28 Buttock augmentation
Synopsis
Micro fat grafting














Introduction
• Buttock augmentation is major surgery, with the potential for significant complications.
• The overall goal of buttock augmentation is to achieve a more youthful appearance and contour and to create the ideal waist-to-hip ratio of 0.7.
• There are three acceptable methods of buttock augmentation: (1) silicone implants placed in the intramuscular plane; (2) silicone implants placed in the subfascial plane; and (3) autologous micro fat grafting (MFG).
• A fourth method of buttock augmentation, subcutaneous placement of buttock implants, is solely mentioned so it can be condemned due to the unacceptably high complication rate.
• Each method of buttock augmentation carries its own set of indications, risks, surgical equipment needs, and complications.
• Preoperative planning and the surgical technique used should be patient-specific with regard to individual anatomy and patient desires.
• Preoperative markings are crucial in guiding the surgical procedure and should be performed with the patient in a standing position.
History
Buttock augmentation advanced with the advent of autologous fat grafting, first reported by Chajchir and colleagues in 1990.1 Since then, there has been an increase in the literature documenting that there is one female body shape that is universally found to be most attractive, with the buttocks as one of the two most important determinants of beauty of the female torso. This attractiveness is directly related to the proportion of the waist to the buttocks, or the waist-to-hip ratio.2,3
Patient and physician interest gradually escalated during the late 1990s and through to today.4–6 Over that time, there has been an evolution in gluteal augmentation, with modifications in the approach, understanding of the various anatomical planes for implant insertion, and improvement of the surgical technique for implant-based augmentation.7–12 The implants themselves have evolved with different silicone elastomers, shapes, sizes and projection, making it possible to individualize the implant for each patient. Likewise, there has been refinement of the autologous fat grafting technique to improve fat survival, minimize complications and optimize outcomes for patients.13–16
Basic science
Gluteal aesthetic ideals
The attractiveness of the buttocks is not judged in isolation, but in proportion to the waist. According to Singh,2 there is one female body shape that men universally find most attractive (full buttocks, narrow waist). These ideal female proportions are summarized as a waist-to-hip ratio of 0.7 (measuring the waist at its narrowest and the buttock at the level of maximum circumference). In addition to this overall proportional relationship, there are various characteristics associated with attractive youthful buttocks. These include: (1) A smooth inward sweep of the lumbosacral area and waist; (2) a very feminine cleavage as the buttocks separate superiorly and inferiorly; (3) maximum prominence on the vertical axis at the level of the mid to upper buttock, and on the transverse axis, at the junction of the medial and central thirds of the buttocks; (4) minimal infragluteal crease; and (5) no ptosis.13
Topographical anatomy
A thorough grounding in anatomy and aesthetics is essential when dealing with the gluteal aesthetic unit.17 We can all recognize attractive buttocks, but translating these aesthetics into words becomes a challenge. Dr Ralph Millard18 emphasized in his book, Principalization of Plastic Surgery, that in order to be successful in our surgical design, approach and ultimate results, we must first understand the beautiful – in this case, the ideal buttock.
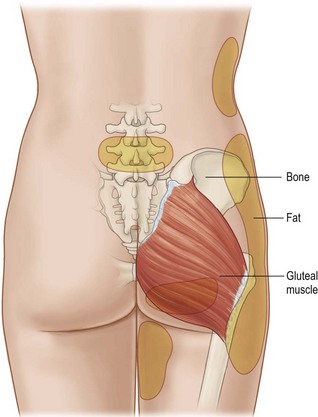
The gluteus maximus muscle originates primarily along the lateral margin of the sacrum and, to a lesser extent, from the coccyx and sacrotuberous ligament. The origin continues in an upward curvilinear fashion to the posterior iliac spine (identified as bilateral dimples in the parasacral zone); traditional teaching tells us that the muscle attaches all along the superior iliac crest, but in reality it only follows the crest for one-third of its initial distance. The superior limit of the gluteus maximus muscle is the posterior iliac spine. The gluteus maximus inserts into the iliotibial tract, and to a lesser degree, the greater trochanter (Fig. 28.1).
Aesthetic analysis
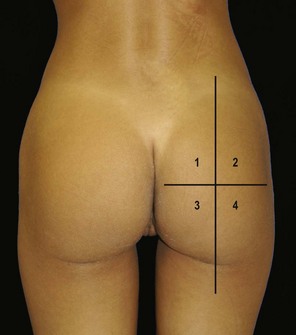
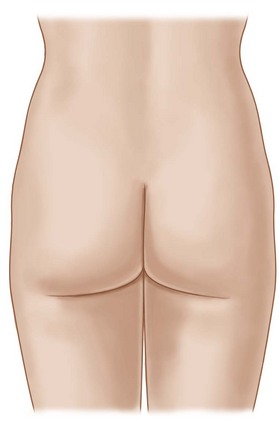
To further assess volume distribution, a horizontal mid-buttock line is added to divide the buttocks into four quadrants (Fig. 28.2). The ideal buttock also has equal volumes above and below this horizontal line. If we evaluate each quadrant individually, then the lower quadrants, three and four are equal, but tend to be slightly wider than one and two. In determining the best procedure for a particular patient, all four quadrants are evaluated as either sufficient or deficient.
Upper inner gluteal/sacral junction: ideal presacral space shape
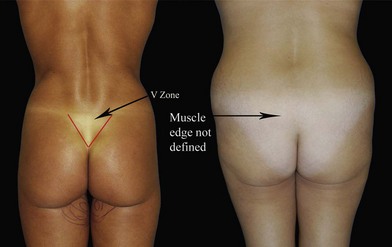
The inner gluteal/sacral space should be well defined so that a V-shape is apparent; this lower presacral space is appropriately called the “V” zone (Fig. 28.3). As the “V” zone becomes more visible, the buttock has greater aesthetic appeal. In the ideal buttock, the gluteal muscle edge should be well defined and have a semicircular upward turn. If this space is not well defined, the buttock becomes blunt and appears flat, especially on the lateral view.
Lower inner gluteal fold/leg junction
To describe this relationship, the intergluteal crease will be referred to as the midline. The upper aspect of the crease is easily identified; however, the inferior aspect is defined at the point where the buttock begins to separate from this midline. In the ideal buttock this occurs at about the bottom two-thirds to three-quarters of the muscle. The separation widens until it meets the inner leg junction. At this point the lower gluteal fold has a 45° take-off from the center intergluteal crease line and the inner gluteal fold/leg junction should create a diamond shape space (see Fig. 28.4). This is a key point in gluteal aesthetics.

As the lower inner gluteal fold and inner leg become fuller, it changes the 45° sloping line to a more horizontal position, which causes the diamond shape space to turn into a straight line, losing its aesthetic appeal (Fig. 28.4). As the fullness increases, it develops an inverse relationship creating an upward slope (negative angle) (Fig. 28.4). Improvement of this zone will depend on the severity of the fullness.
Lateral mid-buttock/hip contour
In the aesthetic buttock, the lateral mid-buttock is an area without any depression. This zone is categorized as having; no depression, mild depression, moderate or severe depression (Fig. 28.5).
Lateral view aesthetics
On lateral view, the presacral area should have a sweeping curve that has a lazy S shape (from the back to the bottom of the gluteus) (Fig. 28.6). Most of the gluteal volume is central and has equal distribution in the upper and lower gluteal zones, giving a C-shape curve. It has been suggested that the peak of the central mound should be at the level of the pubic bone (Fig. 28.7).
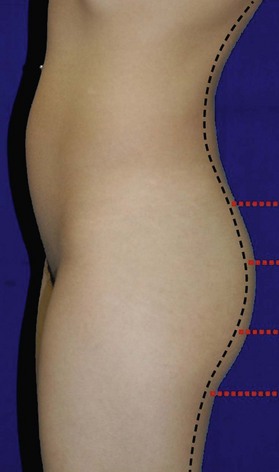

Determining where most of the volume lies (upper, central or lower buttock) will be important in deciding what procedure is best used to augment the buttock (Fig. 28.8).
Diagnosis/patient presentation
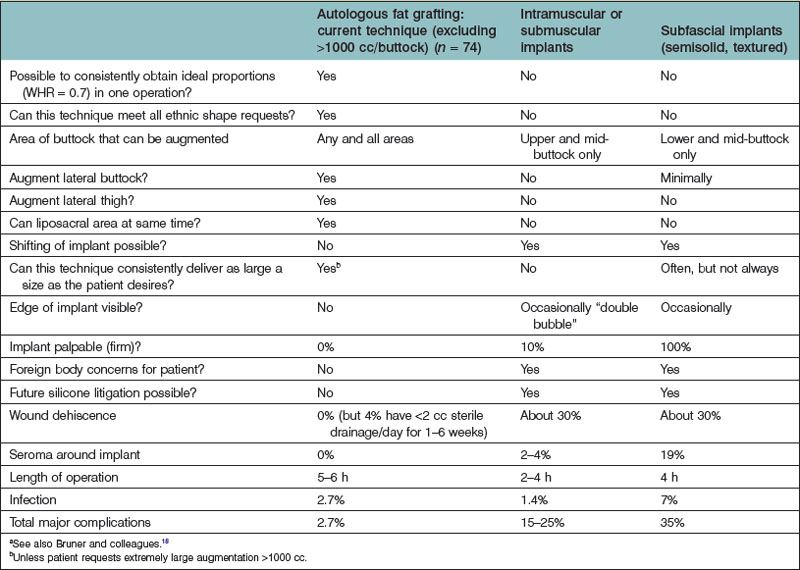
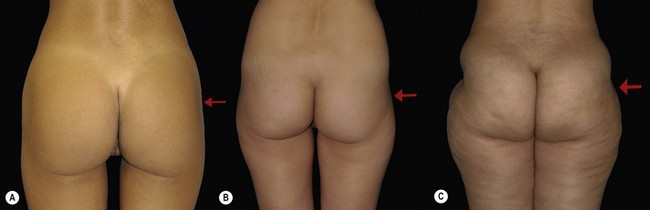
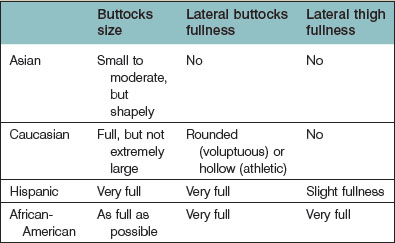
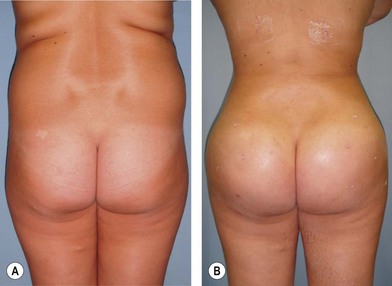
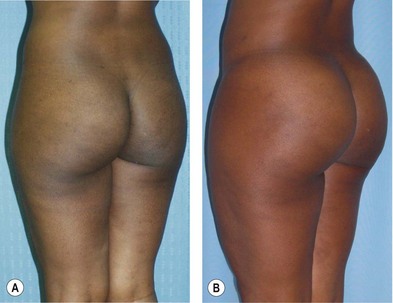
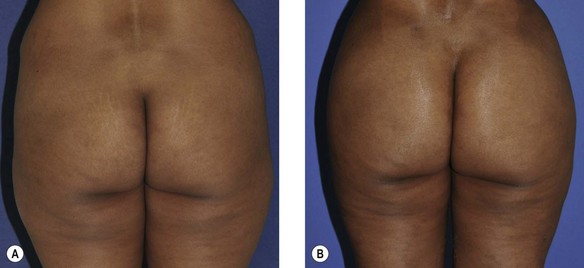
Ethnic ideals need to be taken into consideration regarding patient desires (Table 28.1).13 Some Caucasian patients may desire full, but not overly large buttocks which are rounded laterally (Fig. 28.9) or a trim, athletic appearance with hollow lateral buttocks. Some Asian patients may desire buttocks that are relatively small, whereas some Hispanic patients may prefer buttocks that are full and rounded medially and laterally, with lateral buttocks that are relatively full (Fig. 28.10). Some African-American and Caribbeans of African descent (Fig. 28.11) may desire larger buttock size, with fullness in the lateral buttocks and lateral thighs (“hips”).

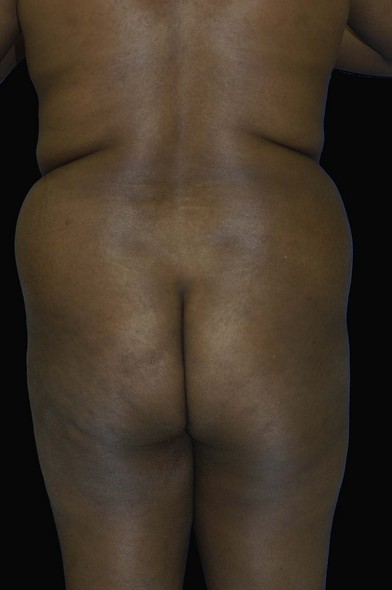
Gluteal augmentation is not just about making the buttock bigger, but rather accentuating, contouring, and reshaping. The focus becomes volume redistribution; shifting volume from an unattractive zone to a more desirable position. With this perspective, even the full-figured woman becomes a candidate since, on closer examination, the large buttock has maldistributed adiposity, with deficient volume in pertinent aesthetic zones (Fig. 28.12). The question is no longer who is a candidate, but rather, what reshaping method is best for each particular patient? Liposuction is for sculpting, while fat transfers and/or implants are used for volume expansion.
Patient selection
Early series on implant-based augmentation documented unacceptably high rates of would dehiscence and implant exposure. As patients requested greater augmentations, larger implants were used, resulting in higher complication rates. Patients were retrospectively stratified into various groups of body frames, based on size/BMI (Figs 28.13–28.16).9 The larger the body frame, the greater the risk of wound dehiscence and implant exposure



Aesthetic goals
Research by Singh, as well as other authors, has documented the importance of an ideal waist-to-hip ratio of 0.7.2 There is a tremendous synergistic effect of liposuction of the lower back, waist and flanks in conjunction with buttock augmentation to achieve this ideal waist-to-hip ratio. This is clearly evidenced by the fact that fuller, more shapely buttocks appear more attractive when the waist is slender rather than fuller.
In attractive female buttocks, there is beautiful cleavage as the buttocks separate superiorly. Furthermore, there is an inward sweep of the lower back, lumbar and sacral area, which accentuates this cleavage. It is also important to make the buttocks shorter vertically, than one would think. A short full buttock is attractive. A vertically long buttock simply appears big. (For a detailed summary of advantages and disadvantages of the various techniques for buttock augmentation see Table 28.2.)