascade
Rule out injuries to nerves, lumbricals, vessels, or tendons to small and ring fingers as well
54.2 Work-Up
54.2.1 History
Mechanism of injury (sharp, blunt, or avulsion)
The position of the hand at the time of injury (flexed vs. extended position)
Numbness or tingling (question whether patient had local anesthetic injected)
Significant bleeding at time of injury
Suggests arterial and digital nerve injury
Time elapsed since injury (e.g., 2 days vs. 2 months)
Right hand dominant versus left hand dominant
Any additional or associated injuries
Occupation and hobbies
Prior injuries or associated medical problems especially to hands
Comorbidities and social history (drug/alcohol abuse)
54.2.2 Physical Examination
Resting cascade of the hand: Interphalangeal joints should maintain flexion with arc increasing as examination moves ulnarly
Tenodesis (especially important to check with child/obtunded patient)
Passive wrist extension results in flexion of the fingers
Lack of flexion of the lacerated finger demonstrates discontinuity of flexor tendons
Level of laceration and likely zone of injury (e.g., laceration over center of middle phalanx, likely zone 1 and flexor digitorum profundus [FDP] only repair)
Separately assess active flexor action for all fingers
Flexor digitorum superficialis (FDS): The examiner maintains other digits in extension while attempting flexion of injured finger to isolate the FDS
FDP: The examiner maintains the PIP in extension while attempting flexion of the DIP
Flexor pollicis longus (FPL): In the setting of an injured thumb/palm, the examiner maintains the metacarpophalangeal joint (MCP) in extension while attempting flexion of the interphalangeal joint (IP)
Sensibility: Radial and digital nerve injuries
Perfusion of the digit: Absence of perfusion would prompt emergent intervention
54.2.3 Pertinent Imaging or Diagnostic Studies
Standard three-view X-rays (anteroposterior, lateral, and oblique) of the hand should be obtained to assess for fracture or foreign bodies
54.3 Patient Counseling
Patient should be counseled on critical importance of postoperative compliance with splinting and hand therapy. Potential complications should be reviewed
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


