Introduction
Autologous options for breast reconstruction have greatly expanded since the initial descriptions of the latissimus dorsi musculocutaneous flap and the transverse rectus abdominis musculocutaneous (TRAM) flap. In many ways, these two flaps have provided the cornerstone for many of the autologous options that are currently available. Through ingenuity and innovation, plastic surgeons have pioneered a variety of flaps that are currently in use in order to reduce donor site morbidities and to maintain high aesthetic quality. Perforator and muscle-sparing flaps are now derived from virtually all territories of the body and include the abdomen, posterior and lateral thorax, gluteal region, as well as the medial and posterior thigh. Some of these flaps are robust and can provide large volumes for total breast reconstruction and others are ideally suited for partial breast defects.
Given the diversity in flap characteristics and the various donor sites, the ability to properly evaluate and select patients for autologous reconstruction is important. This entails evaluation of the anatomy, breast volume requirements, and donor site considerations. This chapter will focus primarily on the various autologous options that are currently in use for breast reconstruction with an emphasis on principles and techniques.
Anatomy of the Breast
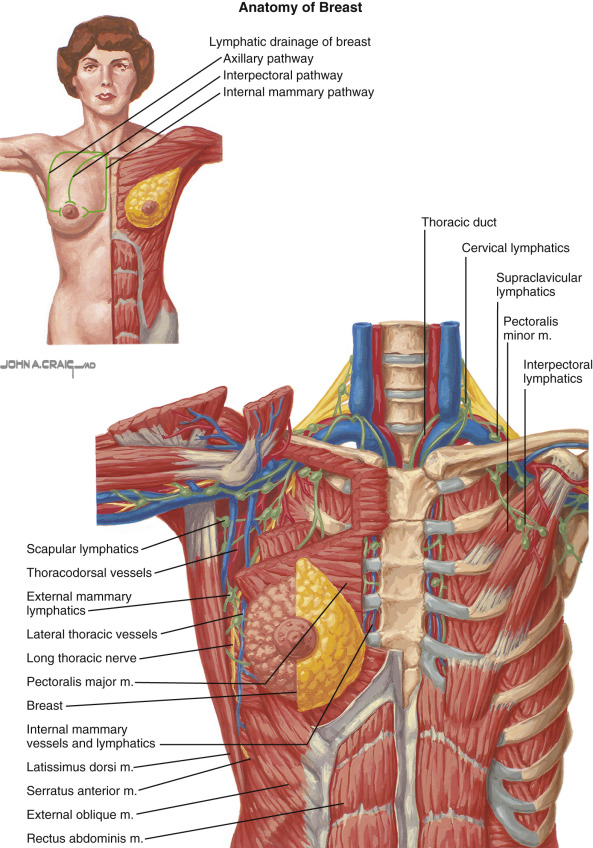
An understanding of breast anatomy is an important consideration for the reconstructive surgeon. The breast borders extend from the inframammary fold to the 2nd rib and from the midaxillary line to the medial sternal border ( Fig. 16.1 ). It is important to appreciate the natural footprint of the breast when considering autologous reconstruction. The breast is comprised of lobes, lobules, ducts, and fat that are enclosed within the investing fascia of the breast. Preservation of the subcutaneous adipose tissue and subdermal vascularity is important to maintain the quality of the post-mastectomy skin envelope. The vascularity of the breast is derived from multiple sources that include the internal and lateral mammary perforators, pectoral perforators, and the thoracoacromial vessels ( Figs 11.1 , 11.2 ). The innervation to the breast is via the medial and lateral pectoral nerves, as well as the long thoracic nerve. Cutaneous sensation to the breast is derived from the sensory branches of the 1st through 6th thoracic rami ( Fig. 11.2 ). Lymphatic ducts of the breast drain toward the axillary, supraclavicular, and internal mammary lymph node basins.
Preoperative Considerations
When evaluating women for autologous breast reconstruction, several factors should be considered that are related to specific characteristics of the patient and breast. These include breast volume and contour, body habitus, reconstructive volume requirements, donor site considerations, medical comorbidities, tumor characteristics, patient preferences and expectations, as well as the potential need for adjuvant therapy. Many women are now choosing to have prophylactic mastectomy and as a result, aesthetic expectations are high. Thus, it is important that plastic surgeons select options and operations that they are comfortable with, are safe and effective, are predictable and reproducible, and are associated with high rates of success and good outcomes.
Perhaps the most important determinant of a good outcome following autologous reconstruction is proper patient selection. With the myriad autologous options available and the wide variation in body habitus, there is usually a flap that will be suitable for most patients. With the epidemic nature of overweight and obese patients, the abdomen remains the most commonly used donor site for most plastic surgeons. Prior to flap selection, it is important to perform a thorough physical exam, calculate BMI, and obtain appropriate diagnostic tests on all patients considering breast reconstruction. In women with a BMI <30, immediate autologous reconstruction can usually be safely performed assuming that there is sufficient donor site tissue and that there are no oncologic contraindications. In patients with a BMI ranging from 30–39, immediate autologous reconstruction can still be performed but will be dependent upon other comorbidities such as diabetes mellitus and tobacco use, as well as cardiac or pulmonary disorders. In these patients, appropriate medical management and control of comorbidities is recommended before reconstruction is offered. In patients that are morbidly obese (BMI >40), immediate reconstruction is usually not recommended because of the higher incidence of adverse events. These patients are usually advised to proceed with the mastectomy but consider delayed reconstruction following a defined period of weight loss.
When considering flap selection, an important assessment on physical examination is a sufficient quantity of skin and fat in order to reconstruct a breast that will meet expectations. Although a woman may be slender with a paucity of fat, she may still be a candidate for autologous reconstruction if the breast volume requirements are low. In women who are overweight or obese, a flap can still be performed; however, the flap should be tailored to sustain its perfusion requirement and to minimize the incidence of fat necrosis. Abdominal flaps may be contraindicated in the presence of multiple scars, especially when located in the vicinity of the primary vascular pedicle or the principal adipocutaneous perforators. In these patients, preoperative vascular imaging should be considered. A large abdominal pannus or extreme lipodystrophy may also preclude autologous reconstruction. The most common autologous donor sites include the abdomen, posterior thorax, gluteal region, and thigh.
For women that are in need of partial breast reconstruction, the options are adjusted because the volume requirements are usually less. In these cases, the posterior or lateral thorax is usually considered rather than the abdomen because these donor sites supply less tissue than the abdomen and also because the abdomen is usually preferred for total breast reconstruction. Typical flaps for partial breast reconstruction include the latissimus dorsi (TD); thoracodorsal artery perforator (TDAP); intercostal artery perforator (ICAP); and internal mammary artery perforator (IMAP) flaps. An important consideration in these patients is the location of the defect. Most of these posterior thoracic flaps are excellent for lateral or inferior defects but may be not be possible for medial defects because of the limited arc of rotation. The IMAP flap is sometimes a better option for medially based defects.
Indications for Autologous Reconstruction
The indications for autologous reconstruction are variable and include women that do not want prosthetic reconstruction, have a sufficient quantity of donor site tissue, have had a prior failed prosthetic reconstruction, or have had prior radiation to the breast or chest wall. In the United States these women constitute approximately 25% of the patients who have breast reconstruction following total or partial mastectomy.
Preoperative Imaging
Preoperative imaging of the vascular architecture has been demonstrated to be useful for operative planning ( Table 16.1 ). It enables surgeons to identify suitable perforators and to determine the patency of primary source vessels. It is often considered for the abdominal and gluteal flaps. Imaging modalities that are currently available include duplex ultrasound, computerized tomographic angiography (CTA), and magnetic resonance angiography (MRA).
| Test | X-Ray | Contrast | Caliber | Location | Flow | Course | Accuracy |
|---|---|---|---|---|---|---|---|
| Doppler | No | No | No | Yes | No | No | Low |
| Color duplex | No | No | No | Yes | Yes | No | Moderate |
| CTA | Yes | Yes | Yes | Yes | No | Yes | High |
| MRA | No | Yes | Yes | Yes | No | Yes | High |
Computerized Tomographic Angiography
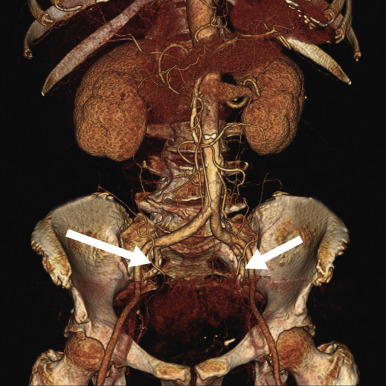
Computerized tomography angiography is considered by many plastic surgeons to represent the gold standard for preoperative imaging and was the first of the highly accurate methods of perforator assessment. Its use has been primarily directed toward abdominal flaps to identify perforator location but can also be used in the gluteal, posterior thorax, and thigh regions. The benefits of CTA include anatomic localization of the perforators, determination of the course of the perforator through the muscle, comparative assessment of the right and left vascular anatomy, and elucidation of anatomic detail of the medial and lateral row perforators ( Fig. 16.2 ). CTA will not reduce complications related to the anastomosis, flap failure, occurrence of fat necrosis, and complications relayed to dehiscence or delayed healing. CTA is especially useful in the setting of prior abdominal surgery. Paramedian abdominal incisions have been demonstrated to be the most disruptive to the perforators and the primary source vessels, whereas, laparoscopic incisions were the least disruptive.
Magnetic Resonance Angiography
Magnetic resonance angiography (MRA) represents a non-ionizing option for vascular imaging. When compared with CTA, MRA has lower spatial resolution but greater contrast resolution. This enables MRA to detect very small perforators that might otherwise be missed on CTA. As with CTA, MRA provides useful information regarding perforator location, size, and distance from the umbilicus. Its accuracy and reliability are high based on preoperative and intraoperative analysis in which all perforators visualized on MRA using a gadolinium-based contrast agent were found intraoperatively. In all patients, the location of each perforator was within 1 cm of that predicted using MRA. MRA can also successfully predict the preferred use of an SIEA flap instead of the DIEP flap based on imaging characteristics. MRA is also useful for imaging gluteal flaps and can assist with the decision to choose an IGAP or an SGAP. One study demonstrated that the superior gluteal artery was responsible for 57.5% of all gluteal perforators, the inferior gluteal artery was the source for 35% of the gluteal perforators, and the deep femoral system was the source for 7.5% of the perforators.
Duplex Ultrasound
Duplex ultrasound remains a useful tool but is less commonly utilized than either CTA or MRA. Its primary application is for abdominal flaps such as the pedicle and free TRAM, and is able to provide useful information related to the location, caliber, and flow patterns of the perforators. It is also useful to differentiate between arterial and venous flow patterns. The differentiating benefit of duplex ultrasound compared with CTA and MRA is the ability to determine flow direction and velocity. Studies evaluating perfusion of the TRAM, DIEP, and SGAP flaps, have demonstrated that the highest flow and velocity was achieved in the TRAM flap following by the DIEP and SGAP flaps. Typical flow measurements for the vessels that perfuse these flaps include the deep inferior epigastric artery (10–11 mL/min), the superior gluteal artery (9–11 mL/min), and the internal mammary artery (25–30 mL/min). The principal limitation of the color duplex is that it cannot provide 3-dimensional or architectural detail of the perforator system. Other limitations include a relatively high number of false-positive results (46%) using the handheld Doppler for localization of perforators. Comparative studies have demonstrated that CTA was superior to Doppler, based on visualization of the DIEA, its branching pattern, and the perforators.
Intraoperative Assessment and Monitoring Tools
There are a variety of methods and techniques that can be used to assess flap perfusion intraoperatively. Traditionally, surgeons have evaluated the color of the flap to determine if the perfusion is normal, congested, or pale. Surgeons have also employed the handheld acoustic Doppler and auscultated the signals of the pedicle and the cutaneous perforators ( Fig. 16.3 ). Arteriovenous bleeding from the cut edges of the flap is generally regarded a sign of adequate perfusion. Zone 4 of the abdominal free flap is often poorly perfused and cannot be reliably transferred because of the risk of fat necrosis. A fluorescent Woods lamp can demonstrate perfusion patterns within the flap. However, there has been no quantitative method to evaluate flap perfusion in the period immediately prior to or following a microvascular anastomosis.

Fluorescent Angiography
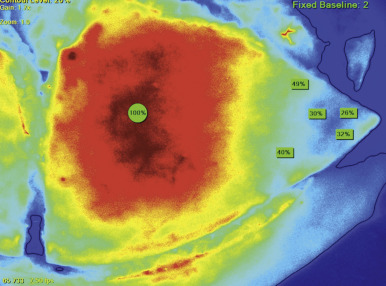
Fluorescent angiography is a relatively new technology that allows direct visualization of perfusion within a cutaneous territory. This application can be used on tissue that is elevated as a flap or on a cutaneous territory that has not been elevated ( Fig. 16.4 ). The images are captured following the intravenous injection of indocyanine green (ICG). An image-capturing laser is then positioned a few inches above the cutaneous territory to be imaged. This device is linked to a computer that analyzes the data and generates a real-time image based on the fluorescence of the ICG. Images are obtained about 15 s after the ICG injection. In the setting of flap reconstruction, the images can be captured prior to, during, and following flap elevation, as well as postoperatively.
Evaluation of the reliable vascular territory of the cutaneous portion of an abdominal flap was one of the first applications of fluorescent angiography in the setting of autologous reconstruction. It was demonstrated that classic perfusion zones described by Hartrampf were not quite accurate in that the distal segment of the flap laterally adjacent to Zone 1 was better perfused than the medially adjacent territory on the other side of the midline. Other clinical applications have included assessing perfusion in various free tissue transfer operations that include the TRAM, DIEP, SIEA, and SGAP. It was demonstrated that areas with relative hypoperfusion went on to develop areas of necrosis or eschar formation. Inflow and outflow of the microvascular anastomosis are easily visualized to confirm patency.
Fluorescent angiography is also useful in evaluating viability of the mastectomy skin flaps in the setting of immediate breast reconstruction. Fluorescent angiography is able to determine the perfusion thresholds of the skin following mastectomy and predict whether the skin will remain viable or not. Fluorescent angiography is beneficial, especially in cases of mastectomy with nipple areolar preservation. Alterations in perfusion can be noted despite what appears to be normal. In patients with a history of tobacco use or with connective disuse disorders, fluorescent angiography can help determine if further debridement is necessary.
Surgical Procedures
The abdomen is the preferred donor site for the majority of breast reconstruction procedures and is the source for the pedicle TRAM, free TRAM, DIEP, and SIEA flaps. Inherent to understanding these flaps is an appreciation for the various types of muscle preservation techniques. Classification of muscle sparing is based on the amount of rectus abdominis preserved ( Table 16.2 ). Most muscle-sparing operations will require free tissue transfer. The next section focuses on the various flaps based on body region of harvest.
| Muscle sparing technique | Definition (rectus abdominis) |
|---|---|
| MS-0 | Full width, partial length |
| MS-1 | Preservation of lateral segment |
| MS-2 | Preservation of lateral and medial segment |
| MS-3 (DIEP) | Preservation of entire muscle |
Abdomen
DIEP Flap (see Ch. 57 )
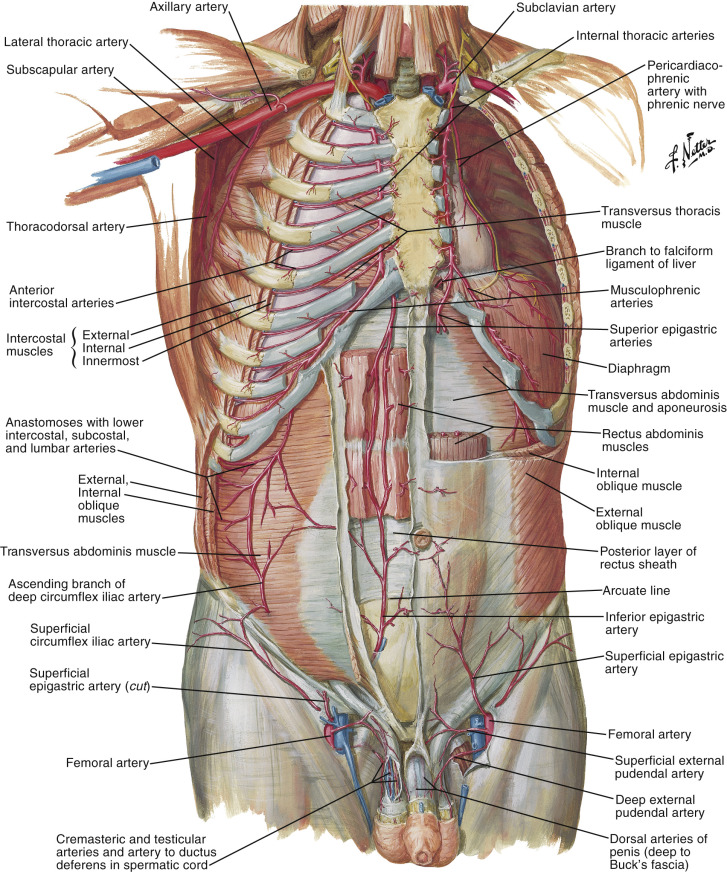
The deep inferior epigastric perforator (DIEP) flap has become the most commonly utilized option for autologous breast reconstruction. The blood supply to the anterior abdominal wall is derived from the superior and inferior epigastric vascular systems ( Fig. 16.5 ). The inferior system is composed of the deep inferior epigastric artery and vein as well as the superficial inferior epigastric artery and vein. The deep system is usually the dominant and is therefore preferred in the majority of cases. The superficial system is less predictable, often not present, and therefore less commonly used; however, in some cases (<5%) the superficial system provides the dominant venous drainage to the adipocutaneous component of the anterior abdominal wall. This fact may explain the problem of venous congestion that is observed in some DIEP flaps, despite a patent venous anastomosis.
An understanding of the perforating system and primary source vessels for abdominally based flaps is critical when considering their use. The “Gent” consensus described the five most common perforator types based on location, branching patterns, and diameter. In general, for a DIEP flap to be successfully harvested and transferred, a single perforating artery and vein of at least 1.5 mm in diameter is recommended. If a dominant perforator arising from the deep system is not identified, it may be because the superficial inferior epigastric system is the more dominant.
Successful harvest of a DIEP flap requires precise perforator identification, dissection, and preservation. Specific techniques will vary from surgeon to surgeon but in general, are based on similar principles and concepts. Only a few surgical instruments are necessary that include a fine tip mosquito clamp, Weitlaner retractors, fine scissors, tissue forceps, and a low set mono- or bipolar electrocautery unit. The selected perforator should be ideally located near the center of the flap in order to obtain equidistant perfusion. A minimal perforator diameter of 1.5 mm is usually recommended. When several perforators are available, sequential occlusion can be performed to assist with the selection process ( Fig. 16.6 ). Multiple perforators can be considered when they are aligned in series or in close proximity. Medial row perforators are preferred when the reconstruction requires the inclusion of Zones 3 and 4 on the opposite side of the midline. Perforators in the lateral row are usually more closely intertwined with the intercostal motor nerves of the rectus abdominis muscle, and excessive dissection in that area may predispose to nerve injury and motor weakness.
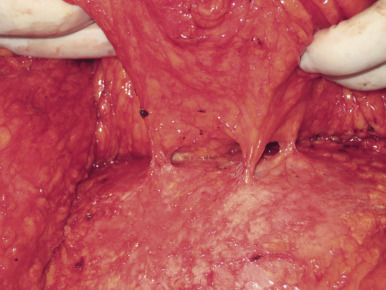
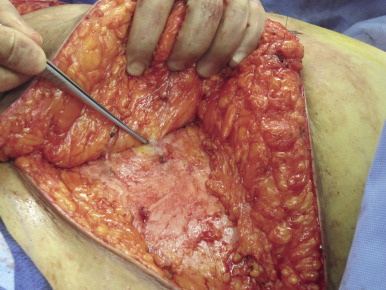
When initiating the perforator dissection, the location of the tendinous inscriptions is important. Sometimes the perforator penetrates this region of the anterior rectus sheath and, in those cases, including a small cuff of the anterior rectus sheath (1–2 mm) around the perforator is recommended ( Fig. 16.7 ). During the dissection it is imperative to preserve the lateral intercostal nerves as they pierce the rectus abdominis muscle at the junction of the lateral and central longitudinal segments. Failure to do so will likely result in abdominal weakness or bulge. Motor nerve branches that cross the perforator or the source vessel should be sharply divided in order to elevate the flap. Whether or not to coapt the severed nerve is controversial. Some advocate using a microsuture for coaptation, whereas others prefer to allow the cut end of the motor nerve to neurotize into the adjacent medial segment of the rectus abdominis muscle. The intramuscular dissection proceeds to the point that the perforator or inferior epigastric vessel becomes submuscular ( Fig. 16.8 ). At that point, the dissection continues within the retromuscular plane and progresses from the lateral edge of the muscle toward the iliac vessels. Some surgeons prefer to dissect the source vessel to its origin in order to optimize the length and the caliber of the vascular pedicle ( Fig. 16.9 ). Some surgeons prefer to dissect the pedicle to the length and caliber that is necessary in order to perform a successful anastomosis. This technique may minimize trauma to the rectus abdominis muscle and improve function. Dissection of multiple perforators can potentially compromise function of the rectus abdominis muscle if the myotomies are several in number as well as diagonal or transverse in orientation.
Throughout the dissection of a DIEP flap, it is recommended to assess the perfusion from the peripheral edges of the flap. This is often achieved by direct visualization for arterial and venous bleeding as well as by using a handheld Doppler probe to listen for the arterial and venous signals. Fluorescent angiography using indocyanine green can also be considered because it can identify cutaneous perforator location and determine the limits of perfusion within the adipocutaneous territory of the flap. When several perforators are isolated but only one or two are needed, the extra perforators are preserved until the pedicle is completely isolated. The extra perforators can be used in the event that a selected perforator is injured during the dissection. When in doubt about the quality of the perforators, a muscle-sparing free TRAM flap can be considered. Figure 16.10 illustrates a patient following bilateral DIEP flap reconstruction.
The primary recipient vessels for the DIEP and all free flaps used for breast reconstruction include the internal mammary artery and vein and the thoracodorsal artery and vein ( Fig. 16.5 ). The internal mammary vessels are preferred by most surgeons because they are relatively easy to expose, provide excellent flow characteristics, and are usually of a more favorable caliber. The internal mammary vessels are usually used for the most immediate and delayed reconstructive procedures. The vessels are exposed at either the third or fourth interspace by excising the cartilaginous segment. At this level the diameter of the internal mammary vein is usually 2.5–3.5 mm and the internal mammary artery is 2.5–3 mm. The thoracodorsal artery and vein can also be considered; however, given the prevalence of sentinel lymph node biopsy and the rarity of axillary dissection, these vessels are used less often. However, in the setting of a modified radical mastectomy where the thoracodorsal vessels have been exposed, they are routinely preferred.
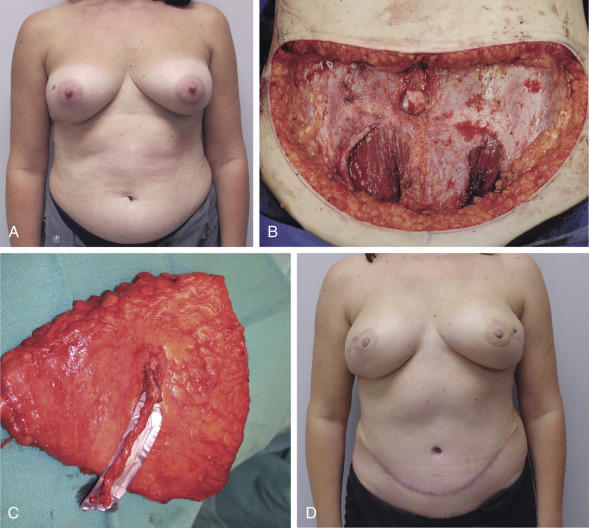
Free TRAM Flap (see Ch. 37 )
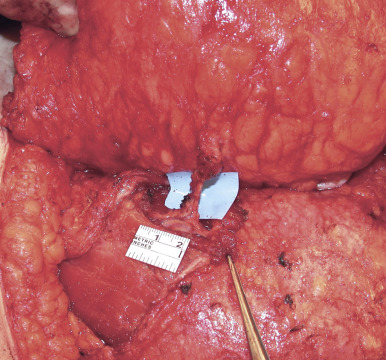
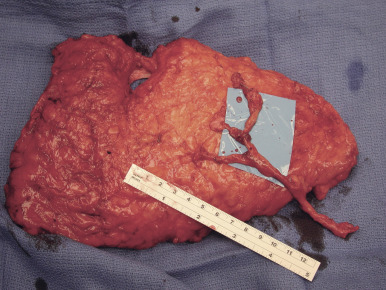
The decision regarding whether to perform an MS-2 free transverse rectus abdominis musculocutaneous (TRAM) flap or DIEP flap is ultimately based on the presence and quality of the abdominal wall perforating vessels. Knowledge of these perforators can be assessed either pre- or intraoperatively as previously described. When a suitable perforator from the deep inferior vascular system is not visualized, one can consider performing an SIEA flap or a muscle-sparing free TRAM. The MS-2 muscle-sparing free TRAM is the author’s preferred flap in this situation. With this flap, a small central segment of the rectus abdominis muscle and anterior rectus sheath (2–4 cm) is harvested incorporating several small (<1.5 mm) vessels ( Fig. 16.11 ). An algorithm for the selection of a DIEP or muscle-sparing free TRAM is depicted ( Table 16.3 ). Figure 16.12 demonstrates a woman following a left breast reconstruction with a muscle sparing (MS-2) free TRAM flap.










