Case 15 Unilateral Cleft Lip Deformity

15.1 Description
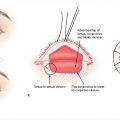
Complete left-sided, unilateral cleft lip deformity
Cleft nasal deformity: Nostril is widened and slumped (alar cartilage is inferiorly, posteriorly, and laterally). The nasal tip is bulbous and shifted toward the cleft.
Septal deformity: The septum and columella are shifted away from the cleft.
Alveolar cleft visible
Complete unilateral cleft palate inferred based on wide alveolar defect
15.2 Work-Up
15.2.1 History
Family history of orofacial clefting
Feeding difficulties, confirm appropriate weight gain
Additional medical problems/congenital abnormalities and associated syndromes
15.2.2 Physical Examination
Evaluate involved structures (lip, alveolus, palate)
Lower lip pits: Van der Woude syndrome (autosomal dominant)
Evaluate for associated birth anomalies consistent with a syndromic presentation
15.2.3 Diagnostic Studies
Only if there is concern for other systemic illness or syndrome
15.2.4 Consultation
Best managed by a multidisciplinary team: Plastic surgery, pediatric otolaryngology, speech pathology, child psychology, audiology, genetics, pediatric dentistry, orthodontics, maxillofacial surgery, social work, and nursing
Genetic evaluation if additional congenital abnormalities are present
15.3 Patient Counseling
Cleft care is best managed via a multidisciplinary team
Discuss the likelihood of several surgeries over the child’s lifetime (see Table 15-1 for cleft management timeline)
Feeding: Critical aspect of cleft care
Specialized nipples/bottles: Dr. Brown bottle, Haberman nipple (with a squeezable tip) or Pigeon nipple (with crosscut opening for faster flow)
Molding: Narrows cleft to optimize repair
Not employing any molding technique is also a reasonable option
Lip taping: With steri-strips or commercially available devices (such as DynaCleft)
Nasoalveolar molding (NAM)
Passive molding appliance rapidly becoming the gold standard for optimizing nasal shape
Alveolar molding alone takes place until alveolar ridges are 5 mm apart, then nasal prongs are attached to improve the shape of the nose
Latham appliance
Active molding appliance which expands palate and retracts premaxilla
Less commonly used due to concerns regarding maxillary growth
Lip adhesion
Performed surgically, in place of molding techniques
Preliminary repair of skin with or without muscle between ages of 6 weeks and 3 months
Goal: Minimize tension during the definitive cleft repair performed around 3–6 months of age
Cleft lip repair: Approximately at the age of 3 months
Rule of 10s: 10 lb of weight, 10 grams of hemoglobin (Hb), 10 weeks of age
May be delayed secondary to molding (NAM) or earlier lip adhesion
Cleft palate repair: Approximately 1 year of age
Earlier repairs favor speech but potentially compromise maxillary growth
The opposite is true for palatoplasty after 18 months of age.
Alveolar bone grafting
Performed during period of mixed dentition (roughly 7–10 years old), after appropriate orthodontics
Cleft nasal/septal reconstruction
Optimally performed once the patient has reached skeletal maturity. Can be combined with “touch up” procedures to optimize appearance.
Septoplasty is frequently deferred until this time.
Elaborate on the need for long-term follow-up through the Cleft Team
Assess for appropriate development and absence of negative outcomes, such as velopharyngeal insufficiency (see Chapter 17) or maxillary hypoplasia, requiring jaw surgery.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


