Biology of Nails
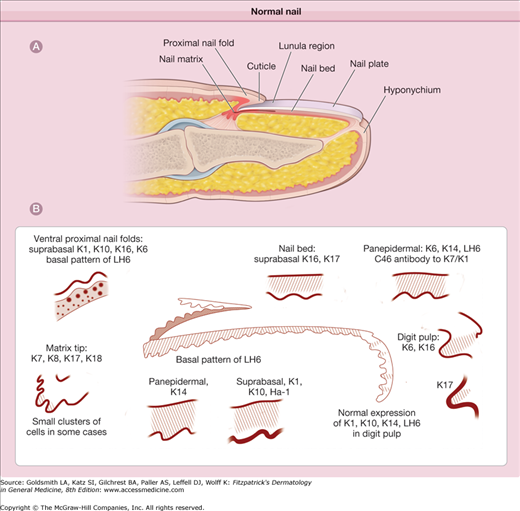
The nail apparatus consists of a horny “dead” product, the nail plate, and four specialized epithelia: (1) the proximal nail fold, (2) the nail matrix, (3) the nail bed, and (4) the hyponychium (Fig. 89-1A). The nail apparatus develops during the 9th embryonic week from the epidermis of the dorsal tip of the digit as a rectangular area, the nail fold that is delineated by a continuous groove.1 The proximal border of the nail fold extends downward and proximally into the dermis to form the nail matrix primordium. By the 15th week the nail matrix is completely developed and starts to produce the nail plate, which will continue to grow until death. The nail apparatus lies immediately above the periosteum of the distal phalanx. The intimate anatomic relationship between the nail and the bone is responsible for the common occurrence of bone alterations in nail disorders and vice versa. The shape of the distal phalangeal bone also determines the shape and the transverse curvature of the nail.
Fingernails usually present a longitudinal major axis and toenails a transverse major axis. The ratio between length and width is important for the aesthetic appearance of the nails. The size of the nails varies in the different digits. The biggest nail is that of the first toe, which covers approximately 50% of the dorsum of the digit.
Nails have numerous functions. Fingernails not only contribute to the pleasing appearance of the hands, but are very important in protecting the distal phalanges and enhancing tactile discrimination and the capacity to pick up small objects. They are also widely used for scratching and grooming and are an efficient natural weapon. Toenails protect the distal toes and contribute to pedal biomechanics.
(See Fig. 89-1A)
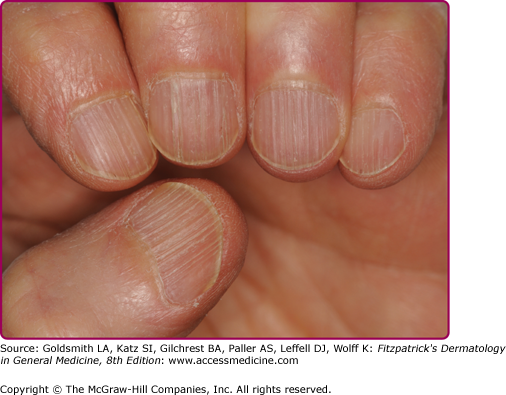
The nail plate is a fully keratinized structure that is continuously produced throughout life (see Fig. 89-1B). It results from maturation and keratinization of the nail matrix epithelium and is firmly attached to the nail bed, which partially contributes to its formation. Proximally and laterally the nail plate is surrounded by the nail folds, which cover its proximal third and lateral margins. At the tip of the digit, the nail plate separates from the underlying tissues at the hyponychium. The nail plate is rectangular, translucent, and transparent. It is curved in both the longitudinal and transverse axes, especially in the toes. The nail plate surface is smooth but frequently shows mild longitudinal ridges that increase with aging (Fig. 89-2). The pattern of these ridges can be used for forensic identification. The bottom of the nail plate shows longitudinal ridges that correspond to the rete ridges of the nail bed. The nail plate is homogeneously pink, except for its free edge, which is white. The pink color of the nail plate is due to the nail bed blood vessels.
The proximal part of the fingernails, especially of the thumbs, shows a whitish, opaque, half-moon-shaped area, the lunula that is the visible portion of the nail matrix. In this area the nail plate attachment to the underlying epithelium is loose. More than 90% of fingernails show a thin distal transverse white band, the onychocorneal band, better defined as the isthmus, which marks the most distal portion of firm attachment of the nail plate to the nail bed.2,3 This area represents an important anatomic barrier against environmental hazards, and its disruption produces nail plate detachment with onycholysis. The onychocorneal band is separated from the nail plate white free edge by a 1.0–1.5-mm pink band called the onychodermal band.
In transverse sections, the nail plate consists of three portions: (1) dorsal nail plate, (2) intermediate nail plate, and (3) ventral nail plate.4 The dorsal and the intermediate portions of the nail plate are produced by the nail matrix, whereas its ventral portion is produced by the nail bed. Above the lunula the nail plate is thinner and consists only of the dorsal and intermediate portions. There is a natural line of cleavage between the dorsal and the intermediate nail plate.
The nail plate progressively thickens from its emergence to its distal margin. The mean toenail thickness at the distal margin is 1.65 ± 0.43 mm in men and 1.38 ± 0.20 mm in women. Fingernails are thinner; the mean thickness is 0.6 mm in men and 0.5 mm in women. There is an increase in nail thickness with age, particularly in the first two decades. Nail thickness depends on the length of the nail matrix and nail bed.5 Thinning of the nails is usually a sign of nail matrix disorders, whereas nail thickening is most commonly a consequence of nail bed disorders.
(See Fig. 89-1A)
The proximal nail fold is a skin fold that consists of a dorsal and a ventral portion. The dorsal portion is anatomically similar to the skin of the dorsum of the digit but thinner and devoid of pilosebaceous units. The ventral portion, which cannot be seen from the exterior and proximally continues with the germinative matrix, covers approximately one-fourth of the nail plate. It closely adheres to the nail plate surface and keratinizes with a granular layer. The limit between the proximal nail fold and the nail matrix can be histologically established at the site of disappearance of the granular layer.
The horny layer of the proximal nail fold forms the cuticle, which is firmly attached to the superficial nail plate and prevents the separation of the plate from the nail fold. The integrity of the cuticle is essential for maintaining the homeostasis of this region.
The dermis of the proximal nail fold contains numerous capillaries that run parallel to the surface of the skin and may easily be observed in vivo by capillary microscopy. This permits the observation of both the arterial and the venous limbs of the capillaries, which are arranged in parallel rows and appear as fine regular loops with a small space between the afferent and efferent limbs. The morphology of proximal nail fold capillaries is typically altered in connective tissue diseases.6–8
(See Fig. 89-1A)
The nail matrix is a specialized epithelial structure that lies above the mid portion of the distal phalanx. After elevation of the proximal nail fold, the matrix appears as a distally convex crescent with its lateral horns extending proximally and laterally.
In longitudinal sections the matrix has a wedge-shaped appearance and consists of a proximal (dorsal) and a distal (ventral) portion. Nail matrix keratinocytes divide in the basal cell layer and keratinize in the absence of a granular zone. The site of keratinization (keratogenous zone) of nail matrix onychocytes can be clearly distinguished in histological sections as an eosinophilic area where cells show fragmentation of their nuclei and condensation of their cytoplasm.1 In this area, nuclear fragments are destroyed by deoxyribonuclease and ribonuclease enzymes. In some conditions nuclear fragments may persist within the intermediate nail plate, producing leukonychia spots. However, these frequently disappear before reaching the nail-free edge, due to the persistence of active DNA and RNA lytic enzymes within the horny nail plate.
Maturation and differentiation of nail matrix keratinocytes do not follow a vertical axis, as in the epidermis, but occur along a diagonal axis that is distally oriented. For this reason, keratinization of the proximal nail matrix cells produces the dorsal nail plate and keratinization of the distal nail matrix cells produces the intermediate nail plate.
In some fingers the distal matrix is not completely covered by the proximal nail fold but is visible through the nail plate as a white half-moon-shaped area, the lunula. The white color of the lunula results from two main anatomic factors: (1) the keratogenous zone of the distal matrix contains nuclear fragments that cause light diffraction, (2) nail-matrix capillaries are less visible than nail bed capillaries because of the relative thickness of the nail-matrix epithelium.9
(See Fig. 89-1B).
The nail matrix cells are able to synthesize both “soft” or skin-type and “hard” or hair-type keratins.10–12 Evaluation of keratin expression in the different constituents of the nail apparatus showed that the nail matrix is the sole site of expression of hard keratin proteins, particularly Ha1 keratin.13 Data indicate that fibroblasts derived from the nail matrix may induce hard keratin expression in nonnail-matrix keratinocytes.14
(See Chapter 72).
Nail matrix melanocytes are usually quiescent and therefore not detectable in pathologic sections. However, they possess the key enzymes that are necessary for melanin production, and may become activated by a large number of physiologic and pathologic conditions.15 Nail matrix melanocyte activation produces diffuse or banded nail pigmentation and is more common in blacks and Japanese than in Caucasians. DOPA-negative (inactive) melanocytes are sparsely present in the nail matrix and in the nail bed.16 DOPA-positive, activable melanocytes are especially seen in the distal nail matrix, where they are frequently arranged in small clusters among the suprabasal layers of the nail matrix epithelium.17
(See Chapter 10).
Langerhans cells are more numerous in the proximal than in the distal nail matrix. As in normal epidermis, Langerhans cells are predominantly found in the suprabasal layers. However, they may occasionally be seen within the basal layer of the nail matrix epithelium.
The presence of Merkel cells in the nail matrix has been demonstrated. Their density is possibly influenced by age, with these cells being more numerous in fetus than in adult nails.18
(See Fig. 89-1A)
The nail bed extends from the distal margin of the lunula to the isthmus and is completely visible through the nail plate. The nail bed epithelium is so adherent to the nail plate that it remains attached to the undersurface of the nail when the latter is avulsed.
The nail bed epithelium is thin and consists of two to five cell layers. Its rete ridges, which are longitudinally oriented, interdigitate with the underlying dermal ridges in a “tongue-and-groove”-like fashion. The nail bed epithelium is a specialized epithelial structure with a horny layer that interlocks to of the inferior border of the nail plate and is responsible for the strong attachment between the two tissues. Nail bed horny layer forms the ventral nail plate, which corresponds to approximately one-fifth of the terminal nail thickness and mass.19 In pathologic sections, the ventral nail plate is easily distinguishable because of its light eosinophilic appearance. Nail bed keratinization is not associated with the formation of a granular layer. This may appear, however, when the nail bed becomes exposed after nail avulsion.1
The nail isthmus is a thin transverse distal band that represents a transitional zone between the nail bed and the hyponychium and exhibits a unique pattern of keratinization, the onycholemmal keratinization, with pale, nucleated keratinocytes. The cornified layer of the nail isthmus closely adheres to the undulating inferior surface of the nail plate preventing onycholysis; the two grow forward together.3 Keratin expression in the nail bed differs form that of the nail matrix since keratins K6, K16, and K6hf are only expressed in the nail bed.20 The isthmus differs from nail bed because of a strong suprabasal expression of K10. Transition from isthmus to hyponychium is marked by the disappearance of expression of K6hf and K6/16, and return to expression of K5/17.
The hyponychium marks the anatomic area between the nail bed and the distal groove, where the nail plate detaches from the dorsal digit (see Fig. 89-1A). Its anatomic structure is similar to that of plantar and volar skin, and keratinization occurs through the formation of a granular layer. The horny layer of the hyponychium partially accumulates under the nail plate free margin. The hyponychium is normally covered by the distal nail plate, but it may become visible in nail biters. The architecture of the capillary network of the hyponychium dermis consists in regular capillary loops arranged perpendicularly to the skin, visible as red dots with dermoscopy.
The antigenic structure of the basement membrane zone of the nail is identical to that of the epidermis, and there are no differences in the antigenic composition of the basement membrane zone in the different portions of the nail apparatus.21 This may explain the involvement of the nails in conditions characterized by mutations of basement membrane-associated genes as well as in autoimmune skin diseases involving the basement membrane zone antigens.22
(See Fig. 89-1A)
The nail apparatus is devoid of subcutaneous tissue, and its dermis does not contain pilosebaceous units. The arrangement of the rete ridges varies in the different portions of the nail apparatus. The dermis beneath the proximal nail matrix consists of condensed connective tissue that forms a tendon-like structure connecting the matrix to the periosteum of the proximal phalangeal bone (posterior ligament). A small amount of subdermal fat tissue is present close to the periosteum of the base of the phalanx.23 The close connection between the lateral horns and the periosteum is possibly responsible for the nail plate’s lateral convexity. The rete ridges of the dermis underneath the nail matrix are characteristically long and root-like in shape. The dermis under the distal matrix consists of a loose network of connective tissue containing numerous blood vessels and rare glomus bodies.
The dermis of the nail bed has a unique arrangement with longitudinal grooves and ridges that run from the lunula to the hyponychium.1 The longitudinal orientation of the capillary vessels within the nail bed grooves explains the linear pattern of nail bed hemorrhages (splinter hemorrhages). The nail bed dermis contains abundant connective tissue networks with connective tissue bundles radiating to the phalangeal periosteum. It contains numerous glomus bodies.
The nail apparatus has an abundant blood supply provided by the lateral digital arteries. These run along the sides of the digits and produce both branches that supply the matrix and the proximal nail fold and arches that supply the matrix and the nail bed. The nail matrix, therefore, has two different sources of blood supply. The nail bed is richly supplied (10–20 cm2) by encapsulated neurovascular structures containing one to four arteriovenous anastomoses and nerve endings. These glomus bodies are arteriovenous shunts involved in the regulation of the blood supply to the digits related to thermoregulation. The cutaneous sensory nerves, which originate from the dorsal branches of the paired digital nerves, run parallel to the digital vessels.
(See Fig. 89-1B)
The nail plate, like hair, consists mainly of low-sulfur filamentous proteins (keratins) embedded in an amorphous matrix composed of high-sulfur proteins rich in cysteine. Other nail constituents include water, lipids, and trace elements. Nail keratins consist of 80%–90% hard hair-type keratins and 10%–20% soft skin-type keratins. Hard keratins have been identified as the acidic 44K/46K and basic 56K/60K keratins. Soft keratins have been identified as the 50K/58K and 48K/56K keratin pairs.24 Keratin filaments have a transverse orientation that is parallel to the nail surface. This explains why the nail plate is more susceptible to transverse fractures than to longitudinal fractures. Specific keratins are expressed only in some compartments of the nail unit; for instance, K6a and K6b, K16, and K17 are not expressed in the nail matrix.13,25,26 Mutations of the genes encoding for these keratins are associated with nail thickening due to nail bed hyperproliferation, as is seen in pachyonychia congenita (PC).27,28 Nail keratin content and composition, measured as the quantity of carbon (C), nitrogen (N), and sulfur (S) in the fingernails, vary between sexes and in relation to the aging process. Sulfur content is higher in female than in male nails and the opposite is for nitrogen. Carbon content is equal in the two sexes. The carbon content increases with aging, possibly due to loss of inorganic material, and the nitrogen content decreases, while the sulfur content remains stable.29
Under normal conditions, the water content of the nail plate is 18%, and most of the water is in the intermediate nail plate.30 The average water content of the nail plate is significantly lower in winter than in summer.31 and varies significantly in time, due to the high porosity of the nail plate, which allows it to be rapidly hydrated and dehydrated. Dehydration is faster when the nails are kept long. When the water content decreases below 18%, the nail becomes brittle; when it increases above 30%, it becomes opaque and soft.32
The nail contains less than 5% lipids, mainly cholesterol; the nail plate lipid content is under hormonal control and decreases after menopause.33 The nail plate also contains traces of several inorganic elements, particularly iron, zinc, and calcium. However, these do not contribute to nail hardness.
The nail plate is hard, strong, and flexible. The hardness and strength of the nail plate are due to its high content of hard keratins and cysteine-rich high-sulfur proteins, whereas its flexibility depends on its water content and increases with nail plate hydration.34,35
The double curvature of the nail plate along its longitudinal and transverse axes enhances nail plate resistance to mechanical stress.36
The physical properties of the nail also depend on the arrangement and adhesion of onychocytes in the different portions of the nail plate, as well as on the orientation of the keratin filaments within the nail plate onychocytes.36 At the ultrastructural level, the corneocytes of the dorsal nail plate are flat, with their shorter diameter perpendicular to the nail plate surface. The average sizes of these cells are 34 μm in length, 64 μm in width, and 2.2 μm in height.37 Cell adhesion is strong. This portion of the nail is responsible for nail plate hardness and sharpness. The onychocytes of the intermediate nail plate show multiple interdigitations of their cell membranes. The average dimensions of these cells are 40 μm in length, 53 μm in width, and 5.5 μm in height. Cell adhesion is provided by desmosomes. This part of the nail plate is responsible for nail pliability and elasticity. The ventral nail plate is thin and consists of soft keratins. It provides adhesion to the underlying nail bed.
The nail plate grows continuously in a proximal to distal manner throughout life. The nail plate is “pushed” out by two factors: (1) matrix keratinocytes proliferation and differentiation which makes a new plate, (2) the nail bed which moves slowly, parallel to the direction of the nail growth, toward the inferior border of the nail plate.3
Fingernails grow two times faster than toenails, with a mean growth rate in adults of 3.5 mm/month for fingernails and 1.5 mm/month for toenails. The 5th fingernail growth rate is significantly slower than other fingernails and the growth rate of the great toenail significantly faster than other toenails.38
Complete replacement of a fingernail requires 100–180 days (6 months). When the nail plate is extracted, it is approximately 40 days before the new fingernail first emerges from the proximal nail fold. After a further 120 days it will reach the fingertip.39 The total regeneration time for a toenail is 12–18 months. As a consequence of the slow nail growth rate, diseases of the nail matrix only become evident a considerable time after their onset and require a long time to disappear after treatment.
Nail growth rate varies among different individuals and among the different digits of the same individual. It depends on the turnover rate of the nail matrix cells and is influenced by several physiologic and pathologic conditions. Nail growth rate is slow at birth, increases slightly during childhood, and usually reaches its maximum between the second and the third decades of life. It sharply decreases after the age of 50 years.39
Conditions that have been associated with a slow growth rate include systemic illness, malnutrition, peripheral vascular or neurologic diseases, and treatment with antimitotic drugs. Nails affected by onychomycosis frequently exhibit a slow growth rate. An arrest of nail growth is a typical feature of yellow nail syndrome. Conditions that have been associated with accelerated nail growth include pregnancy, finger trauma, psoriasis, and treatment with oral retinoids or itraconazole. Accelerated nail growth may cause longitudinal ridging of the nail plate (nail beading).
Due to their slow growth rate, the nails may provide information on pathologic conditions that have occurred up to several months before the time of observation. Drugs, chemicals, and biologic substances accumulate in nails, where they can be detected and measured. Advantages of analyzing nail samples include the ease and noninvasiveness of their collection, the small sample size required for analysis, and the ease of storage at room temperature. The nail of the big toe is the best site for investigation because of its size (big toenail length of an adult: 20 mm) and slow growth rate (about 2 mm/month) permitting to obtain data on exposure to drugs and chemicals over a period of 10 months.40
Nail Signs as a Function of the Site of Pathology
Proximal Matrix | Beau’s Lines Pitting Longitudinal striations Longitudinal fissures Longitudinal grooves Trachyonychia |
Distal matrix | True leukonychia |
Proximal and distal matrix | Koilonychia Onychomadesis |
Nail bed | Longitudinal erythronychia Onycholysis Splinter hemorrhages Apparent leukonychia |
Nail bed and hyponychium | Subungual hyperkeratosis |
Proximal nail fold | Paronychia Periungual erythema |
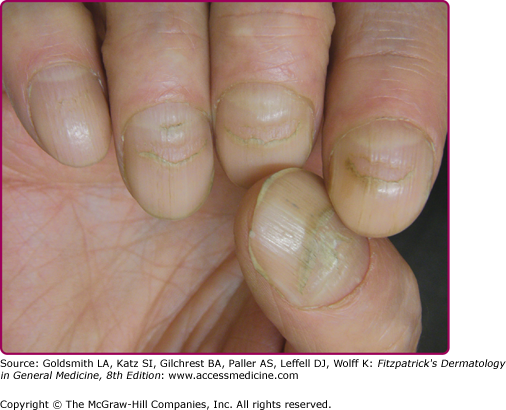
Beau’s lines result from a temporary arrest of proximal nail matrix proliferation and appear as transverse grooves, often deeper in the central nail plate, that move distally with nail growth. Onychomadesis also results from a temporary arrest in nail matrix activity, and the proximal nail plate is detached from the proximal nail fold by a whole-thickness sulcus. Causes of onychomadesis are the same as those for Beau’s lines but are more severe (Box 89-1). Multiple Beau’s lines or onychomadesis in the same nail indicates repetitive insults. Measuring the distance of the groove from the proximal nail fold can date the time of the insult leading to Beau’s lines. Local trauma, such as from manicures or onychotillomania, or related to local cutaneous disease, particularly dermatitis, periungual erythema, and paronychia, are causes of Beau’s lines. Beau’s lines or onychomadesis at the same levels in several nails suggest a systemic cause (Fig. 89-3). Most common among these are drugs (especially chemotherapy), high fever, viral illness,41,42 surgery, and peripheral ischemia. Onychomadesis in children often relates to recent coxsackievirus infection (hand-foot-mouth disease).41,43
|
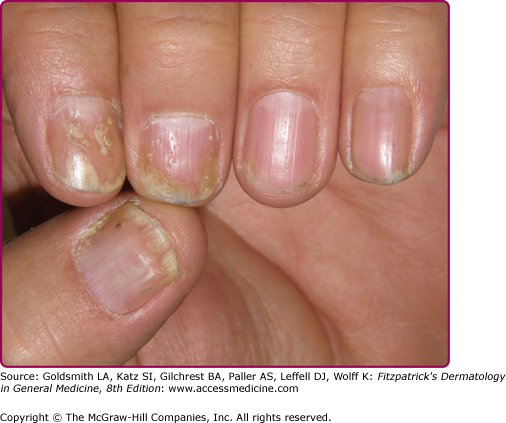
Pits result from small areas of abnormal keratinization of the proximal nail matrix that produce foci of parakeratotic cells in the superficial nail plate. They appear as small punctate depressions of the superficial nail plate, which progress distally and often become more evident with nail growth. Deep and irregularly distributed pits are seen in psoriasis (Fig. 89-4) and atopic dermatitis; geometric and superficial pits are typical of alopecia areata (see Chapters 14, 18, and 88).
Onychorrhexis results from diffuse defective keratinization of the proximal nail matrix. The nail plate is usually thinned and presents multiple longitudinal ridges and fissures. Onychorrhexis is a sign of severe nail fragility and typical of lichen planus (see Chapter 26).
Longitudinal grooves are usually single and appear as a longitudinal depression of the nail plate (1–2 mm large) due to compression of the nail matrix by tumors of the proximal nail fold.
Trachyonychia results from multiple foci of defective keratinization of the proximal nail matrix. The nails are rough due to excessive longitudinal ridging.
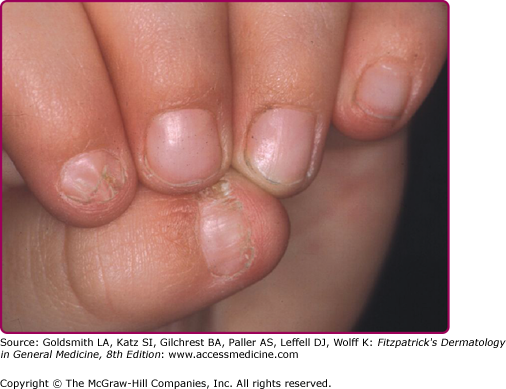
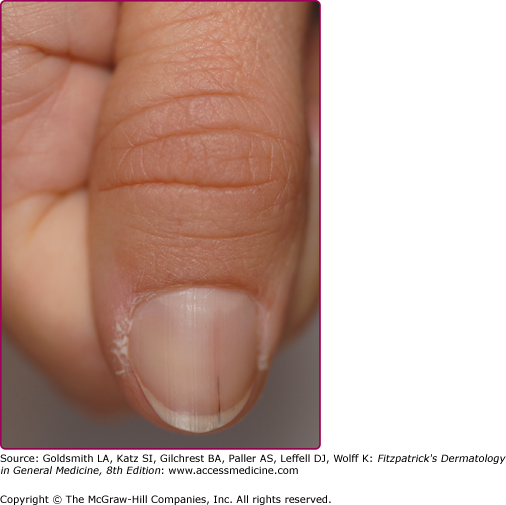
True leukonychia results from defective keratinization of the distal matrix with persistence of parakeratotic cells in the ventral nail plate. The superficial nail plate is structurally normal, but the nail presents opaque white patches or striae, which often disappear before reaching the distal edge of the nail. Punctate leukonychia is due to microtrauma and is typically seen in the fingernails of children (Fig. 89-5). Striate leukonychia of fingernails is a consequence of aggressive manicure. Total or subtotal leukonychia is rare and usually hereditary.

In koilonychia the nail plate is thin and spoon shaped. Koilonychia is physiologic in the toenails of children. In adults it can be a sign of iron deficiency or occupational damage to the nail plate.
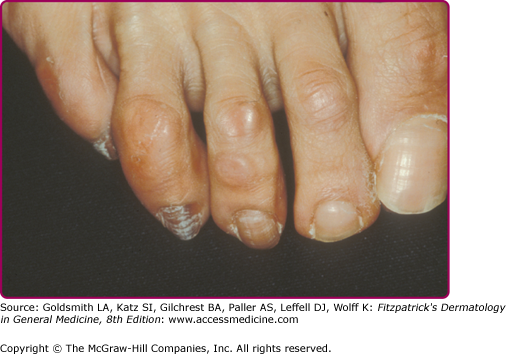
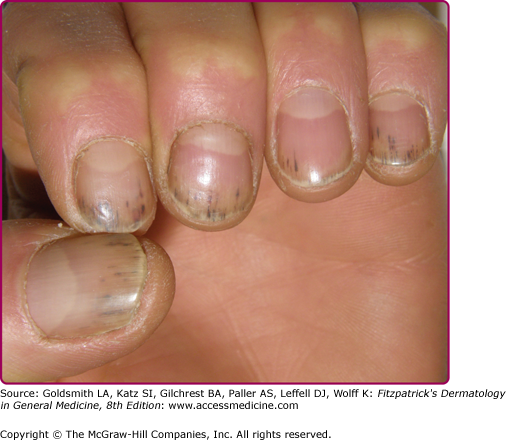
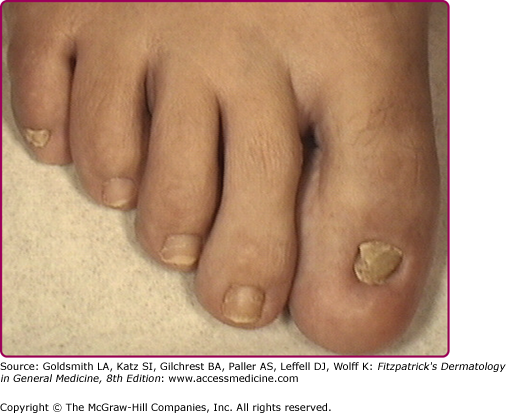
Melanonychia describes a brown to black color of the nail due to the presence of melanin in the nail plate. It can be caused by activation or proliferation (benign or malignant) of nail matrix melanocytes. The pigmentation may involve the whole nail (total melanonychia) or may be banded, as in transverse melanonychia (rare) or in the most common longitudinal melanonychia (LM). LM may appear as a single band involving one digit, or as multiple bands affecting several digits, which are usually due to melanocyte activation, as is seen in dark-skinned individuals, pregnant women, inflammatory nail disorders, individuals with Laugier–Hunziker syndrome, and those taking certain medications (Box 89-2). LM has also been described in individuals with a variety of systemic disorders, particularly human immunodeficiency virus infection and Addison syndrome. In Laugier–Hunziker syndrome, melanonychia begins during adolescence, affects several digits, and is associated with the presence of lip and/or genital pigmented macules45,46 (see Chapter 78). Melanonychia due to melanocyte activation may in some cases involve a single digit, as in patients with onychotillomania, with frictional melanonychia of the 4th or 5th toenails (Fig. 89-6), with inflammatory nail diseases, such as psoriasis or lichen planus, or with nail tumors, such as Bowen’s disease. A single band of melanonychia deserves a careful evaluation, since it may be a sign of a nail matrix nevus or melanoma (see Chapters 122 and 124). LM of a single nail often deserves biopsy.
Longitudinal erythronychia reflects a nail bed disorder and appears as a pink–red longitudinal band of various width extending from the proximal nail to the distal edge. A single band of longitudinal erythronychia is most commonly caused by an onychopapilloma or by another benign or malignant subungual tumor (Fig. 89-7). Multiple bands of longitudinal erythronychia are seen in lichen planus. In Darier’s disease bands of longitudinal erythronychia alternate with white longitudinal bands and V-shaped indentations of the nail-free margin (see Chapter 51).
Onycholysis is detachment of the nail plate from the nail bed and can be caused by traumatic, inflammatory, infectious, or neoplastic nail bed disorders. See Section “Onycholysis under Environmental Nail Disorders.”
Splinter hemorrhages appear as red to black small thin longitudinal lines under the nail plate. They are more commonly located in the distal nail plate and represent rupture of the longitudinally oriented nail bed capillaries (Fig. 89-8). Causes include trauma and inflammatory nail disorders, such as psoriasis.
In apparent leukonychia the nails are pale white due to nail bed discoloration that fades with pressure.
Subungual hyperkeratosis is due to inflammatory disorders that cause an abnormal keratinization of the distal nail bed and hyponychium with accumulation of scales under the distal nail plate. The most common causes include psoriasis, onychomycosis, trauma, contact and atopic dermatitis (see Chapters 13, 14, and 18).
Paronychia is inflammation of the proximal nail fold and presents as painful periungual erythema, sometimes with associated purulence. Acute paronychia is usually caused by infection (see Section “Infectious Nail Disorders”). Chronic paronychia is most commonly due to mechanical or chemical factors. If the periungual area is fluctuant or shows purulence, it should be drained to avoid matrix damage. Topical and/or systemic antibiotics should be administered if bacterial infection is suspected.
Nail pigmentation is most commonly due to exogenous staining of the nail plate. In this case the proximal margin of the pigmentation follows the shape of the proximal nail fold. Exogenous nail pigmentation is most commonly due to occupational exposures or nail cosmetics. Nail pigmentation due to endogenous causes is rare. The proximal margin of the pigmentation follows the shape of the lunula. Possible causes include drugs, argyria, hemochromatosis, alkaptonuria, and Wilson disease.
Hereditary and Congenital Nail Disorders
Ectodermal Dysplasias | Atrophy/Thickening |
Epidermolysis bullosa | Partial or total anonychia Pachyonychia Subungual/periungual hemorrhagic blisters Periungual erosions with granulation tissue |
Pachyonychia congenita | Onychogryphosis Severe thickening Yellow–brown discoloration |
Iso-Kikuchi syndrome | Micronychia/anonychia Hemionychogryphosis |
Nail patella syndrome | Hypoplasia/aplasia Triangular lunulae |
Congenital malalignment of the hallux | Lateral deviation of the nail plate Lateral/distal embedding of nail Nail thickening Yellow–brown discoloration Transverse ridging |
(See Chapter 142)
Nail changes may be associated with hypotrichosis, hypodontia, and hypohidrosis. Most commonly the nails are short, thickened, and hypoplastic.
(See Chapter 62)
Nail abnormalities are a common feature in most subtypes of epidermolysis bullosa (EB) and have recently been included among the criteria for scoring EB severity.49 Trauma undoubtedly contributes to the development of nail dystrophy and for this reason the great toenails are more often severely affected. Pachyonychia of the toenails be the first or the only symptom of dominant dystrophic EB (DDEB) in some families (eFig. 89-8.1). Junctional and dermolytic EB may produce anonychia.50
(See Chapter 50)
PC is an autosomal dominant genodermatosis characterized by painful keratoderma, nail thickening, oral leukokeratosis, and epidermal cysts. The severity of PC can vary greatly among patients and the most problematic aspect of PC, the painful palmoplantar keratoderma (PPK), have vary in extent from focal to a severe, diffuse PPK.51 The International Pachyonychia Congenita Research Registry (IPCRR) has compared the PC phenotype with genotype in hundreds of individuals, and have found issues with the classical division into PC1 (Jadassohn-Lewandowski type) and PC2 (Jackson-Lawler). A new molecular classification has been proposed, in which subtypes of PC refer to the mutated keratin gene.52 Mutations in KRT6A account for almost 50% of known cases, while 24% have mutations are in KRT16, 23% in KRT17, and 3% in KRT6B.53 In contrast to the old classification, in which PC1 was thought to result from mutations in KRT6a or 16, and PC2 from mutations in KRT6b or 17, the clinical features of the former subtypes overlap. For example, cysts (a feature of PC2 and not PC1) most commonly occur in individuals with either a KRT17 mutation or KRT6a mutation.
Nail abnormalities are a constant feature and develop during infancy to early childhood, although a late-onset variety of PC has been described.54 In typical cases the 20 nails are thickened, very difficult to trim, darkened, and with an increased transverse curvature. Nail thickening is a consequence of nail bed hyperkeratosis and is more evident on the distal half of the nails, which have an upward angling. Recent evidence indicates that PC may also present with very subtle nail changes and that there is not a good correlation between mutations detected at molecular level and clinical phenotype. Severity may even vary among family members with the same gene mutation.55,56
Nail abnormalities in nail patella syndrome may involve all fingernails or may be limited to the thumbs, which are always the most severely affected digits (Fig. 89-9). Nail hypoplasia is usually more marked in the medial portion of the nail. The shape of the lunula is typically triangular.48