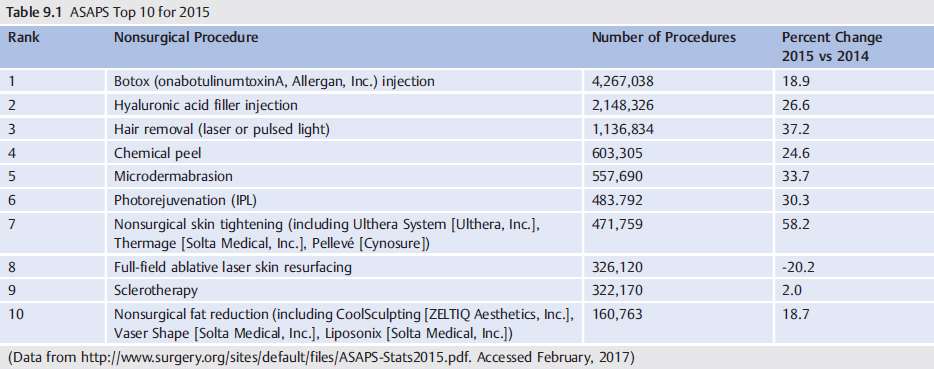
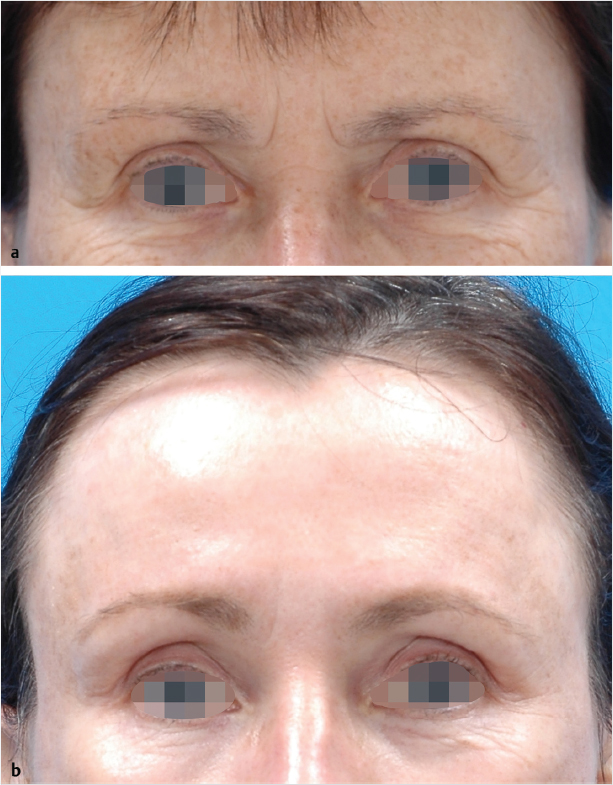
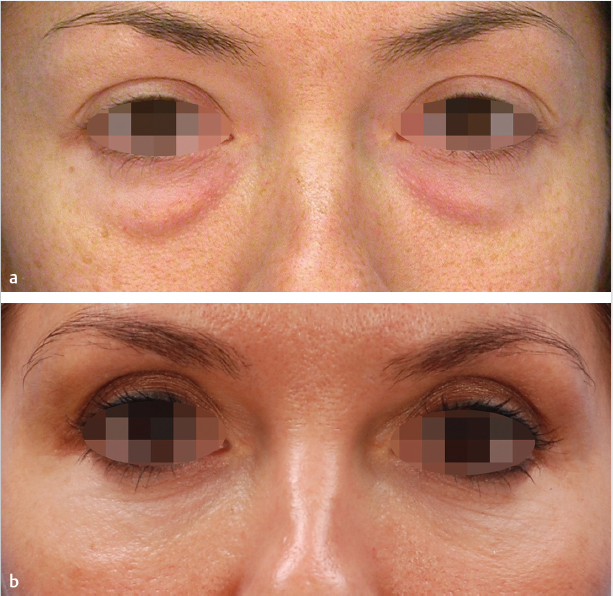
9 Blending Nonsurgical Treatments with Surgery for Facial Rejuvenation Summary Nonsurgical therapy can be a prelude to cosmetic surgery for patients not yet ready for surgery, either as an adjunct to surgery or after surgery. The goal of using the blending of surgical and nonsurgical treatments is to obtain a more complete correction than what can be achieved through surgery alone. Keywords: Botox (onabotulinumtoxinA, Allergan, Inc.) injection, chemical peel, hyaluronic acid filler injection, laser hair removal, laser skin resurfacing, microdermabrasion, nonsurgical, facial rejuvenation, nonsurgical skin tightening, photorejuvenation, pulsed light hair removal, surgical Key Points • Surgical and nonsurgical approaches are commonly combined in modern-day facial rejuvenation. • Nonsurgical treatments may precede surgical intervention or be used concomitantly or subsequently for maintenance or additional correction. • Some nonsurgical techniques address issues that are separate from surgical treatments, such as intense pulsed light (IPL) therapy for age spots and facelifting for laxity. • Some nonsurgical and surgical techniques represent alternative approaches to treating the same problem, such as microfocused ultrasound and facelifting for laxity, or injectable filler and fat injection for volume loss. • Nonsurgical techniques and technologies are undergoing rapid development and are taking the lead in the care of the aging face. Surgical rejuvenation of the face has been the mainstay of therapy for many years, but many nonsurgical options and adjuncts have been introduced recently. Data from the American Society of Plastic Surgeons (ASAPS) collected annually since 1997 have shown the rapid rise of nonsurgical options for facial rejuvenation1 ( Facial rejuvenation surgery includes brow lifting, eyelidplasty, midface lifting, and facelift. Nonsurgical or minimally invasive procedures may be used alongside these procedures or as a replacement for some of these procedures while in surgery. Postsurgical adjuncts will be discussed in the next section. In the mid-1990s, the procedures for browlifting underwent a change in many plastic surgeons’ practices from coronal or hairline incisions to endoscopic techniques. Recently there has been an aesthetic shift toward a more natural, less elevated brow, and many surgeons have limited their use of browlifts to those patients with very significant brow ptosis. For patients who need just a small amount of brow elevation, the question that now arises is what techniques could be used as an adjunct when other procedures (i.e., facelift) are performed. Several useful options are discussed. In addition to creating a fresh epidermal surface and smoothing of the dermal rhytids, laser resurfacing may be used to elicit some brow elevation. This is most likely due to collagen remodeling and new collagen and elastin deposition. Although there has not been a formal study of this phenomenon, the elevation seems to persist and needs further study ( Microfocused ultrasound has had FDA approval for brow elevation since 2010. This procedure is generally used in lieu of surgery for patients who require only a modest improvement in brow elevation or to improve brow symmetry. However, microfocused ultrasound can also be performed in the operating room while the patient is under anesthesia for another surgical procedure for the face, which avoids the discomfort that is often experienced during the treatment as a standalone. Microfocused ultrasound has the ability to focus on different areas of the brow that may not be successfully elevated by the particular brow procedure being utilized by the surgeon. This provides more complete correction or can amplify the correction applied to brow ptosis or brow asymmetry, which is currently not completely addressed by any procedure. Filling of the upper periocular area or brow with fillers or fat may be used to elevate the eyebrow or fill the brow to give the illusion of an elevated brow. This can easily be performed simultaneously with other facial surgery. Such contouring can also correct hollowing of the upper eyelid sulcus resulting from overresection of orbital fat during previous upper eyelid surgery or caused by aging changes. Fig. 9.1 (a) Before and (b) 1 year after full-face laser resurfacing, Note the brow elevation. Botulinum toxins can be used to modify the upper face musculature. Conceivably, they may be administered during facial rejuvenation surgery either to provide immediate correction or on the theory that blocking animation during healing improves the “take” of the correction. Although this theory is appealing, there is no meaningful data to support or refute the efficacy of such an approach. We prefer to use botulinum toxins after surgery when the patients can animate, allowing more precise placement and dosing. Radiofrequency (RF) microneedling has anecdotally proved to be useful for smoothing mild skin laxity (see Chapter 7). Although there is no formal FDA approval at this time, these devices may be used during other facial surgery for brow elevation. Eyelid surgery is a very common procedure in plastic surgery, with just under 170,000 surgeries being performed by core physicians in the United States in 2015.1 Trends in eyelid surgery are for a more natural, less operated look. For this reason, current techniques for upper eyelid surgery involve less removal of orbital fat to avoid hollowing. Occasional volume replacement is needed, even in primary cases and especially in older patients. Lower lid techniques increasingly use the transconjunctival approach, avoiding skin excision or limiting skin excision to a skin-only pinch. This amplifies the need to address skin texture, redundancy, and laxity issues in the lower lid. There are many nonsurgical adjuncts that can be used along with more traditional surgical techniques.2 Laser resurfacing is the mainstay of our nonsurgical facial adjunctive techniques. There are a variety of lasers that may be used for eyelid rejuvenation, but our preference is to use the variable pulse-width erbium laser (Sciton, Inc.) in a nonfractional full-field mode. This laser may be used on the upper and lower eyelids as a replacement for excisional techniques or along with excisional techniques. It is very common in our practices to perform traditional excisional upper lid blepharoplasty with laser resurfacing of the area from the incision line to the inferior portion of the eyebrow. This achieves additional elevation and correction of some skin laxity ( A widespread approach for lower eyelid rejuvenation is laser resurfacing.3 This is often combined with transconjunctival fat removal and with a skin pinch for those cases with marked skin excess. Skin muscle flaps or subcutaneous lower blepharoplasties should not be resurfaced simultaneously to avoid skin necrosis and an increased risk of lid retraction. Aside from surgical interventions, multiple nonsurgical modalities are available to rejuvenate periocular skin. Microfocused ultrasound has a role in the periocular area, but it cannot be used within the confines of the orbit itself for fear of damaging the globe.4 Fig. 9.2 (a) Before and (b) 13 years after tranconjunctival blepharoplasty and laser resurfacing. It is very common to fat graft the periocular area during other facial surgery. Lateral brow filling or tear trough filling with minimal fat aliquots is considered a standard procedure at this time. The use of nonfat fillers, such as hyaluronic acids in the periocular area, is possible but probably better off performed postoperatively for increased accuracy. Controversy exists over the best techniques for fat harvest, processing, and grafting. Micrograft processing or harvesting techniques (sometimes called nanofat grafting), those designed to produce very small graft particles, are more likely to be employed when grafting in the periocular area. Whether this improves the percent of graft take or reduces the risk of visible nodules in this treacherous area is unknown at this time5( Botulinum toxins (Botox, OnabotulinumtoxinA, Allergan; Dysport, abobotulinumtoxinA, Balderma Laboratories LP; Xeomin, incobotulinumtoxinA, Mert North America, Inc.) are routinely used in the periocular area, but most plastic surgeons would perform these injections either as a precursor or after surgery. There is no advantage to using botulinum toxins during a facial surgical procedure. There is a theoretical advantage to having an area resurfaced for rhytides in an adynamic state during healing to provide the best result, although substantiating evidence for this benefit is lacking. Surgical options for the midface are lifting or volumizing with the use of implants. Endoscopic or open midface lifting techniques were very common in the past, but they have fallen out of favor with the increased use of fat grafting. This is true for several reasons: 1. Endoscopic and midface techniques were typically used in younger patients with mild laxity or shape change (flattening) in the midface area. 2. For mild laxity, volume addition with fat grafting or fillers can restore shape, and such re-expansion of the soft tissue space greatly reduces or eliminates mild laxity of the skin envelope in this area. 3. The recovery time and risk associated with fat grafting is substantially less than that associated with midface lifting and with endoscopic facelift, both of which were also notorious for undercorrection or incomplete correction deficiencies despite the significant recovery. 4. Patient perceptions of the relative degree of invasiveness of fat grafting compared to mini-facelift variants may also be driving the end results in procedure selection. Cheek implants have also been supplanted largely in recent times with fat grafting or off-the-shelf filler injections. Cheek implants can create a larger and certainly more-defined shape than fat grafting or lifting procedures. A role for these treatments remains, particularly in the patient who desires a durable result. The use of barbed sutures to lift the cheeks was a common procedure a few years ago as an alternative procedure for facial rejuvenation, but some surgeons used them during facelift as an adjunct to elevate the midface. Now, however, the use of permanent barbed sutures for midface lifting has been pretty much abandoned. Recently, a new absorbable suture with cones was introduced for facial lifting (Silhouette Instalift, Sinclair Pharma plc). This procedure is intended for those patients who are not yet ready for a more extensive facial lifting procedure or for those patients who are not considered to be good candidates for surgery (see Videos 2.6, 2.7, 2.8 and 2.9). The absorbable barbed threads last approximately 2 years but also cause some filling of the area due to a stimulation of tissue growth. These sutures could conceivably be used as an adjunct to facelift to achieve more midface elevation or for the SMAS/platysma tissues to more evenly distribute the tension along the suspension. Fat grafting is now considered a routine option during surgical facial rejuvenation for many plastic surgeons. The midface is the area most suitable for facial volume restoration, and we routinely perform fat grafting during facelifts in patients who manifest moderate or severe volume depletion. As previously mentioned, many plastic surgeons have abandoned the use of cheek implants or midface lifting techniques in favor of fat grafting. Specific features that can be modified include projection of the malar eminence, inferomedial cheek curvature, and submalar hollowing. Additional fill in the prejowl sulcus, nasolabial folds, marionette lines, and temples are also commonly employed. The use of nonfat fillers, as with the periocular area, may be used during the facelift but probably is more accurate and easier after healing occurs. Laser resurfacing during facelift surgery is routinely employed. This serves as a way to improve the quality of the aging skin that redraping alone is unable to accomplish, bringing the patient to a more complete correction. Skin surface features like rhytides, solar lentigines, and assorted pigmentary and textural issues can be addressed, while initiating a protracted period of increased collagen synthesis in the skin. The resulting skin, which looks and biologically acts more like youthful skin, is an important component of meaningful facial rejuvenation. When laser resurfacing is undertaken during facelift alone, central areas of the face such as the forehead, glabella, and periorbital and perioral regions may be resurfaced in a fashion similar to that used as standalone procedures. Full-face laser resurfacing during facelifting allows the entire block of facial skin to be addressed in one step. However, significant modifications in technique are required over the undermined flaps to allow full-face laser resurfacing to be performed concomitantly with face-lift.6,7 Full-field resurfacing using a variable pulse Erbium:YAG laser (Sciton, Inc.) with limited fluences over the medial nonundermined cheek and use of the profractional (fractional erbium) component with very superficial settings over the undermined flap, minimizes risks of flap necrosis and healing delay (see Product Index (p. 176)). Resurfacing may be delayed until after the facelift heals to allow a much more aggressive resurfacing to be performed. This approach will be discussed in the Postoperative Care, Complications, and Shortcomings section (p. 102). This is an area routinely rejuvenated with complementary techniques during facial surgery. The problems are usually loss of volume with or without skin laxity or wrinkling issues. Fat grafting to the perioral area is a routine part of facial rejuvenation surgery. The lips and marionette lines are routinely fat grafted if indicated. A state-of-the-art facelift is capable of creating mild improvement in these features but will never produce complete correction without unwanted facial distortion. An additional technique must be employed to obtain optimum correction. As in the other areas, the use of nonfat fillers to the perioral area is possible but easier if done preoperatively or postoperatively. The use of laser resurfacing of the periocular area is routine during facelift. As with the other areas, the variable pulse erbium laser (Sciton, Inc.) is used in the periocular area and there are no changes in technique or fluences for laser resurfacing performed prior, during, or after facelift. Certainly, a single recovery period has advantages for the patient if procedures are performed concurrently. Safety precautions must be taken to avoid combustion of supplemental oxygen in this area. If no closed airway is present, oxygen should be discontinued several minutes before laser exposure. For endotracheal tubes or laryngeal mask airways, additional shielding must be employed unless the tube is specifically designated as a laser-safe tube. Similarly, deep chemical peels (or light) may be used in the perioral area during facelift. The debate over the relative merits of laser resurfacing versus chemical peeling has gone on for the past two decades and is beyond the scope of this chapter. Ideally, surgeons select the technique that works best in their hands based on their training and experience. Compared to laser resurfacing, chemical peeling results are more heavily dependent on the skill and experience of the provider ( There are a number of aging changes present in the neck that are not well addressed by surgical skin redraping but are increasingly treatable with a variety of nonsurgical, energy-based techniques. These can be used during surgery in some cases, but neck skin is considerably less forgiving and slower healing than facial skin, having typically 1000-fold fewer adnexal structures, which can act as a reservoir of healing cells for epithelialization.
9.1 Introduction
![]() Table 9.1). Nonsurgical therapy can be a prelude to cosmetic surgery for patients who are not yet ready for surgery, or it can be an adjunct to surgery or performed after surgery. There are many publications dedicated to nonsurgical therapy. This book is dedicated to the blending of surgical and nonsurgical treatments, so adjuncts to surgery and postsurgical procedures will be discussed in this chapter. The goal of using adjuncts is to obtain a more complete correction than what can be achieved through surgery alone. While surgery performs the bulk of correction in cases of laxity in aging faces, certain areas of the face are notorious for persisting, to the chagrin of surgeons and patients together.
Table 9.1). Nonsurgical therapy can be a prelude to cosmetic surgery for patients who are not yet ready for surgery, or it can be an adjunct to surgery or performed after surgery. There are many publications dedicated to nonsurgical therapy. This book is dedicated to the blending of surgical and nonsurgical treatments, so adjuncts to surgery and postsurgical procedures will be discussed in this chapter. The goal of using adjuncts is to obtain a more complete correction than what can be achieved through surgery alone. While surgery performs the bulk of correction in cases of laxity in aging faces, certain areas of the face are notorious for persisting, to the chagrin of surgeons and patients together.
9.2 Adjunctive Treatments During Facial Rejuvenation Surgery
9.2.1 Browlifting
9.2.2 Laser Resurfacing
![]() Fig. 9.1).
Fig. 9.1).
Microfocused Ultrasound
Fillers and Fat Grafting
Botulinum Toxins
Other Tightening or Lifting Devices
9.2.3 Eyelidplasty
Laser Resurfacing
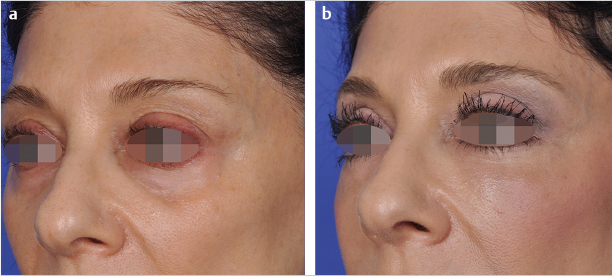
![]() Fig. 9.2).
Fig. 9.2).
Fat Grafting and Fillers
![]() Fig. 9.3).
Fig. 9.3).
Botulinum Toxins
9.2.4 Midface
Suture Lifts
Fat Grafting and Fillers
Laser Resurfacing
9.2.5 Perioral Area
Fat Grafting and Fillers
Laser Resurfacing and Chemical Peels
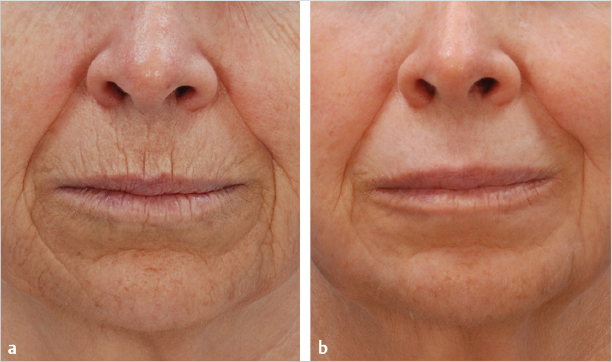
![]() Fig. 9.4).
Fig. 9.4).
9.2.6 Neck
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine