The options for breast reconstruction following mastectomy continue to expand. Prosthetic devices and pedicled musculocutaneous flaps provide patients with good outcomes but have limitations that preclude their use in patients with a history of cigarette smoking or prior radiation, or in patients who are overweight or obese. The primary limitations of pedicled musculocutaneous flaps are that they usually require total sacrifice of the muscles, result in donor-site weakness, and sometimes yield abnormal contour. The primary limitations of prosthetic devices are that they are foreign materials and are subject to mechanical failure eventually.
Free tissue transfer overcomes the limitations described above but is associated with morbidity related to technical factors. Free flaps for breast reconstruction are generally consideredin women with increased body mass index (BMI), ahistory of tobacco use, prior radiation therapy, and also inwomen who desire preservation of the donor-site muscles. These flaps are derived from a variety of donor sites that include the abdomen, gluteal region, and medial thigh. Free flaps can be muscle or perforator based.
The principal abdominal free flaps include the free transverse rectus abdominis musculocutaneous (TRAM), deep inferior epigastric artery perforator (DIEP), and superficial inferior epigastric artery (SIEA) flaps. Other donor sites for free flap breast reconstruction include the gluteal and medial thigh regions. Although these latter sites can be considered as primary donor sites, most surgeons consider these when the abdomen is not an option. The gluteal flaps include the inferior gluteal artery perforator (IGAP), superior gluteal artery perforator (SGAP), and the gluteal musculocutaneous flaps. The thigh flap to be reviewed is the transverse upper gracilis (TUG) flap or transverse musculocutaneous gracilis (TMG) flap. The anterolateral thigh and Reuben’s flap are seldom used for breast reconstruction and will not be reviewed in this chapter.
This chapter focuses on patient selection, anatomic considerations, harvesting techniques, and clinical outcomes. Other relevant topics include a review of algorithms, monitoring techniques, and the current technological advancements that have facilitated these complex operations.
PATIENT SELECTION AND FLAP SELECTION
Patient and flap selection includes a thorough history and physical examination, review of the reconstructive options, an understanding of patient expectations, and the surgeon’s recommendations.1,2Important details of the physical examinationinclude body weight, patient height, BMI, and anestimate of breast volume requirements. The possibility of secondary operations involving the ipsilateral and/or contralateral breast is discussed. The variety of available donor sites allows appropriate volume to be transferred in most patients. The abdomen is the preferred donor site for most surgeons and patients if sufficient skin and fat are available given the desired breast volume. Most patients have had children and have some excess abdominal skin and fat. A slender woman with a paucity of abdominal fat may still be a candidate for an abdominal flap if the reconstructive requirements are low. Women who are overweight or obese may not be candidates for pedicled abdominal flaps but may be candidates for a free TRAM or DIEP flap. The flap, however, must be tailored to sustain adequate perfusion and minimize fat necrosis.3,4 The abdomen is usually not considered when a significant volume is required and midline scars preclude incorporating the contralateral zones.
If the abdomen is not suitable, then the gluteal or thigh region is considered. The SGAP or IGAP is considered in patients who desire autologous reconstruction, lack sufficient abdominal fat, refuse prosthetic reconstruction, and prefer a perforator flap.5,6 Most women will have sufficient donor fat in the gluteal area. An alternative to the gluteal flaps is the TUG flap.7,8,9 The principal limitation with all of these alternate flaps is that the volume is usually limited compared with the abdominal donor site. One advantage compared with the abdomen, however, is that these flaps are available on both sides of the body, permitting separate procedures if necessary.
Patient age, in and of itself, is not an indication or contraindication for any one operation. Advanced patient age (>65 years) may be a relative contraindication for microvascular breast reconstruction, but personal experience, and the existing literature, demonstrates that these techniques are safe and effective in properly selected patients in this age range.10 Women of advanced age are required to obtain medical clearance from their primary physicians. Women with multiple medical comorbidities are discouraged from pursuing complex microvascular procedures and directed toward simpler methods, such as prosthetic reconstruction.
The decision to use a perforator flap or a musculocutaneous flap can be difficult. This is especially true when considering the abdomen as the donor site. Some surgeons feel that all patients have a dominant abdominal wall perforator and that a DIEP flap can be performed in anyone. Others are of the opinion that a dominant perforator is not always present and a musculocutaneous flap is sometimes necessary. Several studies have described an algorithm for flap selection based on patient characteristics.2 Our original algorithm was based on breast volume, abdominal fat volume, perforator diameter, number of perforators, patient age, tobacco use, and whether the reconstruction was unilateral or bilateral. In general, a DIEPflap was preferentially performed when the volume requirementwas less than 750 cc and the patient had mild to moderateexcess abdominal fat. A free TRAM flap was preferentiallyperformed when the volume requirement exceeded 1,000 cc orthe patient had abundant abdominal fat. With increasing experience, this algorithm has been modified (Table 62.1).
The final component of the consultation includes a review of schematic illustrations and preoperative and postoperative photographs of other patients. Typically, the patient is shown a poor result, a good result, and an excellent result. Patients are informed of the potential complications including flap failure (0.5% to 4%), abnormal donor-site contour (0% to 20%), and return to the operating room (1% to 8%).
PREOPERATIVE IMAGING
With traditional musculocutaneous free flaps, there is little need to assess the vascular architecture of the flap or donor site. However, with the introduction of perforator flaps, preoperative imaging is useful. Over the past decade, there have been a variety of technological advancements that facilitate localization of perforators.11,12,13,14,15,16,17,18Preoperative imagingenables surgeons to identify suitable perforators and to determinethe patency of primary source vessels, namely the inferiorepigastric and internal mammary vessels. The modalities that are currently available include duplex and color duplex ultrasound, computerized tomographic angiography (CTA), and magnetic resonance angiography (MRA) (Table 62.2).
TABLE 62.1 AN ALGORITHM FOR SELECTION OF A FREE TRANSVERSE RECTUS ABDOMINIS MUSCULOCUTANEOUS, DEEP INFERIOR EPIGASTRIC ARTERY PERFORATOR, OR SUPERFICIAL INFERIOR EPIGASTRIC ARTERY FLAP
The first tool used for preoperative mapping was the Doppler ultrasound. Although there are many clinical applications for the Doppler, plastic surgeons were interested in the Doppler to map out perforating vessels throughout the cutaneous territory of a flap.11,19,20 There were several early studies utilizing the color Doppler that provided useful information related to the location, caliber, and flow patterns of the perforators in the planning of the TRAM flap.20 Cluster analyses demonstrated that perforators were located throughout the anterior abdominal wall with the majority of dominant perforators being situated in the periumbilical area.20 Perforators exceeding 2.2 mm were few in number but were identifiable in all four quadrants of the anterior abdominal wall.
Other benefits using Doppler included information regarding flow, direction, and velocity. In a study evaluating perfusion of the TRAM, DIEP, and SGAP flaps, it was determined that the highest blood flow and velocity was achieved in the TRAM flap followed by the DIEP and SGAP flaps.11 Specific flow measurements in various vessels were obtained and included in the deep inferior epigastric artery (10.45 mL/min), the superior gluteal artery (9.95 mL/min), and the internal mammary artery (IMA) (37.66 mL/min). The imaging could differentiate between venous and arterial signals.11The principallimitation of the color duplex was that it could not providethree-dimensional or architectural detail of the perforatorsystem. Giunta et al.19 reported a relatively high number of false-positive results (46%) using the hand-held Doppler for localization of perforators. In a comparative study evaluating Doppler ultrasound and CTA, Rozen et al.12 found that CTA was superior to Doppler based on visualization of the deep inferior epigastric artery (DIEA), its branching pattern, and the perforators.
TABLE 62.2 THE FOUR MODALITIES FOR PREOPERATIVE IMAGING OF THE PERFORATORS ARE LISTED
▪
TEST
▪
XR
▪
CONTRAST
▪
CALIBER
▪
LOCATION
▪
FLOW
▪
COURSE
▪
ACCURACY
Doppler
No
No
No
Yes
No
No
Low
Color duplex
No
No
No
Yes
Yes
No
Moderate
CTA
Yes
Yes
Yes
Yes
No
Yes
High
MRA
No
Yes
Yes
Yes
No
Yes
High
CTA, computerized tomographic angiography; MRA, magnetic resonance angiography.
Computerized Tomographic Angiography
Computerized tomography may represent the gold standard for preoperative imaging and was the first of the highly accurate methods of perforator assessment.13,16,17,21 Its use is primarily directed toward abdominal flaps but it can also be used in the gluteal and posterior thorax. Using multi-slice computerized tomography, axial and coronal images are obtained demonstrating the vascular architecture. The benefits of CTAinclude anatomic localization of the perforators, determinationof the course of the perforator through the muscle, comparativeassessment of the right and left vascular anatomy,and elucidation of anatomic detail of the medial and lateral row perforators. CTA can also provide information that may discourage a surgeon from performing a perforator flap and choose instead to perform a muscle-sparing (MS) free TRAM.
TABLE 62.3 THE VARIOUS ABDOMINAL INCISIONS AND THEIR CONSEQUENCES ON THE SUPERFICIAL INFERIOR EPIGASTRIC ARTERY, DEEP INFERIOR EPIGASTRIC ARTERY PERFORATOR, AND ABDOMINAL PERFORATORS ARE LISTED
▪
SCAR
▪
N
▪
SIEA DISRUPTION
▪
DIEA DISRUPTION
▪
PERFORATOR DISRUPTION
Laparoscopy
20
None
None
None
Open appendectomy
20
All (ipsilateral)
None (ipsilateral)
Medial row of DIEA
Pfannenstiel
35
Medial branch (30/35)
None
NR
Paramedian
3
All (ipsilateral)
All (ipsilateral)
All (ipsilateral)
Open choly
1
None
None
None
Midline
17
None
None
Crossover
SIEA, superficial inferior epigastric artery; DIEA, deep inferior epigastric artery; NR, not reported. From Rozen WH, et al. The effect of anterior wall scars on the vascular anatomy of the abdominal wall. Clin Anat. 2009;22:815-823.
Clinical trials using CTA have been useful. Casey et al.17 have demonstrated that preoperative CTA has reduced operative times, increased the number of suitable perforators included in a flap, and reduced the incidence of a postoperative abdominal bulge. The latter is presumably related to the selection of medial rather than lateral row perforators minimizing intercostal nerve injury. Unfortunately, CTA has notreduced complications related to the anastomosis, flap failurerates, occurrence of fat necrosis, dehiscence, or delayed healing. CTA has also demonstrated benefit in the setting of prior abdominal surgery. Rozen et al.16 studied 58 patients who had a total of 96 abdominal scars with CTA to determine if there was any disruption to the perforators or the primary source vessels. Their findings were that paramedian incisions resulted in most damage to the perforator, SIEA, and DIEA vessels. On the contrary, laparoscopic incisions caused the least damage (Table 62.3).
Magnetic Resonance Angiography
MRA represents the next generation in vascular imaging in part because the imaging quality is maintained or enhanced without ionizing radiation.15,18,22,23When compared withCTA, MRA has lower spatial resolution but greater contrastresolution.22 This enables MRA to detect very small perforatorsthat might otherwise be missed on CTA. MRA enables surgeons to become aware of perforator location, size, and distance from the umbilicus. Clinical studies have provided useful information. Greenspun et al.18 reviewed the outcomes in 31 women (50 flaps) scheduled for DIEP flaps. All perforators visualized on MRA using a gadolinium-based contrast agent were found intraoperatively. In 100% of patients, the intraoperative location of each perforator was within 1 cm of that predicted using MRA. In three flaps, the DIEA perforators were small and the SIEA system was relatively large. MRA successfully predicted the preferred use of an SIEA flap instead of the DIEP flap in three out of three women (100%). Other studies have demonstrated similar findings. Masia et al.15 used MRA without contrast for abdominal perforators. A dominant perforator was identified in 56 women having DIEP flap reconstruction. They were able to determine the location of the dominant perforator, define its intramuscular course, and reliably evaluate the SIEA. The intramuscular perforators originated from the lateral row in 55% and from the medial row in 31%.
Imaging of the gluteal and thigh perforators can also be performed. Vasile et al.23 used MRA in 32 buttocks and imaged 142 perforators. The superior gluteal artery was the source for 92 (57.5%) perforators, the inferior gluteal artery was the source for 56 perforators (35%), and the deep femoral artery was the source for 11 (7.5%) perforators. The authors demonstrated that MRA imaging determined the location and course of the perforating vessels and can be useful when choosing an inferior or superior gluteal perforator flap.
FREE FLAPS
Free tissue transfer can be accomplished from virtually anywhere in the body. When reconstructing the breast, there are certain criteria that make some flaps better suited than others. These criteria include adequate volume, ability to shape, adequate donor vessels, and donor-site considerations. The flaps that are reviewed in this chapter include the free TRAM, DIEP, SIEA, SGAP, IGAP, and TUG.
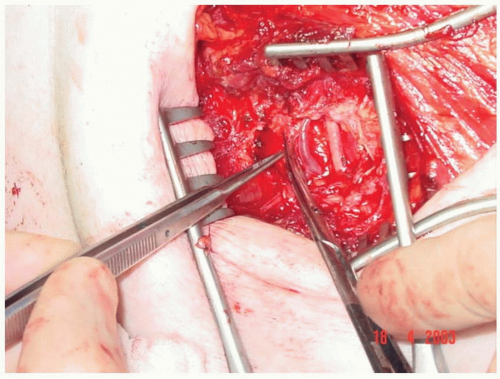
Integral to the selection of the flap for microvascular reconstruction is the selection of the recipient vessels. The most common recipient vessels are the internal mammary and thoracodorsal artery and vein.24,25,26,27,28The internal mammary vesselsare the vessels of choice in most cases because of ease ofexposure, compatible size match, maximum freedom for flappositioning, and excellent flow characteristics (Figure 62.1). The diameter of the internal mammary vessels at the level of the fourth rib ranges from 0.99 to 2.55 mm for the artery and 0.64 to 4.45 mm for the vein. In contrast, the diameter of the thoracodorsal vessels ranges from 1.5 to 3.0 mm for the artery and 2.5 to 4.5 mm for the vein.15,16 The blood flow rate of the IMA ranges from 15 to 35 mL/min (mean, 25 mL/min) and the blood flow rate of the thoracodorsal artery ranges from 2 to 8 mL/min (mean, 5 mL/min).
FIGURE 62.1. The internal mammary artery and vein are prepared as recipient vessels for the microvascular anastomosis.
TABLE 62.4 THE MUSCLE-SPARING CLASSIFICATION FOR FREE TRANSVERSE RECTUS ABDOMINIS MUSCULOCUTANEOUS AND DEEP INFERIOR EPIGASTRIC ARTERY PERFORATOR FLAPS IS SHOWN
▪
MUSCLE-SPARING TECHNIQUE
▪
DEFINITION (RECTUS ABDOMINIS)
MS-0
Full width, partial length
MS-1
Preservation of lateral segment
MS-2
Preservation of lateral and medial segment
MS-3 (DIEP)
Preservation of entire muscle
MS, muscle sparing; DIEP, deep inferior epigastric artery perforator.
Only gold members can continue reading. Log In or Register to continue