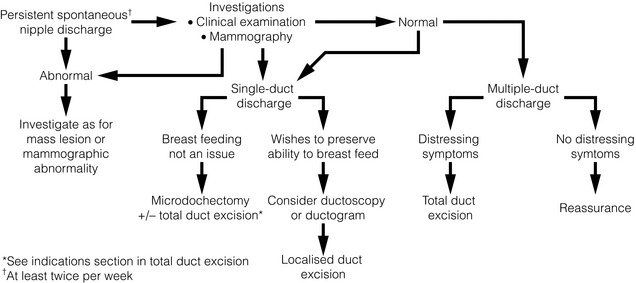
17 Over 90% of patients presenting to a breast clinic have normal breasts or benign breast disease.1 An understanding of the aetiology, symptoms and management will ensure correct treatment and patient satisfaction. The expectation that the breast surgeon’s role is simply to diagnose or exclude breast cancer has long disappeared. Benign breast disease causes considerable morbidity and anxiety, and with increasing patient awareness and expectations, the number of such patients attending clinics is increasing. Effective treatment includes accurate diagnosis followed by adequate explanation of the condition, provision of relevant information related to the diagnosis and how it is best managed. This is a rewarding part of a breast specialist’s workload. Accessory breast tissue tends to become more prominent or obvious during pregnancy (Fig. 17.1). Reassurance and an explanation of the cause of the ‘lump’ are usually all that is required. Surgical excision should be reserved for those truly symptomatic, as they are difficult to excise cosmetically and surgery is associated with significant morbidity.2 Liposuction during excision helps define the planes between the accessory breast and the fascia of the axilla. As with normal breast tissue, both benign and malignant conditions can develop within accessory breast tissue.3 This is failure of one or both (rarely) breasts to develop fully and can be congenital or acquired. Genetic causes include Poland’s syndrome and ulnar–mammary syndrome. Poland’s syndrome is a group of conditions associated with the absence of hypoplasia of the pectoralis major muscle, the chest wall and varying degrees of syndactyly.4 It is rare and usually only partial in nature. It is more common in men than in women. Acquired abnormalities in breast development can be caused by iatrogenic trauma or radiotherapy. Treatment of hypoplasia and Poland’s syndrome depends on the degree of deformity. Mild asymmetry is a common problem and usually only reassurance is needed. If the asymmetry is marked, augmentation of the smaller breast with or without tissue expansion and/or reduction or augmentation of the opposite breast may be required (Fig. 17.2). Tissue expansion is often required as there are differing amounts of skin on the two breasts. A pedicled or free myocutaneous flap, with or without an implant, can be used to reconstruct any muscle defect and produce symmetry in cases of severe hypoplasia or aplasia. Fat transfer (lipofilling) has also been described as a technique to correct or aid correction of breast hypoplasia either alone or combined with a breast implant.5,6 Hypoplasia can also be associated with tubular or tuberous breasts. This deformity can affect one or both breasts and the breast shape is caused by a constricting ring at the base of the breast, limiting vertical and horizontal growth. The surgical management of this group of conditions is challenging and often unsatisfactory. Tissue expansion combined with radial incisions on the deep aspect of the breast to divide the constricting ring usually improves contour. The large nipple–areola complex may need to be reduced in size. Lipofilling is being used increasingly in such patients.6 Macromastia is the excessive development of the breasts. This tends to occur during puberty (juvenile hypertrophy) or with onset of lactation (gestational). Prepubertal breast enlargement may occur very rarely in conjunction with a hormone-secreting tumour. Juvenile hypertrophy results from excessive proliferation of ducts and stromal tissue but no lobule formation. Significant psychological and physical problems can be caused by macromastia and patients with significant breast enlargement benefit from breast reduction. This procedure is not without complications and should be performed by an appropriately trained surgeon.7 Defining what represents breast disease and what is normal is not a new problem. The ANDI classification8 was developed to provide a framework to help understanding of the pathogenesis and subsequent management of benign breast disease. Most benign diseases arise from normal physiological processes and range from normality to mild abnormality (aberration) to severe abnormality (disease). The breast passes through phases related to the levels of circulating hormones and their effects on the ducts, lobule and stroma. The phases are breast development, cyclical change and involution (Table 17.1). Table 17.1 Aberrations of normal breast development and involution A fibroadenoma is classified as an aberration of normal breast development and is made up of a combination of connective tissue and proliferatory epithelium (Fig. 17.3).9 It is not a neoplasm or benign tumour as it does not arise from a single cell. Fibroadenomas arise from the hormone-dependent terminal duct lobular unit and are influenced by hormones, e.g. increasing in size during pregnancy. The stromal element of these tumours defines their classification and behaviour. A ‘simple’ fibroadenoma contains stroma of low cellularity and regular cytology. Phyllodes tumours may or may not arise from fibroadenomas but contain stroma with much more marked cellularity and atypia. Although phyllodes tumours cannot always be differentiated on core biopsy with 100% certainty from fibroadenomas, it is usually possible to tell whether phyllodes is likely and when the lesion is a simple fibroadenoma. All discrete masses over the age of 23 should have a core biopsy – multiple passes with three samples of the lesion. Although ultrasound can usually differentiate fibroadenomas from cancers and guidelines indicate ultrasound is safe under 25, experience from medicolegal practice indicates the cut-off should be younger at 24 or below. Fibroadenomas were observed for 2 years in women under 40 years of age: the majority did not change in size (55%), some got smaller or resolved (37%) and only a small number increased in size (8%), the majority of which were in women under the age of 20.10 In older women (> 23 years of age) it is clearly essential to differentiate a fibroadenoma from breast cancer by triple assessment including core biopsy. Rapid growth of a fibroadenoma is rare but can occur in either adolescence (juvenile fibroadenoma) or in the perimenopausal age group (Fig. 17.4). Tumours over 5 cm are termed ‘giant fibroadenoma’ and are seen more commonly in African countries.11 On macroscopic appearance fibroadenomas are discrete, bosselated, whitish tumours that appear to bulge when cut through. Only rarely does cancer develop within a fibroadenoma but when it does it tends to be non-invasive and lobular in nature.12 Management: The management of fibroadenomas depends on the patients’ age and preference as well as the results of triple assessment. Core biopsy (multiple cores) is now preferred to cytology to confirm the diagnosis of a fibroadenoma. In patients with lesions under 4 cm, where histology confirms the diagnosis, the patient can then be reassured and discharged. In women presenting with multiple clinical and radiological fibroadenomata, core biopsy should be undertaken of the largest lesions – either one from both breasts or two from the same breast. Excision should be performed through a cosmetically placed incision, which includes a submammary, axillary and circumareolar incision. Another option is to remove fibroadenomas with a mammotome.13 With larger lesions (> 5 cm where histology has shown no suggestion that it could be a phyllodes tumour), it is safe to section the tumour in situ and remove it through a small incision below the breast to improve cosmetic outcome. Large lesions are best be removed cosmetically through an inframammary incision. Removal of excess skin is rarely required in young women, particularly when removing a large juvenile fibroadenoma (Fig. 17.4). In some very large lesions later revisional surgery is required but it is important to leave this for up to a year after the initial excision as skin retracts and the breast reshapes itself over this period. Recurrence of a fibroadenoma can occasionally occur but is rare and it may be due to undiagnosed adjacent lesions rather than incomplete excision. The aetiology of phyllodes (leaf-like) tumours is unknown. They are less common than fibroadenomas (ratio of presentation 1:4014) and constitute about 2.5% of all fibroepithelial tumours. The age of onset is 15–20 years later than fibroadenomas. They can grow rapidly, sometimes producing marked distortion and cutaneous venous engorgement, which occasionally can lead to ulceration. The majority are benign in nature and feel like large fibroadenomas, and are diagnosed only following core biopsy. They are rarely fixed to skin or muscle. When cut during removal they are more brownish in colour than fibroadenomas and can have areas of necrosis within. Most diagnoses of phyllodes tumour are made before operation, on core biopsy, and the aim of surgery should be to remove the lesion with a clear macroscopic margin. Overall, phyllodes tumours recur locally in approximately 20% of patients. Most locally recurrent tumours are histologically similar to the original lesions but occasionally benign phyllodes recur as borderline lesions. Malignant phyllodes tumours recur earlier on average than benign lesions. For benign lesions, total excision with clear margins (≥ 1 mm) is sufficient.15 For borderline and malignant lesions a wider margin is recommended and this may necessitate mastectomy with or without a myocutaneous flap for skin cover or breast reconstruction in large lesions. Regional lymph node metastases are seen rarely in malignant phyllodes tumours, with nodes being affected in approximately 5%. Metastatic spread, when it occurs, is similar in pattern to that of sarcomas. Fewer than 5% of all phyllodes tumours metastasise and approximately 25% of those classified as malignant metastasise, depending on the exact criteria used for classification. Treatment of metastatic disease is discouraging, with no sustained remissions reported from radiation, hormonal treatment or chemotherapy. Nipple discharge accounts for 5% of referrals to a breast clinic,16 with up to 20% of these caused by in situ or malignant disease.17 The important features to assess are whether the discharge is from a single or multiple ducts, is coloured or bloodstained, is induced or spontaneous, and is affecting one or both breasts. The frequency, colour and consistency of the discharge should be noted. Blood-coloured discharge or discharge that contains significant amounts of blood on testing has been reported by some but not all authors to be more likely to arise from a cancer than coloured discharge that contains no blood on testing.18 The sensitivity and specificity of blood in the discharge is, however, not high. Persistent discharge (≥ 2 per week) is also more likely to be associated with a significant causative lesion (such as a papilloma or cancer). The aim is to differentiate between physiological causes and ductal pathology (Fig. 17.5). Discharge can be elicited by squeezing around the nipple in 20% of women19 and is often noted following mammography. If discharge is associated with a lump, then management is directed to the diagnosis of the lump. Figure 17.5 Multiduct physiological discharge. Note the range of colours characteristic of physiological discharge. Assessment includes a careful breast examination to identify the presence or absence of a breast mass. Firm pressure applied around the areola can help to identify the site of any dilated duct (pressure over a dilated duct will produce the discharge); this is helpful in defining where an incision should be made for any subsequent surgery. The nipple is squeezed with firm digital pressure and if fluid is expressed, the site and character of the discharge are recorded. Testing of the discharge for haemoglobin determines whether blood is present but this is of limited value, although bloodstained discharge is more likely to be associated with malignancy. Fewer than 20% of patients who have a bloodstained discharge or who have a discharge containing moderate or large amounts of blood have an underlying malignancy. Age is said to be an important predictor of malignancy; in one series, 3% of patients younger than 40, 10% of patients between ages 40 and 60, and 32% of patients older than 60 years who presented with nipple discharge as their only symptom were found to have cancers.20 The absence of blood in nipple discharge is not an absolute indication that the discharge is unrelated to an underlying malignancy, as demonstrated in a series of 108 patients where the sensitivity of haemoccult testing was only 50%. Nipple discharge cytology is of little use due to its poor sensitivity.21,22 A number of techniques have evolved to determine the aetiology and avoid unnecessary surgery. Ductoscopy, using a microendoscope passed into the offending duct, allows direct visualisation. There are encouraging reports of its use (see Chapter 3), especially in directing duct excision at surgery23 and detecting deeper lesions that may be missed by blind central excision.24 Ductal lavage is a technique in which the duct is cannulated, irrigated with saline and the subsequent discharge examined cytologically. This technique increases cell yield by 100 times that of simple discharge cytology.25 Ductography (imaging of the ductal system) can identify intraductal lesions. Although this investigation has only a 60% sensitivity for malignancy, a filling defect or duct cut-off has a high positive predictive value for the presence of either a papilloma or a carcinoma.26,27 Ductography, however, is a painful procedure and is not widely practised. At present, the major role of ductoscopy is as an adjunct to surgery; by using simple transillumination of the skin overlying the lesion during ductoscopy, limited duct excision is possible. The role of ductal lavage has been questioned due to large variations in its sensitivity and specificity.28,29 During ductoscopy, visualised lesions can be biopsied and in one report 38 of 46 women with biopsy-proven papillomas were observed for 2 years with no reported missed cancers.24 The role of ductoscopy in the assessment of nipple discharge is set to increase as the quality of equipment improves and it becomes more widely available. A benefit of both ductography and ductoscopy is that they allow identification of the site of any lesion in younger women, allowing localisation and excision of the causative lesion while retaining the ability to lactate (Fig. 17.6). A mammogram should be performed as part of the assessment of patients over 35 years of age with a discharge. The sensitivity in this group of patients is low, at 57%.21 Digital mammography has been shown to have a greater pick-up rate than film mammography in women under 50 or with dense breasts.30 Ultrasound can sometimes identify papillomas and malignant lesions in the ducts close to the nipple.31 Papillomas visualised on ultrasound can then be biopsied or removed using a vacuum-assisted core biopsy device.32 If no abnormality is found on clinical or mammographic examination, patients are managed according to whether the discharge is from a single duct or multiple ducts (Fig. 17.6). Any patient with spontaneous single-duct discharge should undergo surgery to determine the cause of the discharge if it is: Duct ectasia: This is benign dilatation and shortening of the terminal ducts within 3 cm of the nipple. It is a common condition and increases in incidence with age. It should not be confused with periductal mastitis, which occurs in younger women and is secondary to cigarette smoking. Duct ectasia can present as nipple discharge, nipple retraction (giving a slit-like appearance) or a palpable mass. It is usually asymptomatic. The discharge is usually creamy and cheesy in nature. Bilateral multiduct green discharge is physiological and not related to duct ectasia. Ductal papillomas: There are three main forms: a solitary-duct discrete papilloma, multiple papillomas or juvenile papillomatosis (Swiss cheese disease). Papillomas are characterised by formation of epithelial fronds that have both the luminal epithelial and the outer myoepithelial cell layers, supported by a fibrovascular stroma. The epithelial component can be subject to a spectrum of morphological changes ranging from metaplasia to hyperplasia, atypical hyperplasia and in situ carcinoma. A solitary intraductal papilloma, which occurs in a large duct (within 5 cm of the nipple), is the commonest form and is the most common aetiology of a bloody nipple discharge. They are most frequently seen in the 30–50 age group and can be palpated in one-third of patients. As papillomas have a thin stalk, they have the potential to tort and necrose. Half of women with papillomas have bloody discharge while the other half have a serous discharge.33 Ductal carcinoma in situ: Bloody nipple discharge with or without the presence of Paget’s disease constitutes one-third of all symptomatic in situ patients.34 Only rarely does an invasive cancer cause nipple discharge in the absence of a clinical mass. In most series, ductal carcinoma in situ (DCIS) is responsible for less than 20% of unilateral single-duct nipple discharge.19 The diagnosis is often made only following surgical excision of the affected duct. Bloody nipple discharge in pregnancy: Bilateral bloody nipple discharge detected either visibly or on testing during pregnancy or lactation is common. In 20% of women who develop nipple discharge during pregnancy, blood is evident on testing. The likely cause is hypervascularity of developing breast tissue; provided that the discharge is multiductal and/or bilateral it is benign, resolves spontaneously and requires no specific treatment.35 Nipple adenoma: Nipple adenomas present as a non-discrete, palpable growth of the papilla of the nipple (see Fig. 17.7). There may be nipple discoloration and contour change noted. Nipple adenomas tend to cause erosion of the nipple tip and commonly present as a bloody discharge from the surface of the nipple. They are benign in nature and definitive treatment is complete excision. It is caused by ductal hyperplasia of the lactiferous ducts and is seen most commonly in women of between 40 and 50 years of age. Microdochectomy: A single duct can be removed by microdochectomy. This is performed through either a radial incision or preferably a circumareolar incision. Expression of the discharge should not be performed until the patient is in theatre and fully draped in order to provide the best chance of identifying the offending duct. The discharging duct is cannulated and either a lacrimal probe placed or methylene blue injected and an incision made. The probe aids identification of the relevant duct and dissection of this from surrounding ducts/breast tissue. A length of at least 2–3 cm should be removed. The excised duct should be opened to ensure a cause for the discharge is present and the distal remnant inspected to ensure that the entire dilated duct has been excised. If the residual duct is dilated, then it should be split, opened and inspected. Microdochectomy should not damage surrounding normal ducts and allows subsequent breastfeeding. If performing a duct excision directed by ductoscopy, then having identified an abnormality in the duct, the light is used to direct the surgical excision. Once the excision has been performed, the nipple should be squeezed gently to ensure that the discharging duct has been excised. Total duct excision or division: In women of non-childbearing age, total duct excision is an option for a single-duct discharge. Current evidence suggests that total duct excision is more likely to result in a specific diagnosis and less likely to miss underlying malignancy than microdochectomy.36 Total duct excision can also be used for multiple-duct discharge if the discharge is copious and affecting quality of life, and is often performed for periductal mastitis. The operation involves dividing all the ducts from the underside of the nipple and removing surrounding breast tissue to a depth of 2 cm behind the nipple–areola complex.37 A circumareolar incision is used. Patients should be warned that there is a small risk of nipple tip necrosis (< 1%), reduced sensation (40%) and nipple inversion associated with this operation. Patients undergoing surgery for periductal mastitis require total removal of all ducts from behind the nipple; leaving even small remnants of ducts predisposes to recurrence. Because the lesions of periductal mastitis usually contain organisms, patients should receive appropriate systemic antibiotic treatment during the operation and for 5 days after surgery. Options for antibiotic therapy include amoxicillin–clavulanate or a combination of erythromycin and metronidazole. Due to the hormonal aetiology, true breast pain is often worse before and relieved after menstruation. Exacerbating factors include the perimenopausal state (where hormone levels fluctuate) and the use of exogenous hormones (hormone replacement therapy or the oral contraceptive pill). The cause of cyclical mastalgia is unknown but studies have implicated excess production of prolactin,38 excess oestrogen,39 insufficient progesterone,40 or increased receptor sensitivity in breast tissue caused by a raised ratio of saturated fatty acids to essential fatty acids.41 A full history and examination should be performed. The patient should be rolled and the underlying chest wall – often the site of the pain – palpated. In women over 40 years of age, mammography should be performed to exclude an occult malignancy (approximately 5% of women with breast cancer complain of pain,14 while 2.7% of women presenting with pain as their main symptom are diagnosed with breast cancer42). If a dominant lump or lumpiness is palpable, then this will dictate further management. Most breast pain, and this includes many women with cyclical breast pain, arises in the chest wall. Analgesia, a firm bra worn 24 hours a day and gentle stretching exercises such as swimming are effective treatments. Reassurance that the symptoms are not related to an underlying malignancy is the most effective treatment for mastalgia.43 Following this, the majority will require no further treatment. Evening primrose oil (EPO) is not effective, as two double-blind, randomised, crossover trials comparing EPO versus placebo showed no benefit for EPO.44,45 The original work that advocated its use has never been published other than in abstract form.46 Other agents that have been shown to have some benefit include phyto-oestrogens (e.g. soya milk)47 and Agnus castus (a fruit extract).48 Reducing fat intake to less than 15% of dietary calories has been shown to improve symptoms in cyclical mastalgia.49 The patients who responded showed changes in their serum lipid profiles but the study was not blinded so placebo effects cannot be excluded and the diet is not easy to adhere to in the long term. In severe pain, medication can be used but complications of these treatments need to be outlined to the patient. Treatment should be either tamoxifen 10 mg daily or danazol. Tamoxifen 20 mg daily was superior to placebo in a double-blind, randomised, controlled trial and pain relief was maintained in 72% of women 1 year after use.50 Tamoxifen restricted to the luteal phase of the menstrual cycle abolished pain in 85% of women. Recurrent pain at 1 year was seen in 25% and the rate of adverse effects was 21%.51 Tamoxifen 10 mg daily has fewer side-effects and is as effective as 20 mg when compared with danazol 200 mg daily.52 Tamoxifen is superior to danazol, with fewer adverse effects: 53% of patients receiving tamoxifen were pain free at 1 year compared with 37% of patients receiving danazol. Tamoxifen 10 mg daily or danazol can be given only during the luteal phase of the menstrual cycle and results in similar improvements in symptoms, but with a marked reduction in adverse effects.51,53 Tamoxifen is not licensed for use in mastalgia. Toremifene, another selective oestrogen receptor modulator, has also recently demonstrated its effectiveness in treating mastalgia. In a randomised, double-blind trial of 195 women with persistent (lasting longer than 6 months) mastalgia, they assigned patients to toremifene 30 mg daily or a matched placebo for three menstrual cycles. This demonstrated a significant benefit for toremifene but with no significant difference in adverse events between the two groups.54 A phase II trial using afimoxifene (4-hydroxytamoxifen) delivered locally to the breast as a transdermal hydroalcoholic gel daily over four cycles has shown statistically significant improvements in signs and symptoms of cyclical mastalgia across patient- and physician-rated scales, with excellent tolerability and safety. There is strong evidence that this tamoxifen metabolite is absorbed into the breast tissue but does not have the systemic effects associated with tamoxifen.55 It is not used in the UK. Bromocriptine should not be used, due to its high rate of adverse effects (80%).56 Selective serotonin reuptake inhibitors have been reported as being of some benefit in mastalgia as part of premenstrual syndrome;57 they also have effects on fatty acid profiles.
Benign breast disease
Introduction
Congenital abnormalities
Supernumerary nipples and accessory breast tissue
Breast hypoplasia
Aberrations of normal breast development and involution
Age (years)
Normal process
Aberration
< 25
Breast development
Stromal
Juvenile hypertrophy
Lobular
Fibroadenoma
25–40
Cyclical activity
Cyclical mastalgia
Cyclical nodularity (diffuse or focal)
35–55
Involution
Lobular
Macrocysts
Stromal
Sclerosing lesions
Ductal
Duct ectasia
Fibroadenomas
Simple fibroadenomas

Phyllodes tumour and sarcoma
Nipple discharge

Investigation
Aetiology
Surgery
Mastalgia
Assessment
Treatment

Related posts:
 Psychosocial issues in breast cancer
Psychosocial issues in breast cancer
 Nipple discharge and the role of ductoscopy in breast diseases
Nipple discharge and the role of ductoscopy in breast diseases
 Techniques of mastectomy: tips and pitfalls
Techniques of mastectomy: tips and pitfalls
![]() The role of adjuvant systemic therapy in patients with operable breast cancer
The role of adjuvant systemic therapy in patients with operable breast cancer
 Breast reconstruction
Breast reconstruction
![]() The genetics of breast cancer, risk-reducing surgery and prevention
The genetics of breast cancer, risk-reducing surgery and prevention
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine