Bony Reconstruction of Foot and Ankle (Bone Grafts)
Kenneth Hunt
Loretta Chou
INTRODUCTION
Recent decades have witnessed a dramatic increase in available bone graft harvest techniques, bone graft substitutes, and orthobiologic technologies. Despite the extensive availability and marketing of bone graft substitutes, and their purported advantages, autogenous bone graft remains the standard for augmenting healing during arthrodesis and nonunion surgery.
Autograft bone is the only naturally occurring material purported to possess osteoconductive, osteoinductive, and osteogenic properties. Still, the use of bone grafts in orthopedic surgery has given rise to a multibillion dollar industry but has by no means eradicated nonunions in foot and ankle surgery.1,2 This chapter will discuss current bone grafting techniques and technologies for foot and ankle procedures in the context of the most common conditions and patient risk factors requiring augmentation for effective healing.
DEFINITION
Bone grafts in the foot and ankle are most commonly utilized for three indications: (a) increase the union rate for arthrodesis in revisions or joints with a known propensity for nonunion, (b) increase union rate for nonunited fractures, and (c) replace or add bone structure due to chronic or acute bone loss. The focus of this chapter is bone grafting techniques to illustrate these three indications. We include some specific, common foot pathology that requires bone grafting, but an inclusive review of foot and ankle pathologies and disease processes is outside of the scope of this chapter.
By far, the most common use of bone graft in the foot and ankle is to aid in healing for joint arthrodesis. The degeneration of joints requiring fusion can occur as a result of a number of disease processes, including post-traumatic arthritis, degenerative joint disease (DJD), posterior tibial tendon insufficiency, trauma, congenital deformity, inflammatory or crystalline arthropathy, Charcot neuropathy, diabetes, avascular necrosis, tumor, and many other causes.
Bone graft is generally incorporated to aid in healing when the risk of nonunion is unacceptably high. This is the case in patients who might have a suboptimal biologic healing response, including those with a history of smoking, diabetes, neuropathy, obesity, or a history of nonunion.3,4,5
The procedures in the foot and ankle that most commonly involve bone graft application include ankle, subtalar (ST), tibiotalocalcaneal (TTC), triple, tibiocalcaneal (TC), talonavicular (TN), calcaneocuboid (CC), naviculocuneiform (NC), and tarsometatarsal (TMT) arthrodesis, and most nonunion repairs. Due to the paucity and inconsistency of literature on the topic, the decision to use bone graft, and which type or material to use (ie, cancellous vs structural, harvest site, autograft vs allograft, bone graft substitutes, etc.), is dependent upon a host of patient factors and surgeon experience.
Generally speaking, cancellous autograft generally has a higher surface area and greater content of growth factors and remains the standard for its ability to induce more new bone formation than cortical (ie, structural) autograft or allografts.6 Structural autograft is often required when significant bone loss or deformity is present, as a means of restoring length, height, and/or alignment. The fast-growing arsenal of “orthobiologics” as substitutes for autograft are purported to rival autograft in terms of timing and rate of healing, without the morbidity of autograft harvest.
ANATOMY
The foot and ankle is composed of 28 bones. There are multiple joints, muscles, tendons, and ligaments. The foot can be divided into the medial and lateral columns. The medial column includes the talus, navicular, cuneiforms, and medial three metatarsals. The lateral column is made up of the calcaneus, cuboid, and lateral two metatarsals. Any injury, deformity, or defect can result in length alterations or stiffness in one or more columns of the foot. This can lead to pain, imbalance, and problems with weight bearing on a foot that is not plantigrade, unstable, or painful.
The ankle joint allows for most of the extension and flexion. The subtalar joint provides inversion and eversion, whereas the transverse tarsal joint (talonavicular and calcaneal cuboid) gives adduction and abduction.
The foot and ankle is responsible for gait. The heel is the first point of contact in the normal gait cycle. As the foot rolls forward, the foot changes from a flexible valgus position to a rigid varus position for push off.
The anatomy of the iliac crest, for the purposes of graft harvest discussed herein, is fairly easy to identify and superficial. The graft harvests described below are generally harvested from 2 to 4 cm above the anterior superior iliac spine (ASIS). The crest at this location can usually be palpated. Keeping the incision and dissection at least 2 cm proximal to the ASIS to avoid injury to the lateral femoral cutaneous nerve.
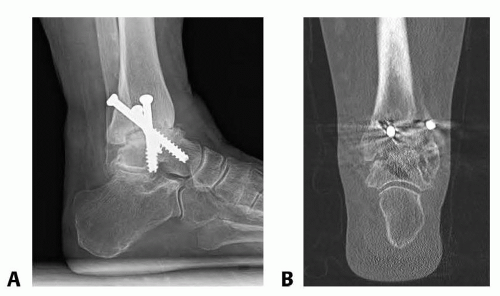 FIG 1 • A. Plain lateral radiograph. B. Coronal and sagittal CT scan images depicting a nonunion of ankle arthrodesis. |
PATHOGENESIS
The foot and ankle are the most peripheral structures in the body and are dependent during most physical activities. As a result, the foot and ankle are at higher risk of peripheral neuropathy, peripheral vascular disease, and other contributors to delayed or nonhealing of fusions or fracture fixation.
The weight-bearing role of the foot and the complexity of biomechanics for normal foot and ankle function place many regions of the foot and ankle at higher risk for abnormal loading, further contributing to delayed- or nonunion of fractures, arthrodesis, or osteotomies.
Patient risk factors known to contribute to nonhealing of bone include smoking, diabetes, age and osteoporosis, peripheral vascular disease, neuropathy, noncompliance, infection, and soft tissue injury.4
NATURAL HISTORY
The disorders of the foot and ankle are broad and significant and include trauma, arthritis, congenital, acquired, sports injuries, and degenerative conditions. With severe deformities or trauma, structural loss or nonhealing of fractures or fusions frequently lead to worsening of the disorder and pain and function, over time. Reconstructive operations may be required to repair such problems. In cases where there is need to add structural bone, or add biology, bone grafting procedures are commonly considered.
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough history is essential preoperatively. Patients are asked about injuries, chronicity, comorbidities, previous operations, and nonoperative treatment. Also, the patient’s occupation and social situation are important considerations.
Medical history should be considered when determining risk factors and the best bone graft to use. Social history is also important because patients may have particular traditions and beliefs governing whether autograft or allograft materials are acceptable. The beliefs should, and generally can, be respected during development of a treatment plan.
The physical examination takes place with the patient undressed from the knees to the toes. Gait is evaluated, as well as the skin, noting edema, scars, erythema, masses, and bony deformities. The neurovascular status is carefully examined. Evaluating potential graft sites is also important.
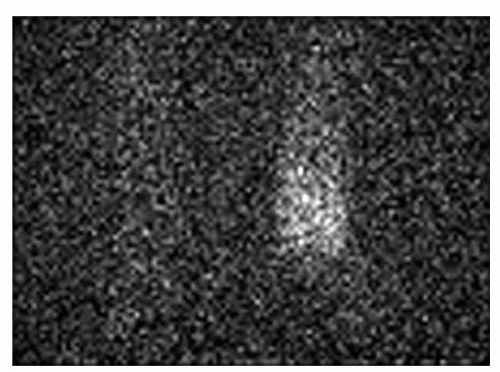
FIG 2 • Tagged WBC study demonstrating increased uptake in the left ankle compared to the right.
The foot and ankle examination can help guide surgical approach and counseling. Incisions should be made where soft tissue disruption, particularly of the well-vascularized periosteum, can be minimized. Old incisions should be incorporated whenever possible, especially when the procedure was recent.
IMAGING
Most nonunions and malunions of fractures, fusions, and osteotomies can be diagnosed on plain radiographs (FIG 1A).
For joints that are difficult to see on plain radiographs, or for complicated procedures with a large fixation construct, a CT scan is the best study to diagnose nonunion (FIG 1B).
MRI scan plays little role in diagnosing nonunion but can be helpful to evaluate soft tissue structures, which may contribute to symptoms, and is a sensitive study for osteomyelitis.
Nuclear medicine studies can aid in diagnosis of infection and osteomyelitis, which is a common contributor to nonhealing of bone (FIG 2).
DIFFERENTIAL DIAGNOSIS
Hypertrophic nonunion
Oligotrophic nonunion
Septic (infected) nonunion
Malunion
Avascular necrosis of bone
Failure of fixation
NONOPERATIVE MANAGEMENT
Nonoperative treatment for many foot and ankle disorders include activity modification, ambulatory aid, such as a cane or crutch. Physical therapy, brace, or orthotic device may be helpful. Oral medications can help reduce pain, although one must be aware of risks (eg, NSAIDs can contributed to delayed healing, narcotic analgesics carry risk of dependency).
Severe deformities may be difficult to accommodate or fit into a brace, and surgical options should be considered.
In general, if patients have persistent pain, dysfunction, problems working or participating in activities of daily living, or if there are risks to other structures or to the patient by continuing nonoperative management, surgery should be considered.
SURGICAL MANAGEMENT
The decision to augment a fusion, osteotomy, or fracture with graft is dependent on many factors, including surgeon preference and experience. Grafts should, in general, be added to increase both the likelihood and the timing of bone union in cases where nonunion or delayed union is unacceptably high. Examples include revision cases and patients with risk factors outlined above.
The authors prefer autograft iliac crest bone graft for most indications where there is high risk of nonunion. When structural grafts are necessary to span a cortical gap in bone, structural autograft from the iliac crest is generally sufficient for most procedures in the foot. Ankle and hindfoot bone loss often requires larger allografts, such as femoral head or fibular grafts.
Orthobiologics can be used in lieu of, or in addition to, other graft materials, or to add a large dose of specific growth factors to the fusion site. Examples of such orthobiologic therapies include platelet-rich plasma (PRP), bone marrow aspirate concentrate (BMAC), bone morphogenetic proteins (BMP), and platelet-derived growth factor (PDGF). The enormous recent growth of the number of available biologic products carries with it a high cost and a paucity of data on safety, effectiveness, and clinical outcomes for many products, particularly compared to the iliac crest bone graft standard. It is the responsibility of the surgeon to judiciously utilize these products with a thorough knowledge of their mechanism(s) of action, approved indications, side effect profiles, and cost.
The ultimate goal of any fusion, osteotomy, or fracture repair operation is bone healing, pain relief, and return to optimal function while avoiding complications, prolonged hospitalization, and revision operations. When a graft is selected, the surgeon must balance necessity, cost, comorbid factors, and risk and have a keen understanding of the selected graft(s) and technique.
Preoperative Planning
Plain weight-bearing radiographs of the foot and/or ankle are necessary for complete evaluation (FIG 3A).
Other imaging studies may be helpful. MRI may show extent of infection or the presence of avascular necrosis. CT scans confirm nonunion and show bone quality and structural bone loss, bony defects and deformities (FIG 3B,C).
A complete evaluation of the skin and adjacent structures must be performed, using radiographs when prudent. This should include the surgical site in the foot or ankle and any potential graft harvest site.
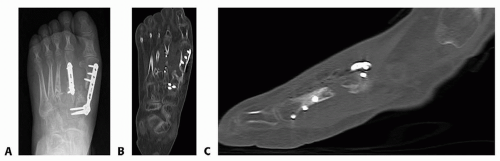
FIG 3 • A. Anteroposterior radiograph of nonunion of the first metatarsal. Axial (B) and sagittal (C) CT scans confirming the nonunion.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access