Introduction
Breast reduction can be performed for either functional or cosmetic reasons. Optimal size, shape, symmetry, and scarring, as four primary goals, should be applied to each type of breast reduction; for example, breast size after breast reduction should be as the patient desired and in proportion to the patient’s body habitus. The shape after breast reduction should be cosmetically pleasing and long-lasting. Although the exact symmetry may be hard to achieve, most women desire a more symmetric result after breast reduction. It is also quite desirable to have minimal scarring after any type of breast reduction.
Medial pedicle breast reduction was promoted by Lejour from Belgium, but the procedure has been popularized by Hall-Findlay. , However, the medial pedicle breast reduction has been criticized by many plastic surgeons, especially in North America, for its inconsistent cosmetic outcome and higher revision rate. In addition, the learning curve for medial pedicle vertical breast reduction appears to be longer because many intraoperative adjustments should be done by the surgeon to produce a cosmetically acceptable final result.
In this chapter, the author describes his preferred technique for medial pedicle breast reduction, emphasizing patient selection and several technical refinements of the surgical technique.
Indications and Contraindications
It is the author’s opinion that medial pedicle breast reduction is not indicated for all patients. , In general, younger women with good breast skin condition (no stretch marks) and reasonably well-maintained round shape of the breast are good candidates for this type of breast reduction. ( Fig. 18.1 ). The overall amount of breast tissue reduction may not be a critical issue, although the average weight of this type of breast reduction is usually between 300 and 500 g for each breast. However, the distance from nipple to inframammary fold (IMF) should be less than 10 cm. For patients who are relatively older and have poor breast skin condition and elongated breast shape, the classic inverted- T inferior pedicle breast reduction, not the medial pedicle breast reduction, should be performed for more predictable results ( Fig. 18.2 ). Box 18.1 summarizes the indications for the medial pedicle breast reduction in the author’s practice.


- •
Younger and healthy women (not for all women)
- •
Good breast skin condition (no stretch marks)
- •
Reasonably maintained breast shape (still round, no grade III ptosis)
- •
Moderate-sized breast reduction (less than 500 g)
- •
Relatively short distance from nipple to IMF (less than 10 cm)
Preoperative Evaluation and Special Considerations
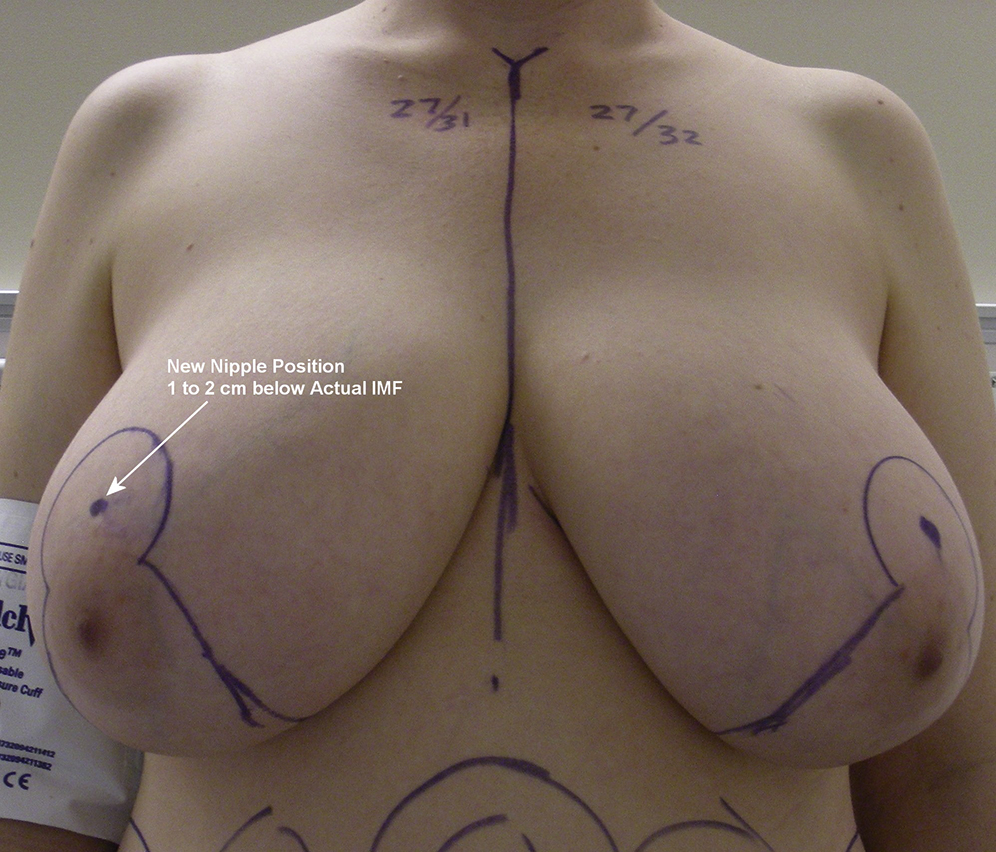
Unlike the classic inverted- T inferior pedicle technique, the medial pedicle breast reduction does require some special considerations and more intraoperative adjustments. For example, the new nipple position should be placed “lower” during the preoperative marking because the vertical technique in general has a tendency to place the nipple too high and to create more upper pole fullness after such a breast reduction. Therefore, the surgeon should pay particular attention to avoiding a high-riding nipple and inform the patient about the temporary appearance of the breast postoperatively.
The new IMF should be placed higher than the actual IMF, so the distance between the nipple and the IMF can be shortened. This distance can be shortened further by a running subcuticular closure. However, the distance between the nipple and the new IMF will never be 5–6 centimeters as after the classic inverted-T inferior pedicle breast reduction. Frequently it will be about 7–8 centimeters, so an optimal breast shape after reduction can be maintained.
The management of the excess tissue in the lower pole of the breast can be critical to the success of the medial pedicle breast reduction. The surgeon should pay attention to this important issue and develop a strategy or technique to properly remove the extra tissue in this part of the breast ( Box 18.2 ).
- •
Place new nipple position “low”
- •
Create new but higher IMF
- •
More intraoperative adjustments
- •
Shorten vertical distance during closure
- •
Manage “excess” tissue in the lower pole
- •
May have temporary upper pole fullness
Surgical Techniques
Relevant Surgical Anatomy
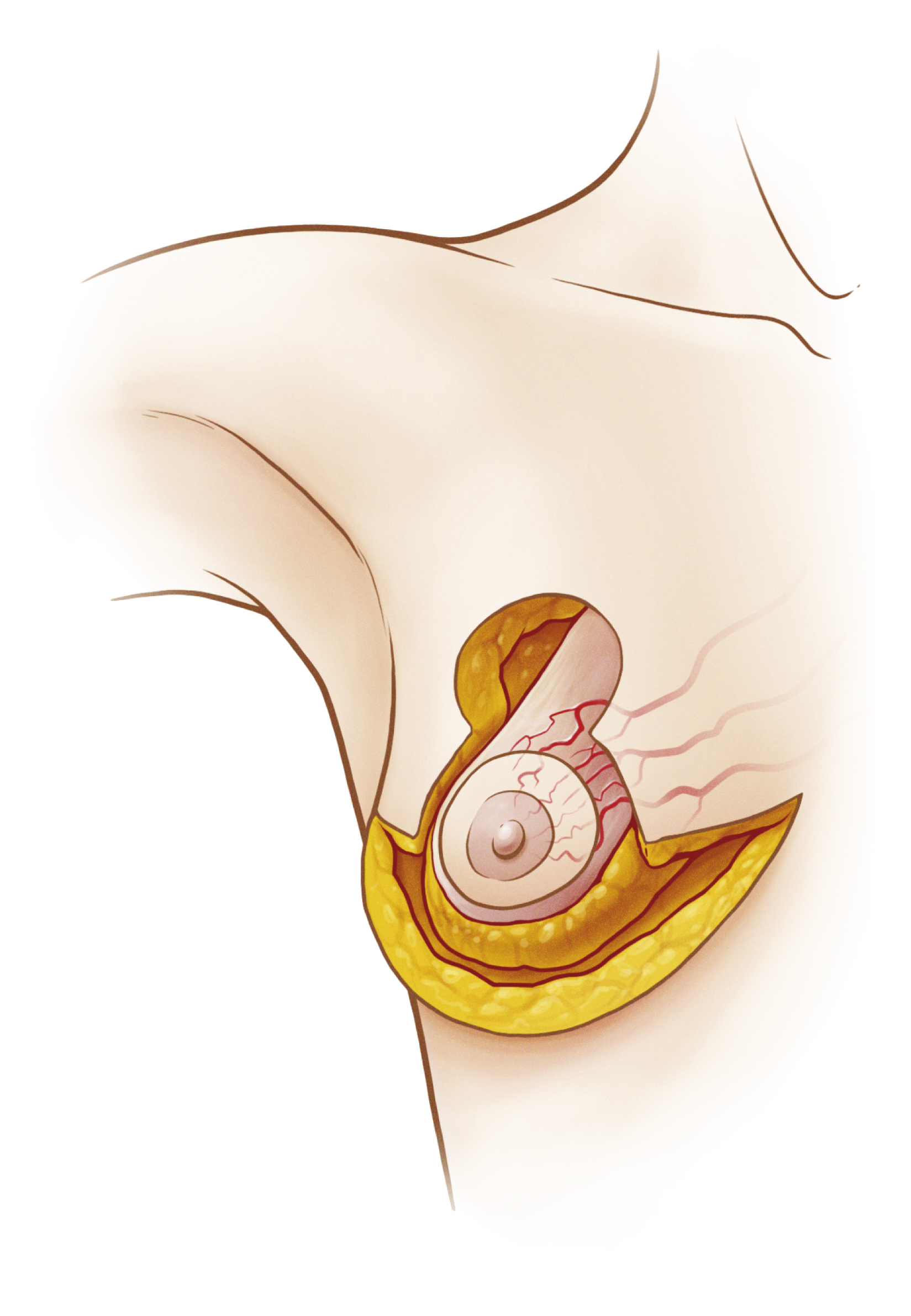
The breast is an ectodermal structure contained in a superficial fascial system. It is formed by about 20–25 individual lobules that connect to the nipple. The blood supply in general comes in from several directions. The main blood supply to the breast is based on medial branches of the internal mammary artery. The medial pedicle receives its blood supply from the perforators of the internal mammary vessels. The perforators in general provide a robust blood supply to the pedicle, so necrosis of the nipple–areolar complex is rare after a medial pedicle breast reduction as long as adequate pedicle width is maintained ( Fig. 18.3 ). The veins of the breast rarely accompany the arteries. Much of the breast is drained by a superficial venous system that lies just under the dermis. The nipple is primarily innervated by the medial and lateral branches of the fourth intercostal nerve. However, the third and fifth intercostal nerves also contribute.
Preoperative Markings
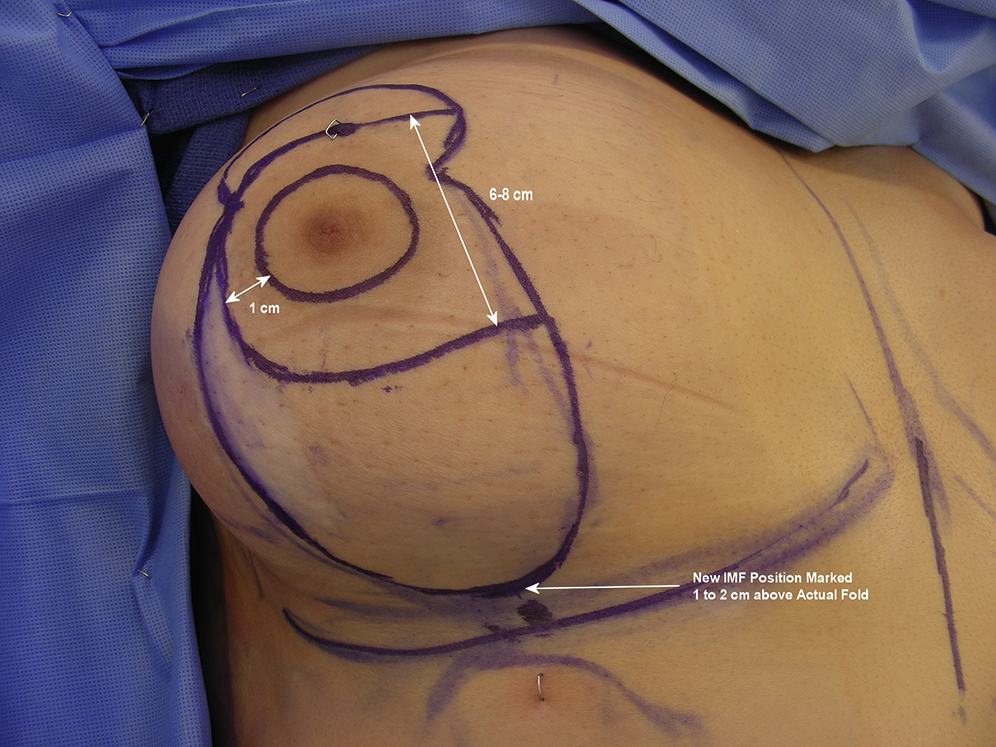
While the patient is in the upright position, the new nipple position should be marked first. However, unlike classic inverted-T inferior pedicle breast reduction, the new nipple position should be set at least 1 or 2 cm below the level of IMF to avoid a high-riding nipple position after this type of the breast reduction. In addition, if the patient has good upper pole fullness, the new nipple position should be marked lower than as intended to avoid high-riding of the nipple. The circle around the new nipple position is marked with a Wise pattern marker as used by the author. This would make the diameter of the circle about 40 mm. The level of the new IMF is determined to be about 2 cm above the actual IMF. After this, the medial and lateral borders of the resection are marked by rotating the breast both medially and laterally in reference to the midline of the breast ( Fig. 18.4 ).
Intraoperative Markings
While the patient is in the supine position, commonly under general anesthesia, the nipple–areola complex is marked with a 38- or 42-mm cookie cutter. The pedicle is then designed with the pedicle width between 6 and 8 cm depending on the breast size the surgeon wants to achieve after breast reduction. It is important to leave at least a 1-cm-wide area of breast tissue away from the proposed upper border of the nipple–areolar complex to avoid cutting into it. Ideally, the width of the pedicle should be marked in such a way that half of it is within the areola opening and the other half is within the area bounded by medial and lateral pillars ( Fig. 18.5A ). After the pedicle is marked, the new circle of the proposed nipple–areolar complex and also the medial and lateral markings of the proposed resected area in the breast are tested for easy approximation without tension.