Breast Augmentation With Round and Anatomic Implants
Bill Kortesis
Charalambos “Babis” Rammos
DEFINITION
Round implants are most commonly used in the United States.
They are symmetrical in height and width and have varying projections for a given volume, typically designated as low, moderate, high profile, and extra high.
The more the projection increases for a fixed volume, the more the width of the device decreases (FIG 1A).
Round implants may be smooth or textured and may be filled with either saline or silicone gel.
Fourth and fifth generation round silicone devices, currently used in the market, are designed with thinner shells and a more cohesive gel.
Anatomic (shaped) implants have become an important alternative for breast augmentation.
Shaped implants are textured to reduce movement and can have differences in height, projection, and width.
They have greater projection in the caudal portion and less projection in the cephalic portion (FIG 1B), mimicking the natural shape of the breast.
The more cohesive and dense silicone gel (fifth generation) allows the implant to maintain its shape, and resist the natural forces exerted by the soft tissue envelope.
Orientation markings on the device position it properly in the breast pocket.
ANATOMY
The breast extends from the 2nd or 3rd rib down to the 6th or 7th rib (cephalad to caudad) and from the lateral sternum to the anterior axillary line (medial to lateral).
The major blood supply to the breast is from the internal mammary artery.
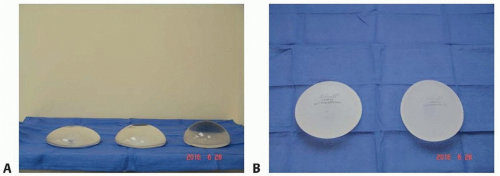
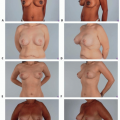
FIG 1 • A. Lateral view of a moderate projection (left), full projection (center), and extra full projection (right) 400 mL smooth round silicone gel implant. As the projection increases, the height and the width of the device decrease. B. Moderate height, full projection (left) and full height, full projection (right) anatomic 420-mL gel implants as seen from above.
Lateral and anterior branches of the second through sixth intercostal nerves provide innervation to the skin overlying the breast.
PATHOGENESIS
Micromastia occurs as a developmental phenomenon either as primary mammary hypoplasia or due to chest wall pathology such as Poland syndrome.
It may also present as an involutional process, due to weight loss or after pregnancy and lactation.
Micromastia may lead to a negative body image and have a deleterious effect on quality of life.
According to the American Society for Aesthetic Plastic Surgery (ASAPS) 2015 statistics, breast augmentation was the second most common aesthetic surgical procedure performed, with approximately 306 000 cases.1
PATIENT HISTORY AND PHYSICAL FINDINGS
Goals and expectations of the patient are discussed in detail during consultation.
A thorough personal and family history is performed.
History of any breast disease and breast cancer
History of pregnancy
Desire for future pregnancy
Mammogram: Screening mammogram is obtained for any patient over 35 years of age.
Physical examination
Current height and weight
Current breast size and desired breast size
Palpation for any breast masses, lymph nodes, or nipple discharge
Observation of breast ptosis and degree of ptosis, and the need for synchronous mastopexy
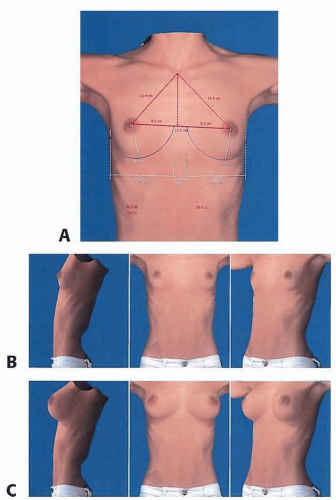
FIG 2 • Three-dimensional photograph of a 24-year-old female using the VECTRA 3D imaging device. A. Breast measurements. B. Preoperative frontal, lateral, and oblique views. C. Simulated images obtained using a 320-mL shaped implant.
Observation of chest wall and breast asymmetries, such as differences in inframammary fold height, nipple-areolar complex height, breast volume, and breast shape
IMAGING
The authors use the VECTRA 3D imaging and simulation system for all patients interested in breast augmentation. The device takes a 3D photograph that can then be visualized in the monitor, with the addition of breast measurements (FIG 2A,B).
Using different implant shapes and sizes, a simulated postsurgical result is produced, allowing the patients to have a visual image of the outcome (FIG 2C).
The use of the VECTRA 3D imaging system provides a high degree of accuracy for breast volume (90%) and contour (98.4%).2
SURGICAL MANAGEMENT
Main objectives of breast augmentation:
Enhancement of breast shape and volume
Main indications for use of a round implant:
Desire for a fuller look
Good skin quality and overall breast anatomy
Concerns about device rotation
Main indications for use of an anatomic implant:
Thin patients with little breast volume. In this patient population, the final shape of the breast will be determined by the device itself.
Patients with deficiency at the inferior pole
Patients with chest height-width disproportions, such as patients who have a very long, but not very wide chest, or have a very wide, but not very long chest.
Patients with breast asymmetries. By using a variety of heights, widths, and projections, these asymmetries may be overcome.
Patients who do not want a full round upper pole appearance.
Main factors to consider when using shaped implants rather than round implants:
Incision length needs to be slightly longer because of the filling material traits.
Orientation: Precise placement of the implant is critical as disorientation will lead to distortion of the breast shape.
Implant height needs to be chosen wisely to avoid overfilling or underfilling of the upper pole of the breast.
Lowering the inframammary fold is important.
For either type of implant, the main steps of the procedure are the same:
Make the incision and aim cephalad with attention not to violate Scarpa fascia.
Create a dual plane.
Identify the pectoralis major muscle edge and incise.
Create a subpectoral pocket with care not to elevate the pectoralis minor muscle.
Place tester implants (sizers).
Exchange tester implants for the formal implants.
Close the wound in layers.
Preoperative Planning
At the time of consultation
Breast measurements
Breast width at its widest point.
Nipple to inframammary fold (N-IMF) distance.
Sternal notch to nipple distance.
Breast height.
Assessment of breast parenchyma and skin
Elasticity: This is performed with deflection of the skin, and observation for resistance.
Pinch test: This is performed at the superior and medial portion of the breast, between the examiner’s thumb and index finger. A result of less than 2 cm is usually an indication for placement of the implant in the subpectoral plane.
Choice of implant volume. Sizers are placed in a bra and compared to the images obtained by the 3D imaging.
Table 1 Calculations for Lowering the Inframammary Fold for Anatomic Implants
Breast Implant Width
Nipple to Fold Distancea
11.0 cm
7.0 ± 0.5 cm
11.5 cm
7.5 ± 0.5 cm
12.0 cm
8.0 ± 0.5 cm
12.5 cm
8.5 ± 0.5 cm
10.0 cm
9.0 ± 0.5 cm
13.5 cm
9.5 ± 0.5 cm
14.0 cm
10.0 cmb
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree