Breast Augmentation: Subglandular, Subfascial, and Submuscular Implant Placement
Chet Mays
Bradley Calobrace
DEFINITION
A critical choice in breast augmentation is where to place the implant pocket.
Subglandular
Subfascial
Submuscular (for purposes of this paper, submuscular refers to below the pectoralis major)
Implant choice, size, and location are based on a variety of patient qualities.
A biodimensional analysis is essential in determining the optimal implant type, size, and pocket location. There are many methods of evaluation. The High Five system described by Tebbetts is a systematic approach that illustrates the most important aspects of evaluation, including the following:24
Base width of breast
Base width of implant
Nipple to fold distance
Estimate of final implant volume
Pocket determination based on skin pinch thickness
Subglandular Implant
The subglandular implant is deep to the breast tissue and superficial fascia, but superficial to the deep pectoralis fascia, coming to rest on the inframammary fold (FIG 1).
The subglandular pocket has long been regarded as the most natural pocket.2
The advantages of subglandular implant placement include the following:
It avoids implant deformation or distortion that can be seen in the subpectoral position
Enhances the improvement in the constricted or ptotic breast
Allows an easier dissection plane
Decreased postoperative discomfort
Allows access to the inframammary fold (IMF) as the superficial and deep fascial components merge
There are some disadvantages of the subglandular pocket, which include the following:
Pocket with the least soft tissue coverage to disguise the implant
Increased visibility or palpability of implant with wrinkling or rippling
Higher capsular contracture rate
Less support and stabilization of the implants, especially shaped devices, compared to subfascial or submuscular pockets
Subfascial Implant
It avoids implant deformation or distortion (animation deformity) that can be seen in the subpectoral position.
This position provides additional soft tissue coverage between the implant and the skin as compared to the subglandular pocket.
Fascia provides additional support to minimize implant edge visibility and palpability seen most commonly with subglandular placement.
Fascia provides support of implant especially in the upper pole minimizing excess implant movement and potential rotation with shaped implants.
Less postoperative pain as compared to submuscular placement
Fascia provides a distinct layer separating the implant from the overlying breast parenchyma.
The disadvantages of a subfascial pocket include the following:
Less soft tissue coverage compared to submuscular coverage
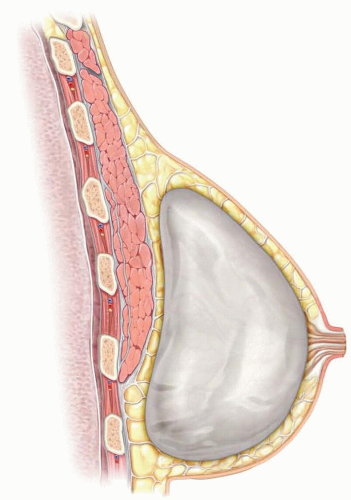
FIG 1 • Subglandular implant placement is deep to the breast tissue but superficial to the pectoralis fascia.
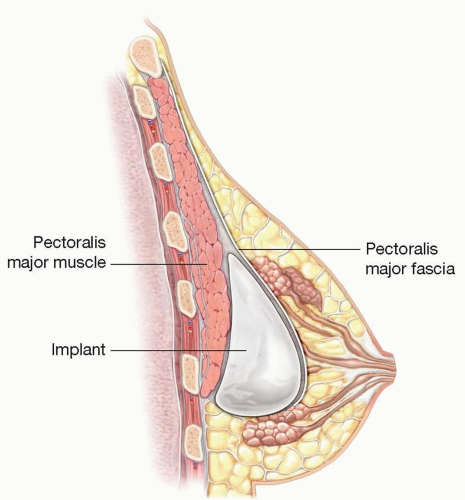
FIG 2 • Subfascial implant placement is deep to the breast tissue and the pectoralis major fascia but superficial to the muscle.
More challenging dissection to separate deep pectoral fascia from underlying muscle while keeping fascia intact.
Higher rate of capsular contracture compared to submuscular
Submuscular Implant
Advantages to placing the implant in a submuscular pocket (FIG 3) as compared to placement in the subglandular or subfascial pocket include the following:
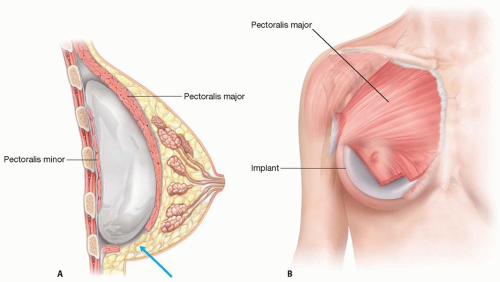
FIG 3 • A. Submuscular position of the implant with overlying pectoralis muscle and breast parenchyma. Note that the released inferior edge of the pectoralis major allows lower pole expansion (arrow). B. Anterior view of the implant placement below the pectoralis major.
Enhanced coverage of the implant
Reduced issues with wrinkling
Sloping natural upper pole
Enhanced support for the breast implant
The disadvantages of a submuscular pocket include the following:
Animation deformity
Increased risk of implant superior malposition with waterfall deformity
Increased postoperative pain
Limited expansion of the lower pole of breast (required to expand constricted and ptotic breasts)
The most significant attribute of the submuscular pocket is in providing maximum soft tissue coverage for the implant. The widespread use of saline implants and wrinkling issues led to surgeons looking for improved implant coverage. After the moratorium on silicone was lifted, surgeons in the United States continued to use the submuscular pocket with mostly smooth and to a limited extent textured silicone implants.6
ANATOMY
An understanding of the breast blood and nerve supply is critical when performing breast surgery (FIG 4AB).
Muscular attachments are shown in FIG 4C.
The breast is a skin appendage contained within layers of the superficial fascia.
The superficial layer of this fascia is near the dermis and is not distinct from it.
The deep layer of the superficial fascia is more distinct and is identifiable on the deep surface of the breast when the breast is elevated in a subglandular augmentation mammoplasty.
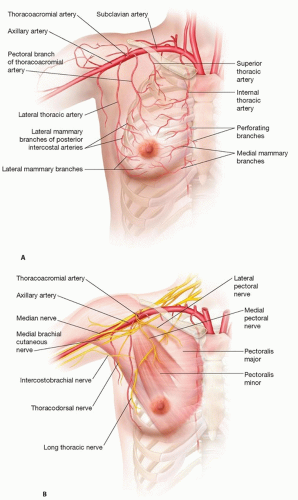
FIG 4 • A. Arterial blood supply of the breast. B. Nerve branches supplying the breast.
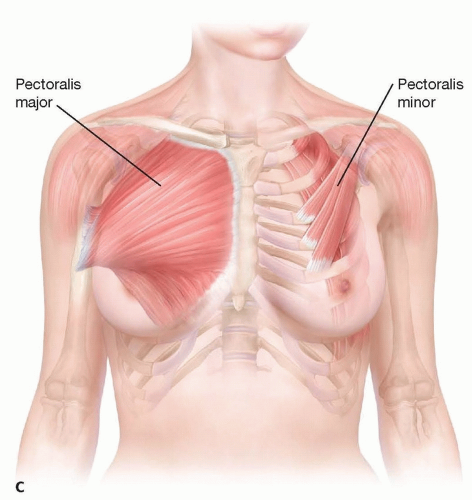
FIG 4 (Continued) • C. Muscular attachments to the chest. The pectoralis major is removed on the right side of the picture revealing the underlying pectoralis minor.
There is loose areolar tissue between the deep layer of the superficial fascia and the fascia to cover the pectoralis major that and to cover the adjacent rectus abdominis, serratus anterior, and external oblique muscles.
The deep pectoralis fascia has its origin on the clavicle and sternum, extending toward the lateral border of the muscle to form the axillary fascia (FIG 5).
It continues down to cover the latissimus dorsi muscle, rectus abdominis, serratus anterior, and external oblique.
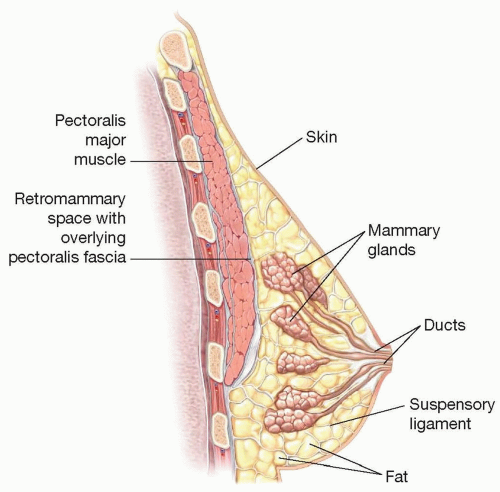
FIG 5 • Breast anatomy showing pectoralis fascia posterior to the breast tissue.
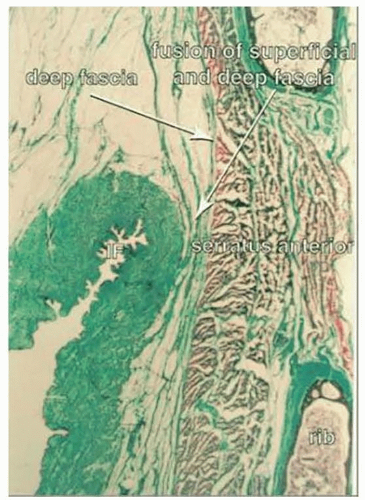
FIG 6 • Histologic slide of the inframammary fold (IMF) showing the superficial and deep fascia fusing together.7
The subfascial pocket is deep to this deep pectoral fascia but superficial to the underlying muscle.
This fascia is thin and more fragile in the lower two-thirds of the pectoralis muscle and becomes denser and substantial in the upper third of the muscle.
The thin fascia in the lower aspects of the breast can make the initial subfascial dissection more challenging, which becomes easier as the dissection proceeds toward the upper pectoralis muscle.
PATIENT HISTORY AND PHYSICAL FINDINGS
Initial consultation should evaluate the patient’s goals and anticipated results with the breast augmentation.
A thorough history and physical should be done to identify any risk factors for the procedure, including bleeding or clotting disorders.
Any history of breast lumps, masses, or breast disease should be elicited.
A family history is required.
In planning for optimal implant pocket selection, it is important to determine the desired appearance or “look” the patient is seeking.
The submuscular pocket is more likely to create a smooth, sloping upper pole with minimal roundedness in the upper pole.
A patient desiring a more rounded upper pole with a more obvious “implant appearance” with implant shape visibility may prefer a subglandular implant, provided there is adequate soft tissue coverage.
The subfascial approach can provide a compromise between the two; the implant will be in a plane similar to the subglandular, but the additional fascia layer will minimize implant edge visibility and palpability that can be seen with the subglandular pocket.
The preoperative exam of the breast augmentation patient will guide the surgeon’s implant selection and pocket placement. The physical exam measurements should include the following (FIG 7):

FIG 7 • Necessary physical exam breast measurements.
Breast width (BW)
Sternal notch to nipple (SSN:N)
Breast height (BH)
Nipple to IMF (N:IMF) at rest and under maximal stretch.
Upper pole pinch (UPP), medial pinch (MP), and lateral pinch (LP)
Intermammary distance (IMD)
Pinch Test
A key point of the exam is the upper pole pinch test.
A pinch test of less than 2 cm indicates the need for a submuscular placement of the implant to avoid noticeable rippling (FIG 8A).
If the pinch test is more than 2 cm (1 cm of soft tissue thickness), the patient is a candidate for a subglandular or subfascial pocket (FIG 8B). (The deep fascial layer will provide additional coverage over the implant to allow for subfascial placement.)
Implant selection impacts adequacy of soft tissue coverage. Keep in mind the thinner the soft tissue, the greater the risk of implant palpation and rippling.
Some implants are prone to more wrinkling, including underfilled saline implants and textured devices.
We require a pinch test of more than 2 cm if placing the implant subfascially or subglandularly, where the soft tissue coverage is firm and good quality.
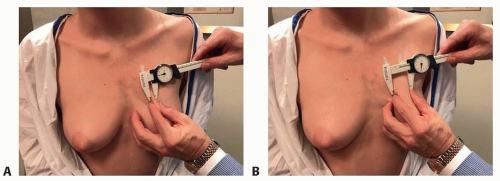
FIG 8 • A. Upper pole pinch test less than 2 cm and (B) more than 2 cm.
If the soft tissue coverage is lax and poor quality or if the implant selected is deemed at risk for wrinkling, a pinch test greater than 3 cm is more reliable in providing adequate coverage and minimizing the risk of rippling.
Adequate soft tissue coverage in the upper pole in a subglandular augmentation will camouflage the transition between the breast and implant, aiding to a smooth natural upper pole.
The deep fascia overlying the implant in the subfascial pocket will provide additional support and coverage in the upper pole and minimize the implant edge visibility, which can be seen if implants are placed in the subglandular pocket with limited upper pole coverage.
If the patient prefers a full, rounded upper pole with an obvious transition between her implant and soft tissue, a subglandular implant would be preferred even if the pinch test is less than 2 cm.
One must have a discussion regarding visible and palpable rippling of the implant if placing the implant subglandular and the pinch test is less than 2 cm.
Capsular contracture can be reduced by using a textured implant in the subglandular position, but one must consider the risks of rippling with textured implant in a patient with inadequate upper pole coverage with a pinch test of less than 2 cm.1
Physical Assessment
Assess for all asymmetries, including breast volume, IMF, nipple-areolar complex (NAC), and chest wall.
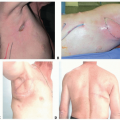
Chest wall (skeletal and muscle) abnormalities or asymmetries are often underappreciated and can significantly alter the final result (FIG 9).8
Pectus excavatum occurs occasionally, whereas pectus carinatum and Poland syndrome are rare.9
Central deformities are typically ameliorated sufficiently by breast augmentation alone.
Deep pectus excavatum deformities can be treated simultaneously with a custom solid silicone implant made from a plaster mold, although most patients decline this option.
Poland syndrome (absence of sternal head of pectoralis muscle) is best addressed with subglandular augmentation as the sternal head of the pectoralis major muscle is absent. When more severe, more extensive adjunctive procedures, such as tissue expansion, fat grafting, and latissimus muscle transfer, may be required.10
Hemithorax asymmetry due to differences in shape, protrusion, or regression can create an uneven breast foundation, suggesting different size implants despite equivalent breast volumes.
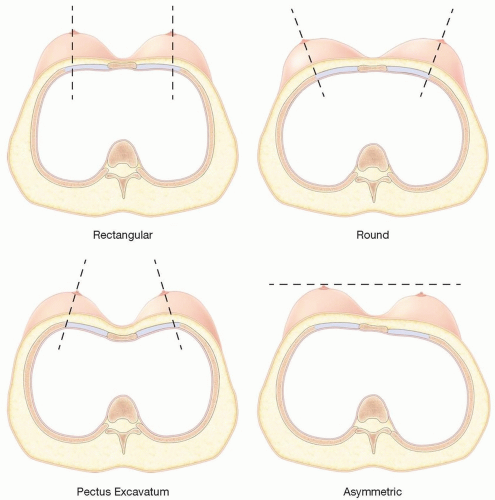
FIG 9 • Examples of chest wall abnormalities.
Unilateral prominence of the chest wall is often associated with scoliosis (FIG 10).
Subtle unilateral pectoralis hypertrophy should not affect subglandular or subfascial implant placement, but it could affect subpectoral placement and overall implant projection.
IMAGING
Screening mammography per the American College of Surgeons is recommended for patients over 40 years of age.
Many plastic surgeons recommend a baseline mammogram at 35 or older prior to a breast augmentation, especially if a family history is present.
Any additional diagnostic studies are guided by the preoperative exam.

FIG 10 • Left chest wall prominence compared to the right chest wall.
Any palpable mass requires evaluation, usually with a diagnostic ultrasound and/or mammogram.
SURGICAL MANAGEMENT
The preoperative evaluation and decision-making are a critical step in achieving optimal outcomes in breast augmentation.
Capsular contracture is the leading indication for revision breast surgery after a breast augmentation and every effort should be made during planning and execution to minimize the risk of capsular contracture postoperatively. Placement of breast implants in the submuscular pocket has consistently demonstrated reduction in capsular contracture rates compared with the other pocket choices.1,4
Validated steps to reduce this risk include the following:
Preoperative Planning
Incision
The decision on incision placement is based on a variety of variables:
Patient and surgeon preferences
Anatomic considerations
Implant type and size
Issues of capsular contracture, breast-feeding, and NAC sensation
There are many potential advantages of the inframammary approach, including the following:
Well-hidden scar in the fold of the breast
Incisional length is unlimited, thus can accommodate any and all implant choices
Excellent visualization for dissection of the implant pocket
The ability to control the IMF position during incision closure
Can be used for any complication revision
Lower capsular contracture
Minimal issue of a scar contracture creating deformity
Potentially less nipple sensation changes
Potential disadvantages of the inframammary incision include the following:
The scar is located on the breast
Scar may be more visible if breast fold is absent or if the scar becomes pigmented
Must determine final IMF position preaugmentation and place scar precisely in planned new fold.
Scar position more vulnerable to irritation from the bra
There are many potential advantages of the periareolar approach, including the following:
Scar can be camouflaged in the areolar border
Direct visualization and access into the breast pocket
Can lower the IMF to any location without predetermining location
Central access allows use in most revision cases with optimal visualization and access to the upper pole of the breast
Access for parenchymal breast scoring in constricted breast deformities
Potential disadvantages of the periareolar incision include the following:
The scar is located on the breast
Access is through a tunnel and may limit visualization in dense, heavy breasts
Cannot use if areolae are too small
Poor scarring possible and can create significant deformities
IMF control sutures not possible when IMF is lowered
Transection of breast ducts may increase bacterial contamination
Potentially higher capsular contracture rates15
Good candidates for the inframammary approach may include the following:
Small areola
When controlling IMF is desired
Indistinct areolar border
Desire for no scar on the breast
Potentially when placing larger implants
Desire future breast feeding as interference with lactation has been implicated with periareolar incision.5
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree