Case 26 Lower Eyelid Ectropion (Involutional and Paralytic)

26.1 Description
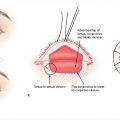
Sagging and eversion of the left lower eyelid margin
Loss of apposition of the eyelid and lower punctum to the eye
Tearing and some evidence of ocular irritation
26.2 Work-Up
26.2.1 History
History of ocular irritation, conjunctival irritation (eye redness), keratopathy, epiphora (excessive tearing), ocular trauma, eye or eyelid surgery, or facial paralysis
History of chronic eye irritation
26.2.2 Physical Examination
Evidence of sagging or eversion of the lower eyelid margin
Search findings to classify etiology of ectropion
Involutional, cicatricial, paralytic, mechanical
Evaluate lateral canthal tendon
Can be lax or detached
Occasionally associated with medial canthal tendon laxity and/or dehiscence or detachment of the lower eyelid retractors
Snap back test
Pull lower eyelid down and away from globe and observe length of time to return to original position
Ectropion is significant if the eyelid does not immediately snap back or does not return to original position
Eyelid distraction test
Laxity: Lower eyelid can be pulled away from the eye by more than 6 mm
Medial canthal laxity test
Pull lower eyelid laterally
Punctum should not move laterally by more than 1 mm
Lateral canthal laxity test
Pull lower eyelid medially
Lateral canthal angle should not move medially by more than 2 mm
Assess orbicularis oculi strength
Bell’s phenomenon (palpebral oculogyric reflex)
Ask patient to close eyes while holding eyelids open
Observe for upward and outward movement of eye upon eye closing
This protects the cornea when the eyes are closed
Slit lamp examination with fluorescein to evaluate for corneal epithelial disease
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


