Case 49 Acute Burn Injury

49.1 Description
Acute burn injury to portions of the face, chest, back, abdomen, bilateral arms and legs, and groin
Superficial and deep partial-thickness burns
Approximately 65% of body surface area
Possible circumferential involvement of the forearms
Concern for inhalation injury
49.2 Work-Up
49.2.1 History and Physical Examination
Trauma evaluation
ABCs (airway, breathing, circulation): Assess for critical injuries during the primary survey
Mechanism of injury
Flame: Most common; can lead to superficial to deep burns, depending on degree of exposure
Oil or grease burns: Must be careful not to underestimate the severity of such burns; oil will continue to burn over longer period of time if not washed off immediately
Electrical (high or low voltage): Raises concern for deeper injury to underlying structures
There is a greater concern for compartment syndrome and rhabdomyolysis (see Chapter 50)
Inhalation injury
Examine for singed facial hair and/or soot in the airway
History of asthma or chronic obstructive pulmonary disease (COPD) can compromise oxygenation
Have a low threshold to intubate patients with any evidence of inhalation injury
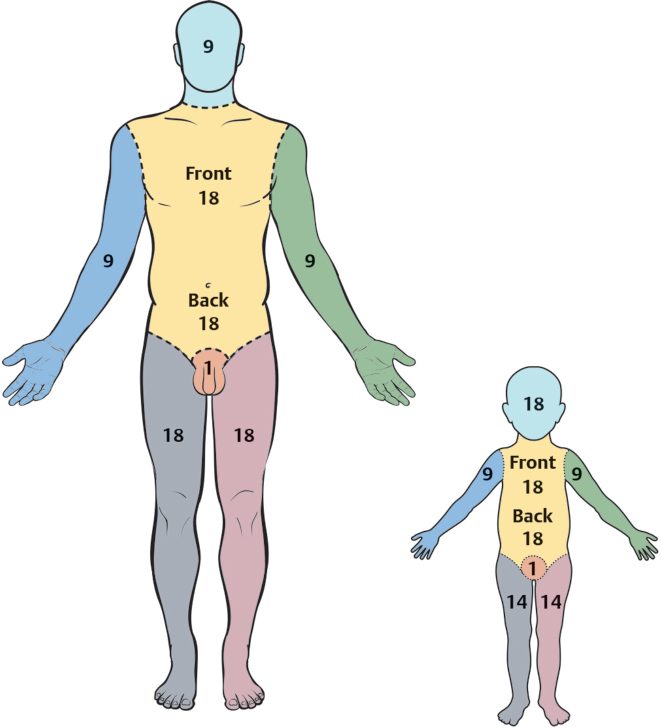
Extent of burn
Rule of Nines: Calculation of extent in percentage of total body surface area (%TBSA) based on second- and third-degree burns; does not include first-degree burns (see Fig. 49-1)
Assess depth of burn: Partial (superficial or deep) versus full thickness
If electrical: Identify entry and exit wounds; determine path of injury
Extremities involved
Circumferential burns: Assess need for escharotomies or fasciotomies
Escharotomies for superficial burns to release tight, leathery burned skin
Fasciotomies when injuries are deep (as in electrical burns); fascial release to prevent necrosis of deeper structures
Compartment syndrome
Compartmental pressures may be measured with STIC pressure monitor (Stryker; Kalamazoo, MI)
Concern if pressures are>30mmHg
Face involved
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


