Chapter 50 Bone–Patellar Tendon–Bone Anterior Cruciate Ligament Reconstruction Using the Endobutton Continuous Loop Bone–Tendon–Bone Fixation System
The Endobutton-CL is a small metal button that is attached to a continuous loop of nylon. The continuous loop means that there is no knot, thus eliminating the risk of knots loosening or tightening under a load; both situations lead to a lengthening of a construct and thus failure. The continuous loop (CL) comes threaded through the metal Endobutton. The loop is then threaded through the graft and back on itself. Thus it is a closed loop system that eliminates a weak link. This minimizes creep or failure of the construct. It is well accepted that the weak link in ACL reconstruction surgery is fixation of the graft during the immediate postoperative period. The Endobutton-CL offers one of the strongest forms of fixation available, with pullout strengths averaging 1345N compared with interference screws that average approximately 700N.*
Technique Overview
Technique in Detail
Tibial and femoral tunnels are likewise drilled in the usual manner. In fact, the femoral tunnel can be drilled right off the posterior femoral cortex without fear of breaking through of the posterior wall, as it will not compromise fixation. I use a 6-mm offset guide for a 10-mm tunnel, which places the femoral tunnel immediately against the posterior femoral cortex. Before reaming the femoral tunnel, check the length of the graft. Grafts usually measure approximately 80 to 90 mm in total length (Fig. 50-1). Ream the femoral tunnel to a depth of the length of the graft as measured directly off the reamer at the tibial cortex. For example, if the graft length is 90 mm, ream to a depth of 90 mm as measured on the reamer at the opening of the tibial tunnel (Fig. 50-2). By doing this, the reamer is mimicking the graft itself and therefore mimicking where the graft will be placed, thus allowing the tibial bone plug to end flush with the tibial cortex. It is no longer necessary to measure the femoral tunnel; however, as a check, the femoral tunnel is usually reamed to a depth of approximately 30 mm. Then ream an extra 10 mm deeper to allow room for the Endobutton to flip outside of the lateral femoral cortex. Try to not perforate the lateral femoral cortex with the reamer. On longer grafts, you can run the risk of running out of room for the femoral tunnel. One way to effectively add length to the femoral tunnel is to flex the knee less than 90 degrees. This lessens the angle of the femoral tunnel, placing it more in line with the femur, and therefore adds length to the femoral tunnel if needed for longer grafts (Fig. 50-3). However, if there is inadvertent perforation of the femoral tunnel, it can be dealt with using the Xtendobutton, which is discussed later in this chapter.
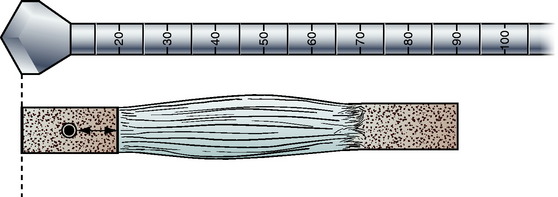
Fig. 50-1
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 EZLoc Femoral Fixation of a Soft Tissue Graft
EZLoc Femoral Fixation of a Soft Tissue Graft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


