(1)
University of Florida, College of Medicine, Gainesville, FL, USA
(2)
Private Practice:, Orlando, FL, USA
5.1 Benign Epidermal and Dermal Tumors
Common benign growth often seen after 3rd decade of life
Typically light brown to yellow to dark brown papule or plaque with waxy or verrucous appearance and ‘stuck on’ appearance
Histology: hyperkeratosis, papillomatosis and acanthosis of epidermis, horn pseudocysts, often increased melanin in basal layer or throughout entire epidermis
At least five histological variants:
Acanthotic SK: most frequently seen histologic type; smooth dome-shaped papule with slight hyperkeratosis/papillomatosis but significant acanthosis and many invaginated horn pseudocysts, increased amount of melanin within keratinocytes
Hyperkeratotic SK: exophytic lesion with significant hyperkeratosis and papillomatosis, only mild acanthosis, fewer horn pseudocysts
Reticulated (adenoid) SK: interlacing thin strands of basaloid cells and horn pseudocysts
Clonal SK: intraepidermal well-defined nests of basaloid cells with uniform appearance
Irritated SK: squamous eddies (whorls of eosinophilic keratinocytes) within epidermis, ± scattered necrotic keratinocytes, lymphoid infiltrate (lichenoid, perivascular or diffuse)
Pigmented SK (melanoacanthoma): acanthotic, heavily pigmented SK
Treatment: reassurance, cryotherapy, electrodessication, curettage, shave removal

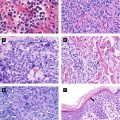
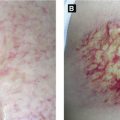
Figure 5.1:
A: Seborrheic keratosisB: Seborrheic keratosisC: Multiple SKs
Sign of Leser-Trelat: sudden eruption of SKs typically on trunk and associated with underlying adenocarcinoma (ie. stomach, colon, etc).
Benign, solitary erythematous papule or plaque most often on the leg
Histology: sharply-demarcated psoriasiform epidermal hyperplasia containing large, pale keratinocytes with + PAS-staining (due to glycogen within cells), exocytosis of neutrophils, ± parakeratotic crust
Common benign fibrohistiocytic tumor often on leg
Presents as pigmented or pink firm dome-shaped papule with central induration, + dimple sign (dimpling of skin with inward compression of lesion)
Histology: poorly-circumscribed nodular proliferation in dermis of spindle-shaped fibroblasts with storiform pattern, hyalinized collagen at periphery of lesion (‘keloidal collagen’) with fibroblasts around collagen (collagen trapping), epidermal hyperplasia ± flattened (‘tabled’) rete ridges, ± basal layer hyperpigmentation
Variants: atrophic DF, cellular DF, xanthomatous DF, hemosiderotic DF

Figure 5.2:
A: Dermatofibroma (Courtesy of Dr. Paul Getz)B: DermatofibromaC: Pearly penile papules
Multiple DFs seen in LE, atopic dermatitis and immunosuppression
Giant Cell Tumor of Tendon Sheath (Figure 5.5B)
Presents as slow-growing firm skin-colored nodule on finger or toe, fixed to underlying tendon sheath or fascia
Histology: well-demarcated lobular collection of cells in dermis with fibroblasts and histiocytes, characteristic multinucleated giant cells (osteoclast-like with haphazard nuclei), hemosiderin
General term for lesions with similar histologic features and includes periungual fibromas, fibrous papules and pearly penile papules
Presents as skin-colored to red solitary dome-shaped papule most often on nose or central face; pearly penile papules present as dome-shaped small papules circumferentially around corona of glans penis
Multiple angiofibromas seen in tuberous sclerosis
Histology: dome-shaped papule with ↑ fibroblasts, collagen oriented concentrically around follicles or perpendicular to epidermis, ↑ dilated blood vessels
Solitary pink or brown keratotic excrescence on finger with surrounding collaretteof elevated skin
May resemble supernumerary digit
Histology: massive orthokeratosis and thick, vertically-oriented collagen bundles in dermis, blood vessels surrounding collagen bundles
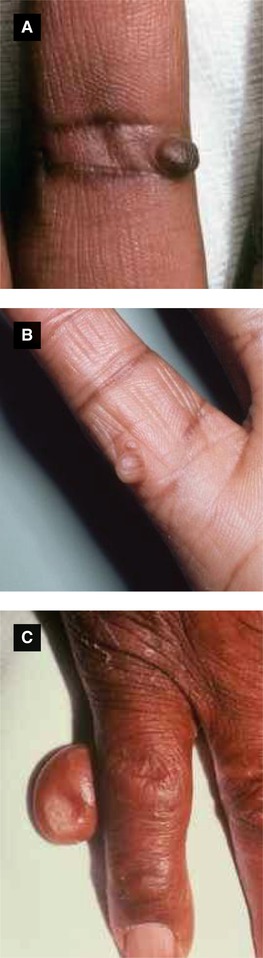
Figure 5.3:
A: Acquired digital fibrokeratoma*B: Supernumerary digit*C: Supernumerary digit**Courtesy of Dr. Paul Getz
Supernumerary digit (Figure 5.3B-C): see ↑ # of nerves (unlike acquired digital fibrokeratoma)
Neurofibroma (NF)
Common benign growth; multiple NFs or plexiform NF associated with neurofibromatosis
Presents typically as solitary, slow-growing skin-colored to pink papule with soft or rubbery feel, ± pedunculated, + ‘buttonhole sign’ (invagination with compression by finger)
Histology: typically unencapsulated somewhat demarcated nodular proliferation in dermis consisting of spindle cells with wavy nuclei, pale ‘bubblegum’ stroma or fibromyxoid stroma, and mast cells
Neuroma
Tumor of neural tissue; two types which include traumatic neuroma (amputation neuroma) and palisaded encapsulated neuroma (PEN)
Often presents as solitary skin-colored to erythematous firm papule, ± associated pain (occurs as site of trauma if traumatic neuroma)
Histology:
Traumatic neuroma: well-circumscribed nodule consisting of fascicles of peripheral nerve arranged in a haphazard pattern
PEN: well-demarcated proliferation of palisading spindle cells with encapsulation and fibrotic stroma
Benign nerve sheath tumor consisting of Schwann cells
Presents as subcutaneous skin-colored papulonodule often on extremity with occasional tenderness or pain
Histology: well-circumscribed, encapsulated deep dermal or subcutaneous tumor consisting of two areas (below), mast cells common
Antoni A tissue: cellular areas consisting of spindle cells with palisaded nuclei arranged in parallel rows with intervening acellular area (Verocay bodies)
Antoni B tissue: hypocellular myxoid areas
Neurothekeoma (Figure 5.5D)
Pink, red or brown papulonodule often involving head; can be soft or firm
Histology: well-demarcated mass in reticular dermis or subcutaneous tissue consisting of myxoid nests or fascicles composed of spindle or epithelioid cells with vesicular nuclei, fascicles divided by fibrous septae
Eccrine Poroma (Figure 5.4A-B)
Presents as erythematous papule, plaque or nodule with surrounding indented ‘moat’, often on palm, sole or scalp
Histology: well-circumscribed tumor appearing in lower part of epidermis and extending into dermis, cells consist of small cuboidal epithelial (‘poroid’) cells which are more pale than normal keratinocytes (may be clear due to glycogen accumulation), small sweat ducts seen within tumor, sharp demarcation between ‘poroid’ cells and surrounding keratinocytes

Figure 5.4:
A: Eccrine poroma, scalp*B: Eccrine poroma, plantar(Courtesy of Dr. Sophie M. Worobec)C: Cylindroma**Courtesy of Dr. Paul Getz
Nodular Hidradenoma (Clear Cell Hidradenoma)
Benign adnexal neoplasm presenting as solitary skin-colored nodule with no site predilection
Histology: well-demarcated nodular proliferation in dermis or subcutaneous tissue consisting of uniform basaloid cells (can have clear cell change), hyalinized collagen in stroma, ± sweat ducts within tumor
Eccrine Spiradenoma (Figure 5.5E)
Presents as erythematous, blue or gray nodule, ± painful
Histology: sharply-delineated basophilic nodule or nodules (‘cannon balls’ or ‘blue balls’) in dermis with two types of cells present (small, dark basaloid cells in rosette pattern and pale large cells)
Presents as single or multiple firm, rubbery nodules with erythematous to blue color, often on scalp
Histology: well-demarcated basaloid proliferation in dermis consisting of discrete lobules of cells arranged in ‘jigsaw’ or mosaic pattern, each lobule with hyalinized cylinders and hyalinized droplets often within tumor
Multiple cylindromas seen with CYLD mutation either in cylindromatosis or in conjunction with other skin appendage tumors in Brooke-Spiegler syndrome

Figure 5.5:
A: Clear cell acanthoma* B: Giant cell tumor of tendon sheath*C: Schwannoma* D: Neurothekeoma*E: Eccrine spiradenoma* F: Cylindroma**Reprint from Baykal C, Yazganoğlu KD (eds). Clinical Atlas of Skin Tumors. Heidelberg, Germany. Springer; 2014.
Trichilemmoma
Neoplasm with differentation toward follicular outer sheath
Presents as solitary or multiple smooth-surfaced or verrucoid papules or nodules on face
Histology: downward lobular growth of epidermis consisting of pale or clear keratinocytes, periphery of lobules with palisading basal keratinocytes and eosinophilic hyaline membrane
Multiple trichilemmomas seen in Cowden disease
Inverted Follicular Keratosis (Figure 5.6A)
Presents as white, tan or pink papule often on face (especially cheek or upper lip)
Histology: endophytic proliferation of pale keratinocytes, ± squamous eddies, ± horn cysts

Figure 5.6:
A: Inverted follicular keratosis*B: Trichoepitheliomas*C: Syringoma***Courtesy of Dr. Paul Getz**Reprint from Baykal C, Yazganoğlu KD (eds). Clinical Atlas of Skin Tumors. Heidelberg, Germany. Springer; 2014.
Trichoepithelioma (Figure 5.6B)
Benign neoplasm with follicular differentiation
Presents as skin-colored papule or nodule with predilection for nose, can be solitary or multiple
Histology: symmetric growth of basaloid tumor islands forming reticulate cords with foci of bulbar differentiation, ± horn cysts
Multiple seen in Brooke-Spiegler syndrome and Rombo syndrome
Desmoplastic Trichoepithelioma
Firm, skin-colored to erythematous annular plaque with central depression typically seen on upper cheek
Histology: thinner cords of basaloid cells arrayed interstitially among dense collagenous stroma, ± horn cysts, ± calcium deposits
Histology resembles sclerosing BCC but benign lesion
Small papules often clustered over eyelids, less often disseminated over trunk
Histology: proliferation in superficial dermis consisting of comma-shaped eccrine ducts (resembling tadpoles), fibrotic stroma, ± horn cysts, ±milia

Figure 5.7:
A: Syringomas(Courtesy of Dr. Paul Getz)B: Cutaneous leiomyomas(Reprint from Bolognia JL, Rapini R, Jorrizo JL. Dermatology. 2nd ed. St. Louis: MO: Mosby; 2008.)C: Actinic keratosis
Hidradenoma Papilliferum
Presents as smooth papule or subcutaneous nodule almost always involving vulva
Histology: circumscribed proliferation in dermis consisting of mazelike glandular spaces lined by tall columnar pale cells and myoepithelial cells, foci of decapitation secretion, no connection to epidermis
Syringocystadenoma Papilliferum
Presents as papule or plaque with papillomatous or crusted surface often on head or neck
Histology: acanthotic epidermis with cystic invaginations containing numerous villous projections lined by two layers of epithelial cells (columnar and small cuboidal), plasma cells in stroma, decapitation secretion
Granular Cell Tumor (Figure 5.11B)
Often solitary, skin-colored to brown-red papulonodule often on head/neck (especially tongue)
Histology: poorly-demarcated nodule in dermis consisting of large, pale cells with granular cytoplasm and centrally located nucleus, intracytoplasmic granules called pustulo-ovoid bodies of Milian, may see striated skeletal muscle if lesion on tongue
Cutaneous Leiomyoma (Figure 5.7B)
Presents as reddish brown, pink or skin-colored papules, ± painful, may be solitary or multiple; often seen during adolescence or early adulthood
Histology: neoplasm composed of bland-appearing myocytes with eosinophilic cytoplasm arranged in intersecting fascicles, cells contain elongated nuclei with ‘cigar-shape’ on longitudinal section; cross-section shows round nuclei and vacuoles
Reed’s syndrome (multiple cutaneous and uterine leiomyomatosis syndrome): multiple cutaneous and uterine leiomyomas, ↑ risk of renal malignancy, mutation in fumarate hydratase
Angiolipoma
Tumor consisting of mature lipocytes and blood vessels
Presents as soft subcutaneous nodules often on forearms of young adults, often with pain
Histology: well-circumscribed neoplasm of mature adipose tissue with a variable number of small vessels, ± fibrin thrombi within vessels, ± mast cells
5.2 Premalignant and Malignant Tumors
Common premalignant lesions in sun-exposed area with potential to transform into squamous cell carcinoma (percentage varies)
Presents as scaly erythematous macule or thin papule in sun-exposed areas (easier to identify with palpation)
Histology: focal parakeratosis, atypical keratinocytes with nuclear pleomorphism and crowding (partial-thickness dysplasia), disordered maturation, prominent solar elastosis in dermis
Variants: pigmented, acantholytic, bowenoid, lichenoid, atrophic, hypertrophic, actinic cheilitis (confluence of AKs typically on lower lip), cutaneous horn (conical excrescence)
Treatment: cryotherapy, 5-fluorouracil, imiquimod, chemical peels, photodynamic therapy