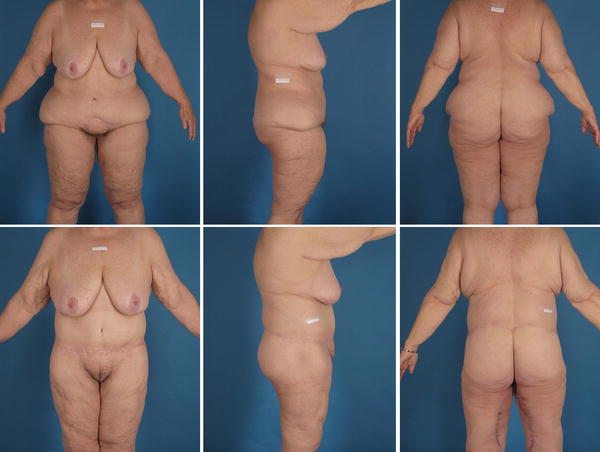
Fig. 39.1
These are nine massive-weight-loss patients. Obviously, they are quite variable in their presentation due to their presenting BMIs, their fat deposition patterns, and the varying qualities of their skin-fat envelopes
1.
The weight or BMI at presentation. The level at which any particular patient presents is dependent on many factors, which the bariatric surgeon is more expert in determining than a plastic surgeon. Thus, whenever possible the plastic surgeon welcomes the bariatric surgeon’s advice on this matter.
2.
The patient’s fat deposition pattern. Each individual is born with a genetically determined fat deposition pattern as well as a fat loss pattern. Currently, these patterns cannot be altered. Although there are many variations, the two most common patterns are “apple” and “pear” fat deposition patterns (Fig. 39.2).

Fig. 39.2
The fat deposition pattern of any particular individual is genetically controlled. This figure demonstrates the two most common patterns encountered
3.
The quality of the skin-fat envelope. The skin-fat envelope will vary in thickness, pliability, and laxity. The variability in quality is based on the genetics of the patient, their age, and the amount of weight loss they experienced.
Because of the variability in the presentation of massive-weight-loss patients, treating their resultant deformities in the same manner can lead to less than ideal results. Thus, the plastic surgeon must tailor their surgical options based on the individual needs of the presenting massive-weight-loss patient.
Workup for Post-Massive-Weight-Loss Plastic Surgery
A complete history and physical must be performed on these patients. The key points of the history that relate to plastic surgery include [1, 2]:
1.
Weight loss history. Generally, a 100-lb weight loss is considered the amount of weight lost that is needed to create the usual body contour changes associated with massive weight loss. However, a more accurate way to make that determination is a ten point, or greater, drop in body mass index (BMI).
2.
The type of bariatric surgery performed, if the patient lost weight through surgical means. If the patient had a lap band, where was the port placed and how is it accessed?
3.
The anatomic areas of most concern and highest priority to the patient.
4.
Previous abdominal surgeries.
5.
Medical problems, i.e., diabetes, heart disease, high blood pressure, etc.
6.
Smoking history.
7.
Psychiatric history.
The key points of the plastic surgery physical exam:
1.
Weight, height, and BMI.
2.
The fat deposition pattern.
3.
The quality of the skin-fat envelope.
4.
The extent of intra-abdominal/visceral fat content. This is especially important because if there is persistent overabundance of visceral fat, the plastic surgeon will not be able to flatten the abdomen, which is one of the main desires of massive-weight-loss patients.
5.
Abdominal scars and their locations. Old subcostal “chevron”-type scars can affect vascularity of the abdominal flap during abdominal contouring surgery.
6.
The presence and extent of an abdominal panniculus. This is important because it is usually the only aspect of the massive-weight-loss patient’s anatomy that may qualify for insurance coverage.
7.
The extent of rectus muscles diastasis.
8.
The lipodystrophy and ptosis of the lateral and posterior aspects of the trunk.
9.
Mons pubis extent of lipodystrophy and ptosis.
10.
The location of a lap band port if present. Almost all massive-weight-loss patients present with abdominal wall laxity, which is treated by plicating the rectus fascia in a vertical fashion, from xiphoid to pubis. Ports located within the extents of the plication will have to be moved during abdominal contouring procedures.
11.
The amount and extent of upper arm excess.
12.
The presence and extent of upper back rolls.
13.
The condition of the breasts. In males, this usually presents as excessive breast tissue. In females, the presentation is quite variable. Some women will present with persistent breast hypertrophy, while others will present with hypomastia, but most often they will present with very ptotic and deflated breasts.
14.
The extent of skin and fat content of the thighs.
Laboratory examination of the massive-weight-loss patient in preparation for plastic surgery is rather extensive compared to other surgical workups. This is because many post-bariatric surgery patients, especially those that are not carefully followed by their bariatric surgeons, present with nutritional deficits that do not manifest clinically unless stressed by the wound healing requirements of the extensive body-contouring procedures discussed later. These examinations include CBC w/differential, electrolytes (sodium, chloride, potassium, CO2, anion gap), albumin, liver function tests, BUN, creatinine, calcium, cholesterol, ferritin, glucose, magnesium, total protein, PT/PTT, vitamin B12, copper, and thiamine.
Treatment
There are a number of areas in the body that are bothersome to patients at presentation and they will be discussed later in the most common order of patient concern. However, it is important to note there are always exceptions and variations in patient desires and priorities. These issues have to be taken into account as a treatment plan is formulated for any individual patient.
The Lower Trunk
The boundaries of the lower trunk include the abdomen, from inframammary crease to the pelvic rim anteriorly, the mid to lower back posteriorly, and the hip and waist region laterally. The majority of massive weight patients have a hanging panniculus as their primary concern. They will also complain of a ptotic mons pubis, excess skin and fat of the hip and waist region, ptosis of the anterior and lateral thighs, and ptosis of the buttocks.
The lower trunk in almost all massive-weight-loss patients has circumferential excess. Abdominoplasty in its various forms will most often lead to less than ideal results because it treats only part of the circumferential problem (Fig. 39.3). In order to treat the entire range of deformities in these patients, a circumferential dermatolipectomy is usually needed. Other names for this procedure include belt lipectomy (the author’s preferred term) [3], body lift, lower body lift, circumferential abdominoplasty, and torsoplasty. This fairly complex procedure involves excision of a circumferential wedge of tissue in the shape of a “boxing championship belt,” wide anteriorly and narrow posteriorly. It requires multiple turns in the operating room and is most often performed under a general anesthetic. Figure 39.4 shows the markings as performed by the author. The skin-fat envelope is removed from the superior to the inferior horizontal line markings. The vertical lines are placed for alignment during closure. Most patients are postoperatively monitored in a controlled setting for 1–3 days. The procedure accomplishes the following in most patients:
Get Clinical Tree app for offline access
Fig. 39.3
Top row
 Duodenal Switch: Technique and Outcomes
The Rationale for Metabolic Surgery
Liability Reduction, Patient Safety, and Economic Success in Bariatric Surgery
Duodenal Switch: Technique and Outcomes
The Rationale for Metabolic Surgery
Liability Reduction, Patient Safety, and Economic Success in Bariatric Surgery
 Operative Outcomes of Bariatric Surgery in Patients with a Low Body Mass Index (30–35 kg/m2)
Operative Outcomes of Bariatric Surgery in Patients with a Low Body Mass Index (30–35 kg/m2)
 Gastrointestinal Obstruction After Bariatric Surgery
Gastrointestinal Obstruction After Bariatric Surgery
 Laparoscopic Adjustable Gastric Banding: Technique and Outcomes
Laparoscopic Adjustable Gastric Banding: Technique and Outcomes




Related posts:
Duodenal Switch: Technique and Outcomes
The Rationale for Metabolic Surgery
Liability Reduction, Patient Safety, and Economic Success in Bariatric Surgery
Operative Outcomes of Bariatric Surgery in Patients with a Low Body Mass Index (30–35 kg/m2)
Gastrointestinal Obstruction After Bariatric Surgery
Laparoscopic Adjustable Gastric Banding: Technique and Outcomes
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
