Introduction
One-stage breast augmentation combined with mastopexy is a challenging operation with numerous potential complications. Augmentation expands the breast volume, and mastopexy reduces the skin envelope; thus, these operations produce opposing forces when performed simultaneously. The combination of procedures as a single stage was initially described over 50 years ago. , However, augmentation mastopexy has been met with stark criticism in the literature by prominent plastic surgeons until as recently as the past decade with warnings such as “surgeon, beware” , when performed primarily and a “recipe for disaster” when mastopexy is performed secondarily in previously augmented patients.
Over the past decade, safe performance of augmentation mastopexy as a one-stage operation has greatly increased after landmark articles by the senior author showing acceptable complication and revision rates. In recent years, the safety of primary augmentation mastopexy has been further validated by several authors. Secondary augmentation mastopexy in the previously augmented patient also can be performed successfully. , The terms secondary and revisional augmentation mastopexy lack standard definitions in the literature. We define secondary to mean simultaneous augmentation mastopexy performed on a breast that previously underwent any type of surgery. We define revisional as a subcategory of secondary augmentation mastopexy that refers to immediate surgical correction of a problem or late surgery to improve the results of a previous augmentation mastopexy.
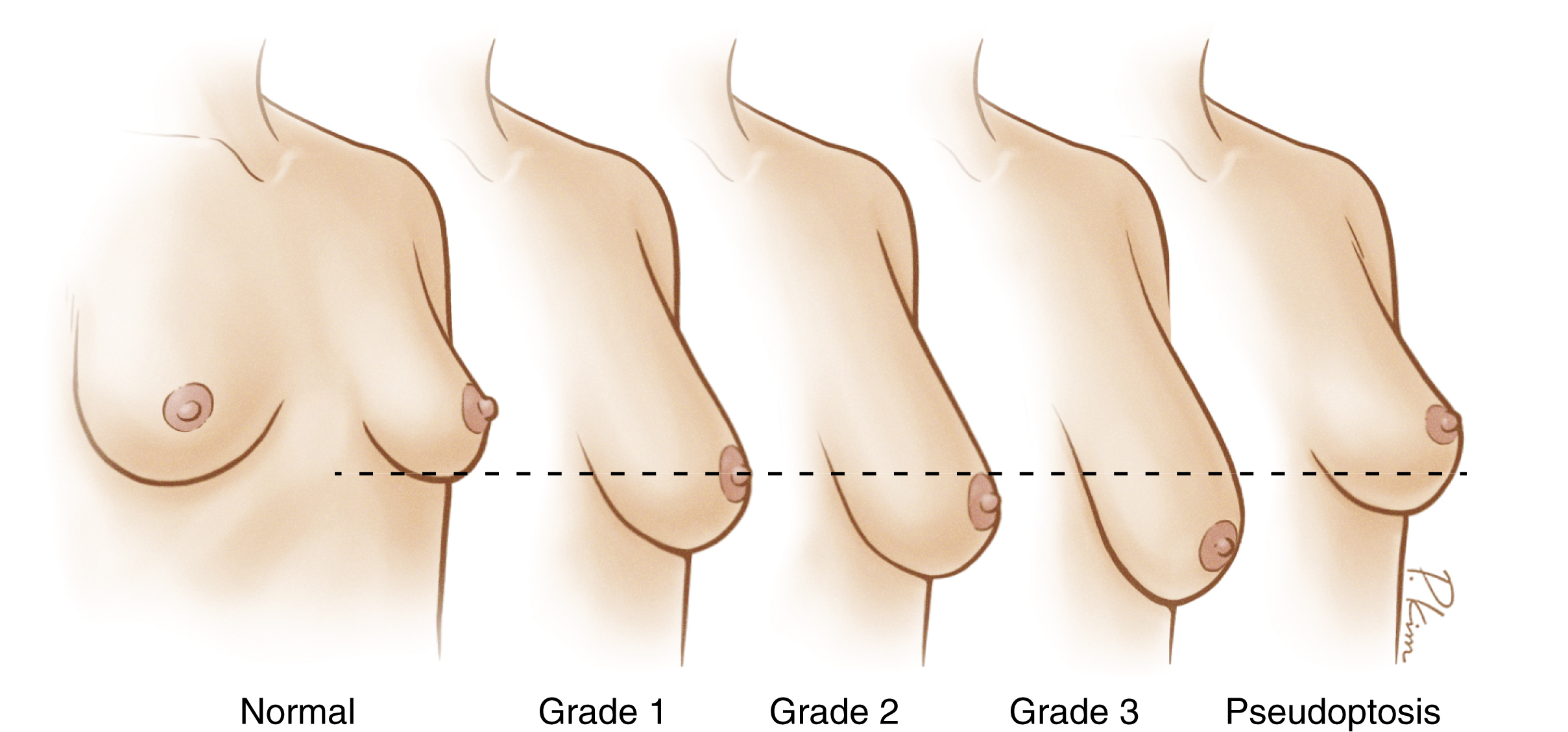
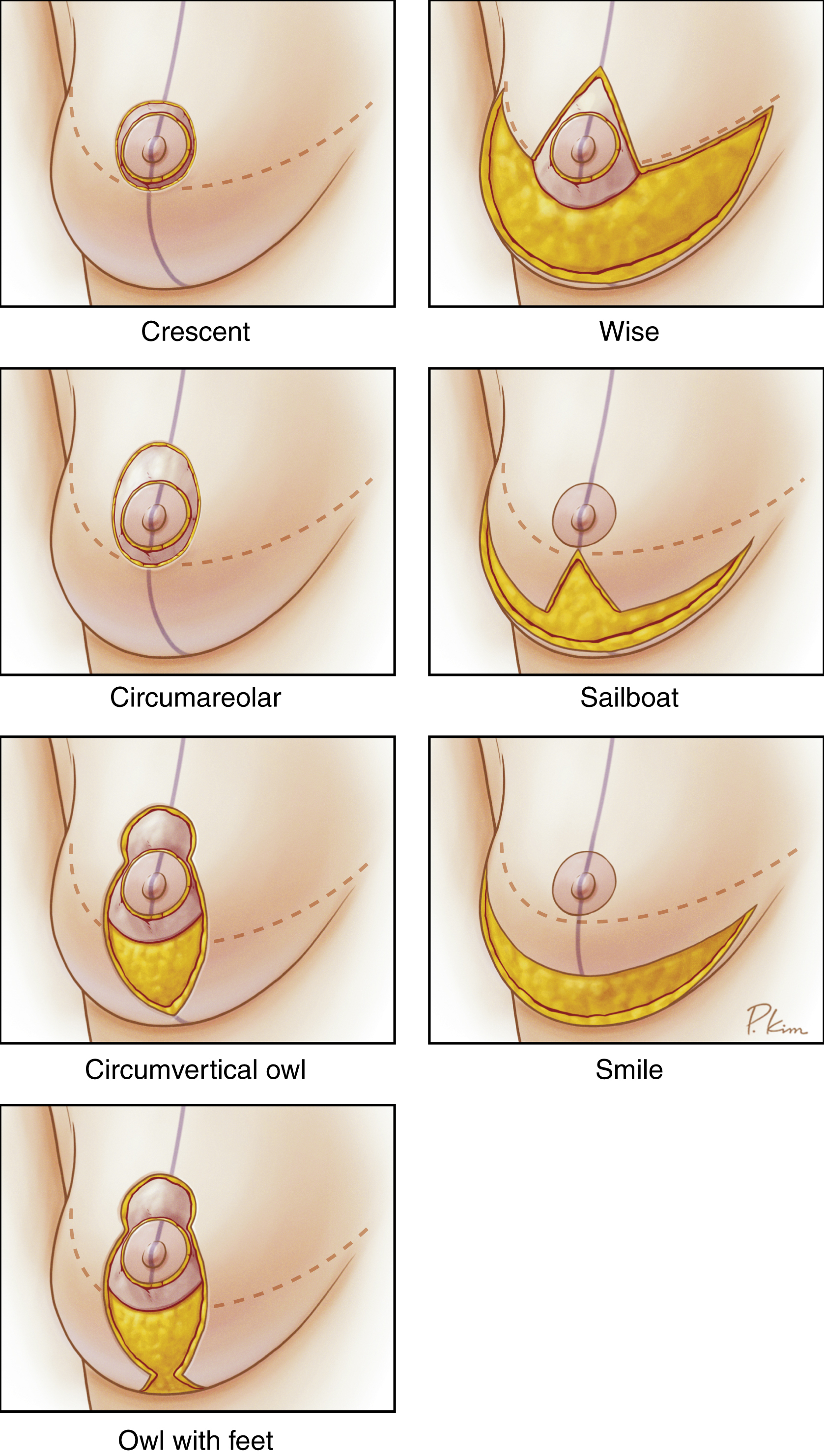
Throughout this chapter, ptosis grades are described according to the Regnault classification ( Fig. 16.1 ). Depending on the degree of ptosis, a mastopexy can be performed by a crescent, circumareolar, circumvertical, or Wise pattern or other approach ( Fig. 16.2 ). Each approach has its own utility in both primary and secondary augmentation mastopexy based on each patient’s individual anatomy. The focus of this chapter will be on the circumvertical (often simply referred to as vertical ) technique for primary augmentation mastopexy.
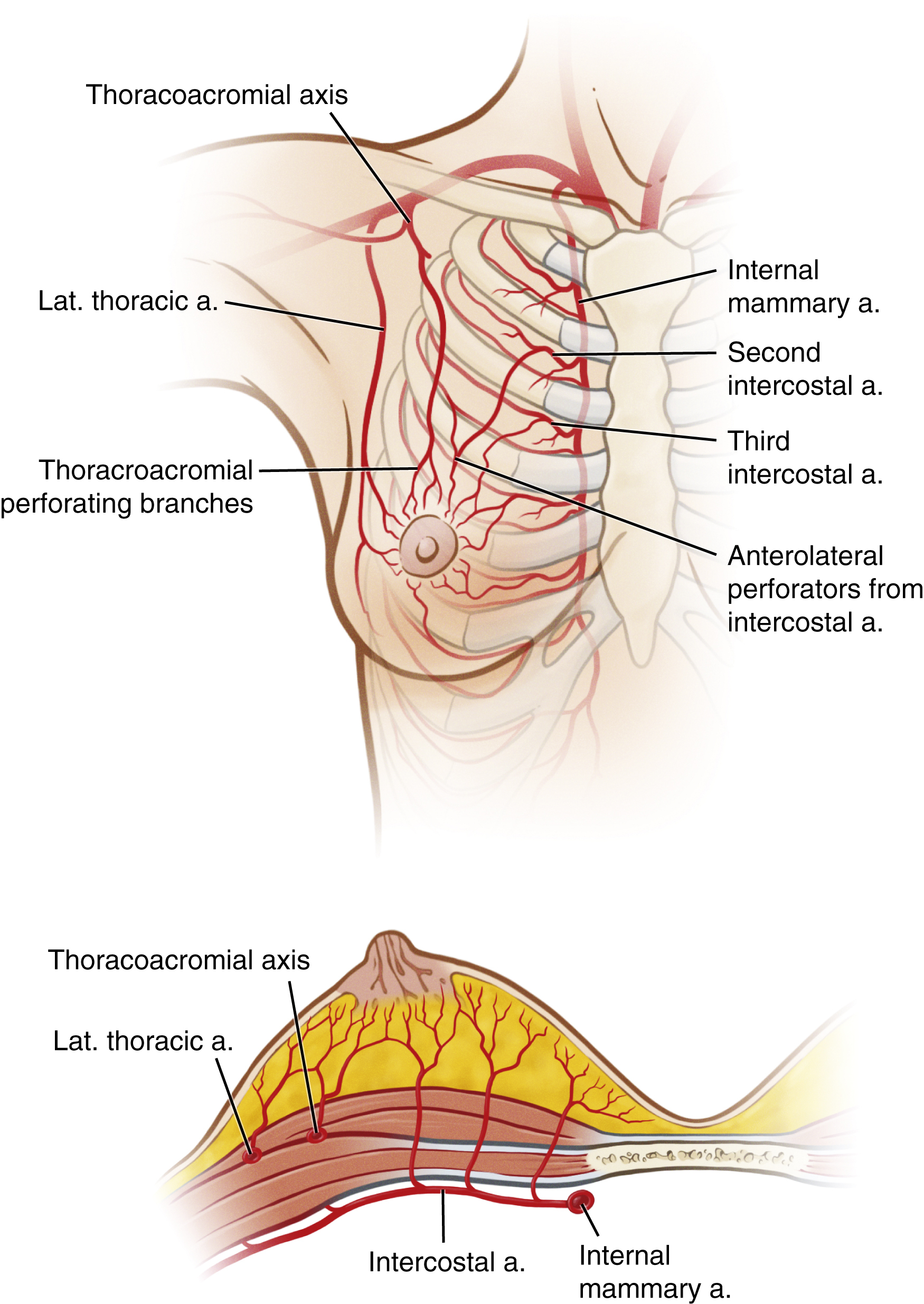
The circumvertical approach is designed as a superior pedicle based on perforators from the second and/or third intercostal vessels ( Fig. 16.3 ). The circumvertical technique often requires a short horizontal wedge of skin in the inframammary fold (IMF) to shorten the nipple-to-IMF distance, thus creating an inverted-T incision pattern at the time of closure. For simplicity, we describe these two approaches as an “owl” and “owl with feet” design, respectively, because of their rudimentary resemblance to the bird. The “body” of the owl refers to the circumvertical pattern, and the “feet” refer to the short horizontal limb at the inferior extent of the circumvertical pattern near the IMF. Unlike a Wise pattern mastopexy, in which the vertical limbs become progressively further apart as they approach the IMF, the vertical limbs taper together with the “owl” techniques as they approach the IMF. Guidelines regarding patient selection for each of these augmentation mastopexy techniques and technical aspects of the procedure are outlined in this chapter.
Indications and Contraindications
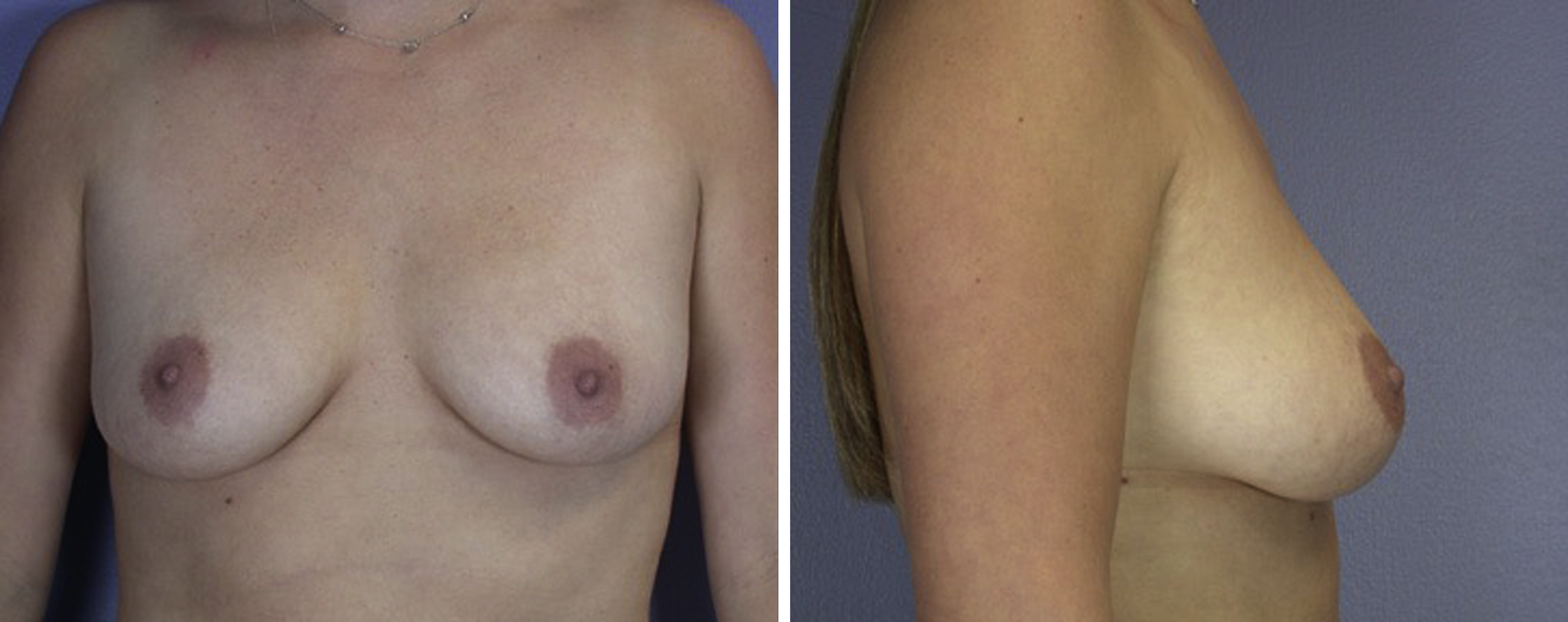
Patients with breast hypoplasia and ptosis are considered candidates for augmentation mastopexy ( Fig. 16.4 ). Patients with Regnault grade I ptosis who require only 1–2 cm of elevation of the nipple–areolar complex (NAC) with minimal laxity of the lower pole of the breast may be candidates for a crescent or circumareolar mastopexy. Patients with Regnault grade II or III ptosis who require more than 2 cm of NAC elevation or patients with grade I ptosis or pseudoptosis with substantial laxity in the lower pole are better treated with a circumvertical pattern. Therefore, the nipple position and grade of ptosis alone do not determine the best mastopexy technique to apply; the amount of lower pole laxity is the most important consideration as to whether a vertical mastopexy pattern would be best.

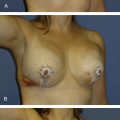
In patients presenting for breast augmentation, there is a common misperception that insertion of larger implants in a patient with mild ptosis or pseudoptosis will suffice as an alternative to the additional scars of a mastopexy, but that is incorrect ( Fig. 16.5 ). Patients undergoing breast augmentation may elect that option to avoid scars and be satisfied accepting some persistent lower pole laxity with greater upper pole fullness; however, the lower pole laxity cannot be corrected with a larger implant alone, and the patient will potentially be subjected to the detrimental effects of an implant that is too large for her breast. In patients desiring a more lifted breast, the addition of an implant can help create a larger, rounded breast shape with greater upper pole fullness via an augmentation mastopexy.
Patients with a tuberous breast often benefit from an implant plus circumareolar mastopexy because of the characteristic anatomic features of their breasts (e.g., amorphous breast shape, constricted lower pole, superiorly positioned IMF, large herniating areola). A circumvertical approach is usually not advisable in the tuberous breast because the lower pole is already overly tight and the low-appearing NAC position is relative to an IMF that is anatomically too high. In such tuberous breast cases, lowering the IMF with an implant will correct the position of the NAC relative to the fold, and a circumareolar mastopexy can be used to reduce the large areola size and flatten its herniation.
Patients with very large areolae relative to their breast width should be approached with caution for a one-stage circumvertical augmentation mastopexy ( Fig. 16.6 ). If the areola width is greater than half the breast width, there is unlikely to be enough skin to allow closure of the vertical limbs of the mastopexy with the additional volume of an implant ( Fig. 16.7 ). In such cases, the surgeon has to choose between two options: (1) design a circumvertical pattern that will allow complete removal of the areola and perform a mastopexy only with insertion of an implant as a second-stage operation or (2) design a circumvertical pattern that does not completely remove the areola but allows an implant to be inserted in a single stage, knowing that a revision procedure will be required at a later date to remove the remaining areola skin along the vertical scar. In such cases, attempting to completely remove the entire areola and insert a sizeable implant can result in excessive tension on the closure with wound breakdown and extrusion of the implant.


Patients with a very long distance from the native nipple position to desired new nipple position superiorly may be better candidates for staged rather than one-stage augmentation mastopexy ( Fig. 16.8 ). As the pedicle length increases for a relatively narrow pedicle width, there is a potential for impaired NAC perfusion. These patients may require greater skin resection by a Wise pattern before augmentation in a second stage.

Other contraindications include patients with an American Society of Anesthesiologists (ASA) classification of 3 or higher, patients who are emotionally unstable, and those who do not accept the possibility of revision surgery. Smoking cessation for at least 2 weeks before and after surgery is recommended to minimize the chance of potential nipple perfusion–related problems.
Preoperative Evaluations and Special Considerations
When assessing these patients, initial questions are geared toward each patient’s desired breast size and shape. Patients who are satisfied with their current breast volume and would like better shape/positioning of the breasts are best suited for a mastopexy alone. Patients who desire larger breasts in addition to better shape/positioning and increased upper pole fullness are considered for augmentation mastopexy. Patients who desire smaller breasts are considered for reduction, which can be combined with an implant in certain circumstances in a fashion similar to that with an augmentation mastopexy. Standard questions regarding breast health are also asked, such as information on recent mammograms, previous breast surgery, and family history of breast cancer. Medications that can increase bleeding or impair wound healing are held for 2 weeks before surgery. Patients 30 years of age and older are referred for a mammogram preoperatively. Patients younger than 30 years of age with a strong family history of breast cancer also receive preoperative breast imaging.
A thorough breast examination is performed to assess for any pathologic condition, and standard breast measurements are made. Preoperatively, vertical measurements are made from nipple-to-IMF because the areola diameter is not uniform and varies from patient to patient. Intraoperatively, vertical measurements are made from inferior areola–to-IMF because the radius from the nipple to areola border is created to be about 2 cm (i.e., 4 cm areola diameter). A circumvertical “owl” is planned when the nipple-to-IMF distance is relatively short at approximately 7 cm or less on manual stretch by the surgeon’s hand. An “owl with feet” is planned when the nipple-to-IMF distance is greater than 7 cm on stretch; in such cases, the short horizontal wedge is typically adjusted intraoperatively toward the end of the operation to achieve the desired areola-to-IMF distance bilaterally (details of these markings are described later in the surgical techniques section). The patient should be counseled preoperatively that the resulting shape of the breast takes priority over the presence or absence of a small horizontal scar hidden in the IMF.
Patients who are candidates for augmentation mastopexy and have asymmetry may consider circumvertical mastopexy of the smaller breast, reduction of the larger breast by a superior pedicle technique, and insertion of the same style/volume implant bilaterally to optimize shape and symmetry. The superior pedicle reduction technique suspends the NAC in a similar fashion to the circumvertical mastopexy technique described in this chapter. Please refer to the indications section of Chapter 17 on the superior pedicle breast reduction for a more complete description of that technique for management of patients with ptosis and asymmetry.
Selecting the most appropriate implant for each patient is an important decision that begins preoperatively. This decision is not as easily determined in patients undergoing augmentation mastopexy as it is for patients undergoing augmentation only with three-dimensional imaging because the tissue dynamics can change greatly with the opposing forces of simultaneous augmentation mastopexy. Therefore, patients are asked to bring photographs of breasts they like to the preoperative visit so the plastic surgeon can understand the size/shape the patient prefers to achieve a similar size/shape intraoperatively. This greatly improves communication and understanding of expectations to minimize the revision rate for size/shape reasons. You may find that some patients prefer a very long, well-rounded nipple-to-IMF distance and slightly upward-pointing nipple, whereas others prefer a more traditional breast shape.
Several sizer and implant volumes should be available on the day of surgery because of the lower predictability of the tissue dynamics with augmentation mastopexy. A round implant is typically preferred, but an anatomic implant can be used in special circumstances. Use of a textured implant may offer some advantage in preventing capsular contracture. However, a textured implant is also more likely to remain in the superior position in which it was placed during surgery, although the breast tissue is likely to re-descend with gravity over time, potentially leading to a “waterfall” (“snoopy”) deformity. A moderate-profile implant is most commonly preferred. A high-profile implant is less frequently used because the recruitment of ptotic breast tissue onto the implant with the mastopexy typically provides satisfactory projection, and the increased projection puts greater tension on the vertical incision closure. For that reason, some surgeons prefer a low-profile implant with an increased width/height (greater cleavage and upper pole fullness) for a given volume. Ideally, the same style/volume implant is inserted bilaterally because the width/height of the implant greatly affects each breast’s shape. In cases of preoperative breast asymmetry, a small reduction of the larger breast is typically preferred (rather than placing a larger implant in the smaller breast) so the same implant can be inserted bilaterally to achieve the greatest possible symmetry.
Preoperative selection of the plane of dissection for implant insertion (subpectoral versus subglandular versus subfascial) also must be determined. We typically avoid the subglandular plane because of the capsular contracture risk and prefer either the subpectoral or subfascial planes. The primary advantage of the subpectoral plane is preservation of the perforators coursing through the pectoralis major muscle by the thoracoacromial vessels whereas the subfascial plane avoids animation deformity and has minimal postoperative pain. The subfascial plane can be a good choice in appropriately selected patients who require minimal elevation of the NAC (e.g., pseudoptosis) and desire a relatively small implant to maintain as much vascularity to the pedicle as possible. Patients undergoing subfascial implant also should have adequate soft tissue coverage in the superior pole.
Surgical Technique
The patient is marked preoperatively in the standing position. The chest midline, breast meridians, and IMFs are marked for reference. When the NAC is located medial to the breast meridian, as is commonly the case with massive weight loss or severe deflation of the breasts after childbirth and breastfeeding, the circumvertical marking is altered to adequately include the NAC and allow it to be repositioned along the breast meridian in a more cephalad position. Biparietal obstetric calipers are used to accurately transpose the position of the IMF onto the breast mound by measuring from a fixed position at the sternal notch. The new nipple position is typically marked directly at the level of the transposed IMF marking or 1 cm cephalad to the transposed IMF marking. This determination is made based on each patient’s unique anatomic features and her preferred breast aesthetic from the photographs she selected preoperatively.
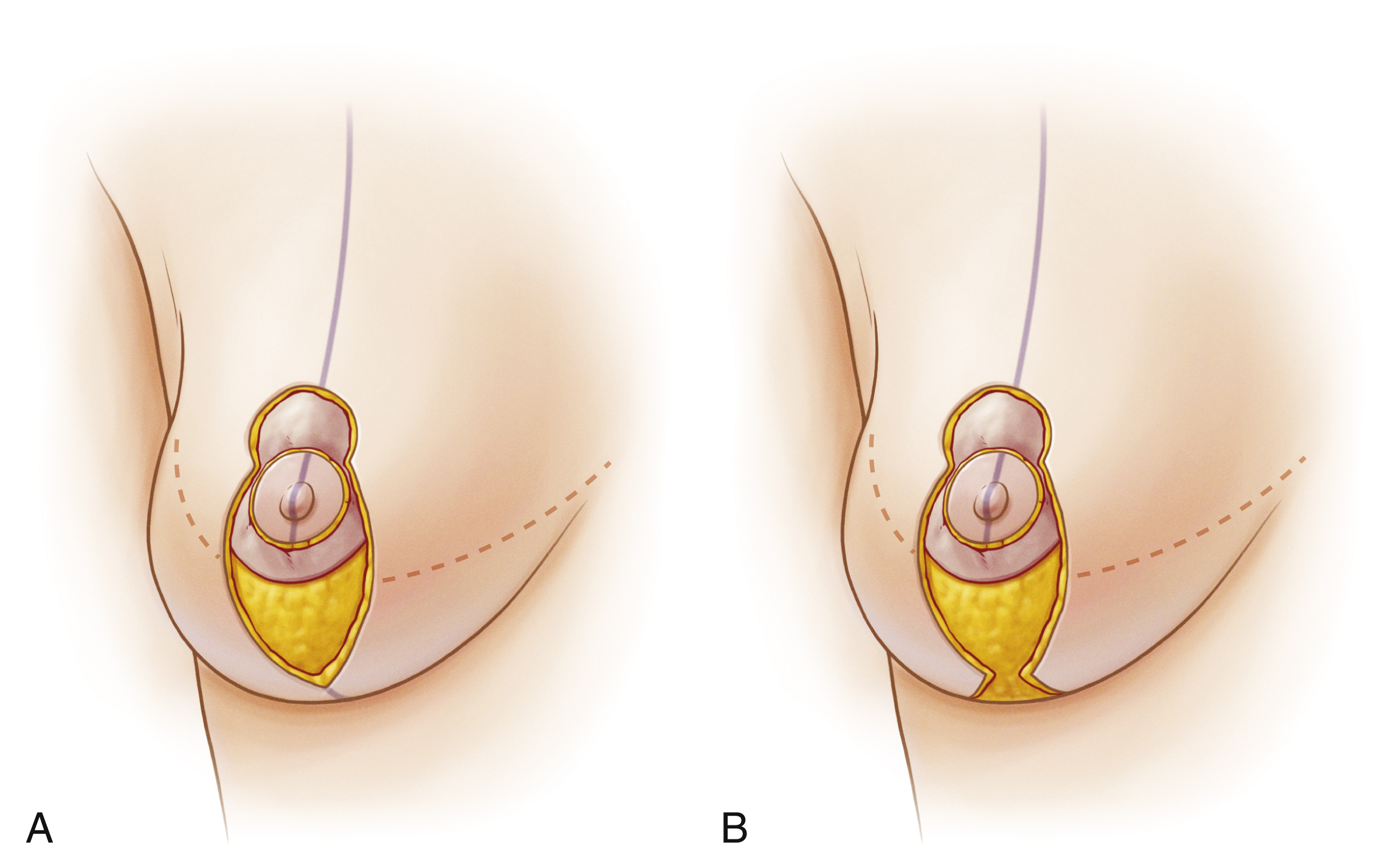
For patients with a relatively wide and/or superiorly positioned NAC combined with lower pole laxity, the new nipple position often needs to be placed 1 cm superior to the transposed IMF marking to allow the circumvertical pattern to completely encompass the NAC ( Fig. 16.9A ). A long nipple-to-IMF distance created by marking the keyhole for the NAC in a slightly more cephalad position than desired because of the patient’s anatomy can be corrected later intraoperatively; the nipple-to-IMF distance can be decreased to the desired set length at the end of the operation with removal of skin inferiorly by the short horizontal wedge of skin at the IMF (i.e., the addition of feet to the owl (see Fig. 16.9B ). The height of the body of the owl is extended inferiorly to a sharp point at or just cephalad to the IMF. The width of the body of the owl is determined by the degree of skin laxity via skin pinch in the lower pole. This width is difficult to precisely predict because it requires anticipation of the implant volume to be inserted and is largely based on experience rather than quantitative measurement. However, there are a few guidelines that can be followed to achieve success with this marking.