Case 12 Cheek Reconstruction

12.1 Description
Following resection, roughly 2 cm full-thickness defect of the right cheek, abutting the inferolateral border of the right lower eyelid
Does not appear to violate superficial musculoaponeurotic system (SMAS) into deeper structures
Moderate skin laxity on examination
12.2 Work-Up
12.2.1 History
Malignancy: Timeline of presentation
Sun and environmental exposure history
Personal and family history of skin cancer
Genetic conditions: Xerodermapigmentosum, Gorlin’s (nevoid basal cell) syndrome, albinism
Complicating comorbidities: Cardiopulmonary/peripheral vascular disease, diabetes, tobacco/steroid use, previous surgery or irradiation, anticoagulation, transplant recipient
12.2.2 Physical Examination
Lymph node examination to check for metastatic disease
Wound characteristics (hair bearing areas, adjacent skin laxity)
Confirm absence of involvement of deeper structures (e.g., parotid, facial nerve)
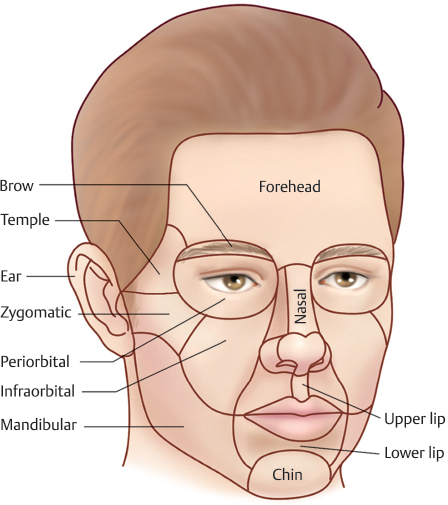
Facial subunit involvement (Fig. 12.1)
12.2.3 Diagnostic Studies
If patient presents initially without resection, a biopsy should be performed to establish a diagnosis.
Full-thickness incisional versus excisional biopsies may be performed. Avoid shave biopsies.
12.3 Patient Counseling
Patients must understand that some degree of asymmetry is to be expected following reconstruction as the surgeon must somehow make up for the absence of tissue.
While flap reconstructions may yield the most aesthetic results, it is reasonable for some patients (e.g., medically complicated, elderly) to opt for simpler skin graft reconstructions or even no reconstruction at all.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


