Key Words
impetigo, cellulitis, erysipelas, gas gangrene, soft tissue infection, necrotizing fasciitis, folliculitis, sycosis barbae, acne keloidalis, distal dactylitis, meningitis, purpura fulminans
Skin Infections
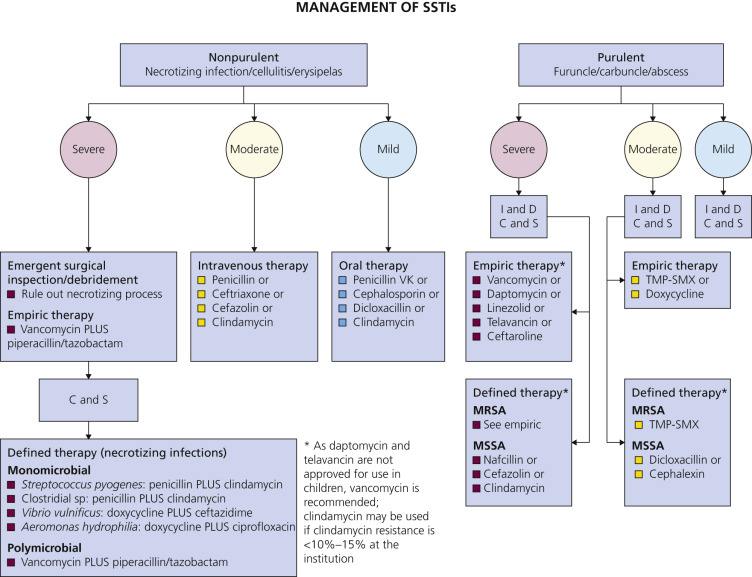
The two Gram-positive cocci Staphylococcus aureus and group A beta-hemolytic streptococci account for the majority of skin and soft tissue infections (SSTIs). S. aureus invades skin and causes impetigo, folliculitis, cellulitis, and furuncles. Elaboration of toxins by S. aureus causes the lesions of bullous impetigo and staphylococcal scalded skin syndrome. The streptococci are secondary invaders of traumatic skin lesions and cause impetigo, erysipelas, cellulitis, and lymphangitis. Skin and soft tissue infections may be categorized as superficial (impetigo, folliculitis) versus deep (cellulitis, erysipelas, necrotizing fasciitis) and/or nonpurulent (necrotizing infection/cellulitis, erysipelas) and purulent (furuncle, carbuncle, abscess). Fig. 9.1 describes a treatment approach for SSTIs.
Impetigo
Impetigo is a common, contagious, superficial skin infection that is produced by streptococci, staphylococci, or a combination of both bacteria. There are two different clinical presentations: bullous impetigo and nonbullous impetigo. Both begin as vesicles with a very thin, fragile roof consisting only of stratum corneum. Bullous impetigo is primarily a staphylococcal disease. Nonbullous impetigo was once thought to be primarily a streptococcal disease, but staphylococci are isolated from the majority of lesions in both bullous and nonbullous impetigo. S. aureus is now known to be the primary pathogen in both bullous and nonbullous impetigo.
Children in close physical contact with each other have a higher rate of infection than do adults. Symptoms of itching and soreness are mild; systemic symptoms are infrequent. Impetigo may occur after a minor skin injury such as an insect bite, but it most frequently develops on apparently unimpaired skin. The disease is self-limiting, but when untreated it may last for weeks or months. Although rare in developed countries (<1 case/1,000,000 population per year), glomerulonephritis following streptococcal infection may be a complication of impetigo caused by certain strains of Streptococcus pyogenes, but no data demonstrate that treatment of impetigo prevents this sequela. Rheumatic fever has not been reported as a complication of impetigo.
Bullous Impetigo
Bullous impetigo (staphylococcal impetigo) is caused by an epidermolytic toxin produced at the site of infection and usually is not secondarily contaminated by streptococci. The toxin causes intraepidermal cleavage below or within the stratum granulosum.
Clinical Manifestations.
Bullous impetigo is most common in infants and children but may occur in adults. It typically occurs on the face, but it may infect any body surface. There may be a few lesions localized in one area, or the lesions may be so numerous and widely scattered that they resemble poison ivy. One or more vesicles enlarge rapidly to form bullae in which the contents turn from clear to cloudy. The center of the thin-roofed bulla collapses, but the peripheral area may retain fluid for many days in an inner tube–shaped rim. A thin, flat, honey-colored, “varnish-like” crust may appear in the center and, if removed, discloses a bright red, inflamed, moist base that oozes serum. The center may dry without forming a crust, leaving a red base with a rim of scale. In most cases, a tinea-like scaling border replaces the fluid-filled rim as the round lesions enlarge and become contiguous with the others ( Figs. 9.2 to 9.10 ). The border dries and forms a crust. The lesions have little or no surrounding erythema. In some untreated cases, lesions may extend radially and retain a narrow, bullous, inner tube rim. These individual lesions reach 2 to 8 cm in diameter and then cease to enlarge, but they may remain for months (see Fig. 9.9 ). Thick crust accumulates in these longer-lasting lesions. Lesions heal with hyperpigmentation in black patients. Regional lymphadenitis is uncommon with pure staphylococcal impetigo. There is some evidence that the responsible staphylococci colonize in the nose and then spread to normal skin before infection.









Serious secondary infections (e.g., osteomyelitis, septic arthritis, and pneumonia) may follow seemingly innocuous superficial infections in infants.
Nonbullous Impetigo
Nonbullous impetigo originates as a small vesicle or pustule that ruptures to expose a red, moist base. A honey-yellow to white-brown, firmly adherent crust accumulates as the lesion extends radially ( Figs. 9.11 to 9.15 ). There is little surrounding erythema. Satellite lesions appear beyond the periphery. The lesions are generally asymptomatic. The skin around the nose and mouth and the limbs are the sites most commonly affected. The palms and soles are not affected. Untreated cases last for weeks and may extend in a continuous manner to involve a wide area (see Fig. 9.12 ). Most lesions heal without scarring. The sequence of events leading to nonbullous impetigo is exposure to the infectious agent, carriage on exposed normal skin, and finally skin infection after a minor trauma that is aggravated by scratching. The infecting strain has been found on normal skin surfaces 2 or more weeks before the appearance of lesions.





Intact skin is resistant to colonization or infection with group A beta-hemolytic streptococci, but skin injury by insect bites, abrasions, lacerations, and burns allows the streptococci to invade. A pure culture of group A beta-hemolytic streptococci may sometimes be isolated from early lesions, but most lesions promptly become contaminated with staphylococci. Regional lymphadenopathy is common. The reservoirs for streptococcal infection include the unimpaired normal skin or the lesions of other individuals, rather than the respiratory tract. Children ages 2 to 5 years commonly have streptococcal impetigo. Warm, moist climates and poor hygiene are predisposing factors. The antistreptolysin O (ASO) titer does not increase to a significant level following impetigo. Antideoxyribonuclease B (anti-DNase B) increases to high levels and is a much more sensitive indicator of streptococcal impetigo.
Laboratory Findings.
Diagnosis is based on history and clinical appearance. Cultures should be performed to identify if Staphylococcus aureus or beta-hemolytic Streptococcus are the causative organisms. Gram-stained smears of vesicles show Gram-positive cocci. Culture of exudate beneath an unroofed crust reveals group A streptococci, S. aureus, or a mixture of streptococci and S. aureus.
Prevention of Impetigo
Mupirocin or triple antibiotic ointment – containing bacitracin, Polysporin, and neomycin – applied three times daily to sites of minor skin trauma (e.g., mosquito bites and abrasions) can be efficacious as a preventative treatment.
Recurrent Impetigo
Patients with recurrent impetigo should be evaluated for carriage of S. aureus. The nares are the most common sites of carriage, but the perineum, axillae, and toe webs may also be colonized. Mupirocin ointment or cream applied to the nares twice each day for 5 days significantly reduces S. aureus carriage in the nose and hands at 3 days and in the nasal carriage for as long as 1 year.
Treatment of Impetigo
Impetigo may resolve spontaneously or become chronic and widespread; 2% mupirocin ointment or cream is effective. Retapamulin ointment is also approved for treating impetigo, but should not be used in the nose because of risk of epistaxis. Local treatment does not treat lesions that evolve in other areas. Infected children should be briefly isolated until treatment has begun. Patients may be treated with the topical antimicrobials mupirocin or retapamulin twice daily for 5 days. Recommended treatment is found in Tables 9.1 and 9.2 .
| Disease Entity | Antibiotic | Dosage, Adults | Dosage, Children * | Comment |
|---|---|---|---|---|
| Impetigo † ( Staphylococcus and Streptococcus ) | Dicloxacillin | 250 mg qid PO | N/A | N/A |
| Cephalexin | 250 mg qid PO | 25–50 mg/kg/day in 3–4 divided doses PO | N/A | |
| Erythromycin | 250 mg qid PO ‡ | 40 mg/kg/day in 3–4 divided doses PO | Some strains of Staphylococcus aureus and Streptococcus pyogenes may be resistant. | |
| Clindamycin | 300–400 mg qid PO | 20 mg/kg/day in 3 divided doses PO | N/A | |
| Amoxicillin–clavulanate | 875/125 mg bid PO | 25 mg/kg/day of the amoxicillin component in 2 divided doses PO | N/A | |
| Retapamulin ointment | Apply to lesions bid | Apply to lesions bid | For patients with limited number of lesions | |
| Mupirocin ointment | Apply to lesions bid | Apply to lesions bid | For patients with limited number of lesions | |
| MSSA SSTI | Nafcillin or oxacillin | 1–2 g every 4 h IV | 100–150 mg/kg/day in 4 divided doses | Parenteral drug of choice; inactive against MRSA |
| Cefazolin | 1 g every 8 h IV | 50 mg/kg/day in 3 divided doses | For penicillin-allergic patients except those with immediate hypersensitivity reactions. More convenient than nafcillin with less bone marrow suppression | |
| Clindamycin | 600 mg every 8 h IV or 300–450 mg qid PO | 25–40 mg/kg/day in 3 divided doses IV or 25–30 mg/kg/day in 3 divided doses PO | Bacteriostatic; potential of cross-resistance and emergence of resistance in erythromycin-resistant strains; inducible resistance in MRSA | |
| Dicloxacillin | 500 mg qid PO | 25–50 mg/kg/day in 4 divided doses PO | Oral agent of choice for methicillin-susceptible strains in adults. Not used much in pediatrics | |
| Cephalexin | 500 mg qid PO | 25–50 mg/kg/day 4 divided doses PO | For penicillin-allergic patients except those with immediate hypersensitivity reactions. The availability of a suspension and requirement for less frequent dosing | |
| Doxycycline, minocycline | 100 mg bid PO | Not recommended for age <8 y § | Bacteriostatic; limited recent clinical experience | |
| Trimethoprim– sulfamethoxazole | 1–2 double- strength tablets bid PO | 8–12 mg/kg (based on trimethoprim component) in either 4 divided doses IV or 2 divided doses PO | Bactericidal; efficacy poorly documented | |
| MRSA SSTI | Vancomycin | 30 mg/kg/day in 2 divided doses IV | 40 mg/kg/day in 4 divided doses IV | For penicillin allergic patients; parenteral drug of choice for treatment of infections caused by MRSA |
| Linezolid | 600 mg every 12 h IV or 600 mg bid PO | 10 mg/kg every 12 h IV or PO for children <12 y | Bacteriostatic; limited clinical experience; no cross-resistance with other antibiotic classes; expensive | |
| Clindamycin | 600 mg every 8 h IV or 300–450 mg qid PO | 25–40 mg/kg/day in 3 divided doses IV or 30–40 mg/kg/day in 3 divided doses PO | Bacteriostatic; potential of cross-resistance and emergence of resistance in erythromycin-resistant strains; inducible resistance in MRSA. Important option for children | |
| Daptomycin | 4 mg/kg every 24 h IV | N/A | Bactericidal; possible myopathy | |
| Ceftaroline | 600 mg bid IV | N/A | Bactericidal | |
| Doxycycline, minocycline | 100 mg bid PO | Not recommended for age <8 y § | Bacteriostatic; limited recent clinical experience | |
| Trimethoprim–sulfamethoxazole | 1–2 double- strength tablets bid PO | 8–12 mg/kg/day (based on trimethoprim component) in either 4 divided doses IV or 2 divided doses PO | Bactericidal; limited published efficacy data | |
| Non-Purulent SSTI (Cellulitis) | Adult Dosage | Pediatric Dosage | Antimicrobial Agents for Patients With Severe Penicillin Hypersensitivity | Comment |
| Streptococcal skin infections | Penicillin 2–4 million units every 4–6 h IV Clindamycin 600–900 mg every 8 h IV Nafcillin 1–2 g every 4–6 h IV Cefazolin 1 g every 8 h IV Penicillin VK 250–500 mg every 6 h PO Cephalexin 500 mg every 6 h PO | Penicillin 60–100,000 units/kg/dose every 6 h 10–13 mg/kg dose every 8 h IV 50 mg/kg/dose every 6 h 33 mg/kg/dose every 8 h IV | Clindamycin, vancomycin, linezolid, daptomycin, or telavancin. Clindamycin resistance is <1% but may be increasing in Asia | N/A |
* Doses listed are not appropriate for neonates. Refer to the report by the Committee on Infectious Diseases, American Academy of Pediatrics, for neonatal doses.
† Infection due to Staphylococcus and Streptococcus species. Duration of therapy is 7 days, depending on the clinical response.
‡ Adult dosage of erythromycin ethylsuccinate is 400 mg 4 times/day PO.
| Manifestation | Treatment | Adult Dose | Pediatric Dose | Class * | Comment |
|---|---|---|---|---|---|
| Abscesses, furuncles, carbuncles | Incision and drainage | AII | For simple abscesses or boils, incision and drainage is likely adequate. Please refer to Table 9.9 for conditions in which antimicrobial therapy is recommended after incision and drainage of an abscess due to CA-MRSA. | ||
| Purulent cellulitis (defined as cellulitis associated with purulent drainage or exudate in the absence of a drainable abscess) | Clindamycin | 300–450 mg PO tid | 10–13 mg/kg/dose PO every 6–8 h, not to exceed 40 mg/kg/day | AII | Clostridium difficile –associated disease may occur more frequently, compared with other oral agents. |
| TMP-SMX | 1–2 DS tab PO bid | Trimethoprim 4–6 mg/kg/dose, sulfamethoxazole 20–30 mg/kg/dose PO every 12 h | AII | TMP-SMX is pregnancy category C/D and not recommended for women in the third trimester of pregnancy and for children <2 months of age. | |
| Doxycycline | 100 mg PO bid | <45 kg: 2 mg/kg/dose PO every 12 h ≥45 kg: adult dose | AII | Tetracyclines are not recommended for children <8 years of age and are pregnancy category D. | |
| Minocycline | 200 mg 3 times daily, then 100 mg PO bid | 4 mg/kg PO 3 times daily, then 2 mg/kg/dose PO every 12 h | AII | ||
| Linezolid | 600 mg PO bid | 10 mg/kg/dose PO every 8 h, not to exceed 600 mg/dose | AII | More expensive compared with other alternatives. | |
| Nonpurulent cellulitis (defined as cellulitis with no purulent drainage or exudate and no associated abscess) | β-Lactam (e.g., cephalexin and dicloxacillin) | 500 mg PO 4 times daily | Please refer to Red Book | AII | Empirical therapy for beta-hemolytic streptococci is recommended (AII). Empirical coverage for CA-MRSA is recommended in patients who do not respond to β-lactam therapy and may be considered in those with systemic toxicity. |
| Clindamycin | 300–450 mg PO tid | 10–13 mg/kg/dose PO every 6–8 h, not to exceed 40 mg/kg/day | AII | Provides coverage for both beta-hemolytic streptococci and CA-MRSA | |
| β-Lactam (e.g., amoxicillin) and/or TMP-SMX or a tetracycline | Amoxicillin: 500 PO mg tid See above for TMP-SMX and tetracycline dosing | Please refer to Red Book See above for TMP-SMX and tetracycline dosing | AII | Provides coverage for both beta-hemolytic streptococci and CA-MRSA | |
| Linezolid | 600 mg PO bid | 10 mg/kg/dose PO every 8 h, not to exceed 600 mg/dose | AII |
* Classification of the strength of recommendation and quality of evidence applies to adult and pediatric patients unless otherwise specified. A slash (/) followed by the recommendation strength and evidence grade will denote any differences in pediatric classification. bid, twice daily; CA-MRSA, community-associated MRSA; DS, double strength; h, hour(s); PO, oral; tab, tablet; tid, three times daily; TMP-SMX, trimethoprim–sulfamethoxazole.
Oral Antibiotics.
Oral antibiotics should be employed in patients who develop numerous widespread lesions, systemic symptoms, or who are part of an outbreak, affecting close contacts.
A 7-day course of oral antibiotics induces rapid healing (see Fig. 9.1 ). Since most impetigo is caused by methicillin-susceptible S. aureus , dicloxacillin or cephalexin (erythromycin or clindamycin if penicillin allergic) are recommended as first-line agents. Suspected or confirmed methicillin-resistant S. aureus (MRSA) should be treated with doxycycline, clindamycin, or sulfamethoxazole–trimethoprim. When streptococci are alone responsible for impetigo, oral penicillin is the treatment of choice. During community outbreaks of poststreptococcal glomerulonephritis, oral antibiotics should be administered to assist in eliminating nephritogenic strains of Str. pyogenes from the community.
Mupirocin.
Mupirocin ointment or cream was the first topical antibiotic approved for the treatment of impetigo. It is active against staphylococci (including methicillin-resistant strains) and streptococci. The drug is not active against Enterobacteriaceae, Pseudomonas aeruginosa , or fungi. It is as effective as oral antibiotics and is associated with fewer adverse effects. In superficial skin infections that are not widespread, mupirocin ointment offers several advantages. It is highly active against the most frequent skin pathogens, even those resistant to other antibiotics, and the topical route of administration allows delivery of high drug concentrations to the site of infection. Mupirocin is applied three times a day until all lesions have cleared. If topical treatment is elected, then it might be worthwhile to wash the involved areas once or twice a day with an antibacterial soap such as Hibiclens or Betadine. Washing the entire body with these soaps may prevent recurrence at distant sites. Crusts should be removed because they block the penetration of antibacterial creams. To facilitate removal, soften crusts by soaking with a wet cloth compress.
Retapamulin.
Topical retapamulin is approved for the treatment of uncomplicated superficial skin infections caused by S. aureus (excluding MRSA) and Streptococcus pyogenes in patients older than age 9 months. Application of retapamulin 1% ointment twice daily for 5 days is effective for impetigo but the efficacy is reduced in patients with MRSA infections or superficial abscesses.
Cellulitis and Erysipelas
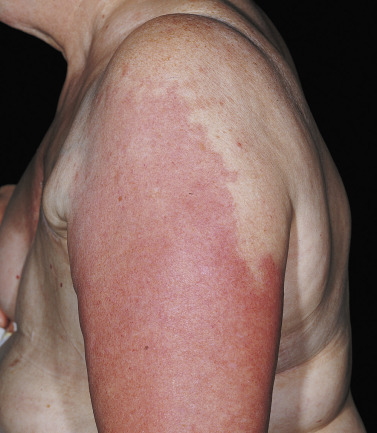
Cellulitis and erysipelas are skin infections characterized by erythema, edema, and pain ( Figs. 9.16 to 9.20 ). In most instances there is fever and leukocytosis. Both may be accompanied by lymphangitis and lymphadenitis. Pathogens enter at sites of local trauma or abrasions and at psoriatic, eczematous, or tineal lesions. Erysipelas involves the superficial layers of the skin and cutaneous lymphatics; cellulitis extends into the subcutaneous tissues.




Cellulitis is an infection of the dermis and subcutaneous tissue that is usually caused by a group A streptococcus – S. aureus in adults and Haemophilus influenzae type b in children younger than 3 years of age. Cellulitis is sometimes caused by other organisms. Cellulitis typically occurs near surgical wounds or a cutaneous ulcer or, like erysipelas, may develop in apparently normal skin. There are many anatomic variants of cellulitis ( Table 9.3 ). There is no clear distinction between infected and uninfected skin. Recurrent episodes of cellulitis occur with local anatomic abnormalities that compromise the venous or lymphatic circulation. The lymphatic system can be compromised by a previous episode of cellulitis, surgery with lymph node resection, and radiation therapy.
| Anatomic Variant or Cause of Predisposition | Location | Likely Bacterial Causes |
|---|---|---|
| Periorbital cellulitis | Periorbital | Staphylococcus aureus, pneumococcus, group A streptococcus |
| Buccal cellulitis | Cheek | Haemophilus influenzae |
| Cellulitis complicating body piercing | Ear, nose, umbilicus | S. aureus, group A streptococcus |
| Mastectomy (with axillary-node dissection) for breast cancer | Ipsilateral arm | Non–group A hemolytic streptococcus |
| Lumpectomy (with limited axillary-node dissection, breast radiotherapy) | Ipsilateral breast | Non–group A hemolytic streptococcus |
| Harvest of saphenous vein for coronary artery bypass | Ipsilateral leg | Group A or non–group A hemolytic streptococcus |
| Liposuction | Thigh, abdominal wall | Group A streptococcus, peptostreptococcus |
| Postoperative (very early) wound infection | Abdomen, chest, hip | Group A streptococcus |
| Injection drug use (“skin popping”) | Extremities, neck | S. aureus ; streptococci (groups A, C, F, G) * |
| Perianal cellulitis | Perineum | Group A streptococcus |
| Crepitant cellulitis | Trunk, extremities | |
| Gangrenous cellulitis | Trunk, extremities | |
| Erythema migrans (bright red, circular lesion at initial sites; secondary annular lesions may develop elsewhere several days later because of hematogenous spread) | Extremities, trunk | Borrelia burgdorferi (agent of Lyme disease) |
* Other bacteria to consider on the basis of isolation from skin or abscesses in this setting include Enterococcus faecalis , viridans -group streptococci, coagulase-negative staphylococci, anaerobes (including Bacteroides and Clostridium species), and Enterobacteriaceae.
Erysipelas is an acute, inflammatory form of cellulitis that differs from other types of cellulitis in that lymphatic involvement (“streaking”) is prominent. The area of inflammation is raised above the surrounding skin, and there is a distinct demarcation between involved and normal skin. The lower legs, face, and ears are most frequently involved. The differential diagnosis of cellulitis is shown in Table 9.4 .
| Disease | Description |
|---|---|
| Anthrax (cutaneous) | Edema surrounding crusted lesion. Painless or itching. Animal contact. |
| Calciphylaxis (calcific uremic arteriolopathy) | Affects diabetic patients with end-stage renal disease and hyperparathyroidism who are receiving renal replacement therapy. Metastatic calcification leads to small vessel vasculopathy. Early stage: presents with nonulcerating plaques in the calves. Lesions eventually become necrotic and painful ulcers develop. |
| Carcinoma erysipelatoides | A form of metastatic carcinoma with lymphatic involvement. Seen on anterior chest wall in breast cancer and sites of distant metastasis. No fever, slow progression. If a suspected breast infection does not resolve with antibiotics, mammography and tissue biopsy are indicated. |
| Contact dermatitis (acute) | Lesion sharply demarcated and constricted to the area of exposure. Pruritus present, not in cellulitis. Topical steroids effective. Systemic corticosteroids are indicated for severe cases. Secondary infection may complicate dermatitis. |
| Deep venous thrombophlebitis | Unilateral leg edema, warmth, or erythema. Tenderness along involved veins. Can have low-grade fever, leukocytosis. Duplex ultrasonography diagnostic. |
| Eosinophilic cellulitis (Wells syndrome) | Acute pruritic dermatitis. Hive-like lesions with central clearing. Lesions evolve over 2–3 days and resolve without scarring in 2–8 weeks. Disease recurs. Peripheral eosinophilia, during acute phase. Biopsy: eosinophils. Idiopathic or associated with myeloproliferative, immunologic, and infectious disorders and with medications. Responds to oral corticosteroids. |
| Erysipeloid ( Erysipelothrix rhusiopathiae ) | Acute bacterial infection (Erysipelothrix rhusiopathiae) of traumatized skin. Contact with infected meat or contact with infected animals or fish. Lesions affect hands; well-demarcated, bright red to purple plaques with a smooth, shiny surface. |
| Erythema migrans | Lyme disease rash that typically expands but clears in center. Often single or multiple lesions occur that are round and red and expand to many centimeters but do not show central clearing. |
| Erythema nodosum | Most common panniculitis. Raised, painful, bilateral, tender lesions located over both shins. Lesions may coalesce and resemble cellulitis. |
| Factitial | Mechanical or chemical manipulation of skin can produce an area of erythema that resembles cellulitis. |
| Familial Hibernian fever | Irish ancestry; rare. Erysipelas-like lesion may occur anywhere on body; most common site is on a limb. Begins proximally and migrates distally during an attack. Lesion (about 15 cm in diameter) is well-demarcated, red, warm, and painful. Corticosteroids effective. |
| Familial Mediterranean fever | Autosomal recessive. Jews and Arabs from Mediterranean basin. Acute self-limited episodes of fever accompanied by peritonitis, pleuritis, pericarditis, or synovitis. Initial attack: childhood or early adolescence. Erysipelas-like erythema. Tender, red, well-demarcated, warm, swollen areas with a diameter of 10–15 cm. Occur below knee, on anterior leg or dorsum of foot (unilaterally or symmetrically). Erythema subsides in 24–48 hours as acute attack resolves. Recurs. Responds to colchicine. |
| Fixed drug eruption | A well-demarcated plaque that recurs at same site each time offending drug is taken. Itching or burning not seen in cellulitis. Most commonly affected areas are lips and genitalia. |
| Foreign-body granulomatous reactions (silicone injections, paraffin oils) | Material injected into skin can stimulate an overlying erythema. |
| Glucagonoma | Pancreatic tumor that is almost always malignant; presents with diabetes mellitus, diarrhea, and weight loss. Necrolytic migratory erythema is a rash that begins as an erythematous area and gradually spreads; after central crusting occurs, the lesions heal. Affects intertriginous, perioral, and perigenital areas. |
| Gouty arthritis (acute) | Joint inflamed with overlying erythema and warmth. May lead to tendinitis and bursitis. Chills, low-grade fever, elevated leukocyte count. Typically monoarticular, lower extremity, usually first metatarsophalangeal joint or knee. |
| Insect stings or bites and other envenomations | Swelling that can extend over a large area; peaks within 48 hours and lasts up to 7 days. No lymphangitis. Pruritus distinguishes this lesion from infectious cellulitis. Envenomations by marine animals cause a similar picture. |
| Leukemia/lymphoma | Lymphoma diagnosed after failure of antimicrobial therapy. Persisting fever or generalized lymphadenopathy may suggest the diagnosis. |
| Lymphedema | Nonpitting edema, erythema, induration of an extremity. No fever, no response to antibiotics. May be complicated by infection, recurrently. Lymphangioscintigraphy confirms diagnosis. |
| Necrotizing fasciitis | A rapidly advancing erythema. Begins with fever and chills. Vesicles and bullae may form and drain fluid. Painless ulcers appear as the process spreads. |
| Panniculitis | Pancreatic disease, either inflammatory or neoplastic, may lead to panniculitis presenting as tender, red nodules located on pretibial regions, thighs, or buttocks. Lupus panniculitis occurs on face and upper extremities. α 1 -Antitrypsin deficiency may present as cellulitis on trunk and proximal extremities, often precipitated by trauma. Panacinar emphysema, noninfectious hepatitis, and cirrhosis should suggest the diagnosis. Protein electrophoresis reveals low levels of α 1 -antitrypsin. Some patients respond to dapsone or α 1 -protease inhibitor concentrate. Other forms of panniculitis are Weber–Christian disease, cytophagic histiocytic panniculitis, poststeroid panniculitis, and nodular panniculitis. Deep excisional biopsies rather than punch biopsy are required to diagnose panniculitis. |
| Polyarteritis nodosa | Subcutaneous, inflammatory, red to bluish nodules (2 cm in diameter) that follow the course of involved arteries; lower extremities, often bilateral; becomes confluent to form painful subcutaneous plaques that may resemble cellulitis. Ulcers may occur. |
| Pyoderma gangrenosum | An ulcerative cutaneous disease. Ulcers may follow trauma. An atypical form occurs on the hand. A red ulcer border may be misinterpreted as infection. |
| Relapsing polychondritis | Affects cartilaginous structures. Auricular chondritis is most common manifestation, usually both ears; cellulitis is usually unilateral with regional lymphadenopathy. Relapsing polychondritis spares earlobe because this structure is not cartilaginous. Recurrent inflammation causes auricular or saddle-nose deformity. Associated features include peripheral, nonerosive polyarthritis; episcleritis; keratitis or uveitis; and aortic valve insufficiency. |
| Sarcoidosis | Atypical lesions manifest as indurated red plaques with edema and pain. |
| Superficial thrombophlebitis | Gradual onset of localized tenderness, followed by erythema along the path of a superficial vein. Varicose veins, prolonged travel, or enforced stasis may be the cause. |
| Sweet syndrome (acute febrile neutrophilic dermatosis) | Papules that coalesce to form inflammatory plaques (red and tender); upper extremities, face, and neck. Fever, arthralgia, or arthritis. Moderate neutrophilia. Biopsy: dermal polymorphonuclear leukocytes. 10% have an associated malignant condition (e.g., acute myelogenous leukemia). Corticosteroids effective. |
Diagnosis of Cellulitis
Recognizing the distinctive clinical features (erythema, warmth, edema, and pain) is the most reliable way of making an early diagnosis. Isolation of the etiologic agent is difficult and is usually not attempted. Fever, mild leukocytosis with a left shift, and a mildly increased sedimentation rate may be present. Patients with cellulitis of the leg often have a preexisting lesion, such as an ulcer or erosion that acts as a portal of entry for the infecting organism.
Cellulitis Versus Deep Vein Thrombosis.
Differentiating cellulitis from deep vein thrombosis (DVT) is a common clinical dilemma. Patients with cellulitis are more likely to have constitutional symptoms, rigors, and a history of diabetes and/or distinct margins of erythema. Diabetic patients are at increased risk for skin infections. Diabetes is not a known risk factor for DVT. Patients with DVT are more likely to have had recent surgery and a history of varicose veins and/or peripheral vascular disease. Patients with a diagnosis of DVT are more likely to have an elevated white blood cell (WBC) count. Aspiration and culture of fluid from the leading edge of the affected specimen is of limited value. Cellulitis is usually diagnosed clinically. Contrast venography is the accepted “gold standard” for the objective diagnosis of DVT. Venous duplex ultrasonography is now the first-line diagnostic test for DVT because it does not use contrast media.
Cultures.
In adults with no underlying disease, yields of cultures of aspirate specimens, biopsy specimens, and blood samples are low. In adults with underlying diseases (e.g., diabetes mellitus, hematologic malignancies, intravenous drug abuse, human immunodeficiency virus infection, chemotherapy) results of culture are more productive. Cellulitis in these patients is often caused by organisms other than S. aureus or group A streptococcus, such as Acinetobacter , Clostridium septicum , Enterobacter , Escherichia coli , H. influenzae , Pasteurella multocida , Proteus mirabilis , P. aeruginosa, and group B streptococci. Cultures of entry sites, aspirate specimens, biopsy specimens, and blood samples facilitate the selection of the appropriate antibiotic for these patients.
Optimal methods for etiologic diagnosis in adults have not been delineated. Culture of the lesion is a more predictable source of information than more invasive procedures. Leading-edge and midpoint aspirates after saline injection and blood cultures are of little value in normal hosts. A higher concentration of bacteria may be found at the point of maximal inflammation. Needle aspiration from the point of maximal inflammation yielded a 45% positive culture rate, compared with a 5% rate from leading-edge cultures. Needle aspiration is performed by piercing the skin with a 20-gauge needle mounted on a tuberculin syringe. A 22-gauge needle is used for facial lesions. The needle is introduced into subcutaneous tissue. Suction is applied as the needle is withdrawn. Most clinicians do not culture, and proceed to treat with oral antibiotics.
Treatment of Cellulitis
Treatment of cellulitis is derived from the recommendations of the Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary .
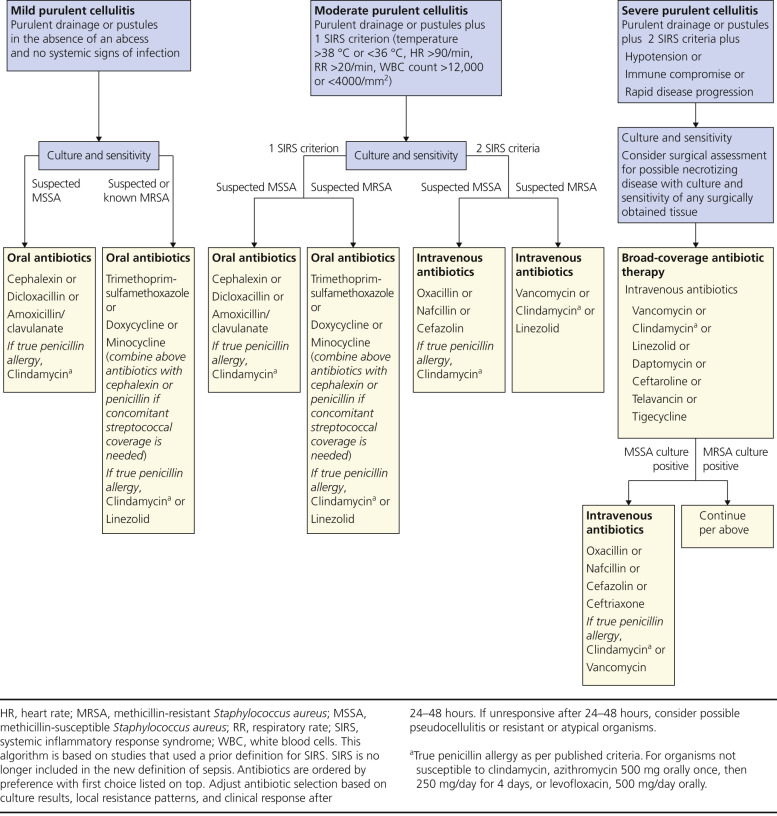
Patients With Purulent Cellulitis.
For outpatients with purulent cellulitis (e.g., cellulitis associated with purulent drainage or exudate in the absence of a drainable abscess), empirical therapy for cellulitis-associated MRSA (CA-MRSA) is recommended pending culture results. Empirical therapy for infection attributable to beta-hemolytic streptococci is likely to be unnecessary. Approximately 5 to 10 days of therapy is recommended but should be individualized on the basis of the patient’s clinical response.
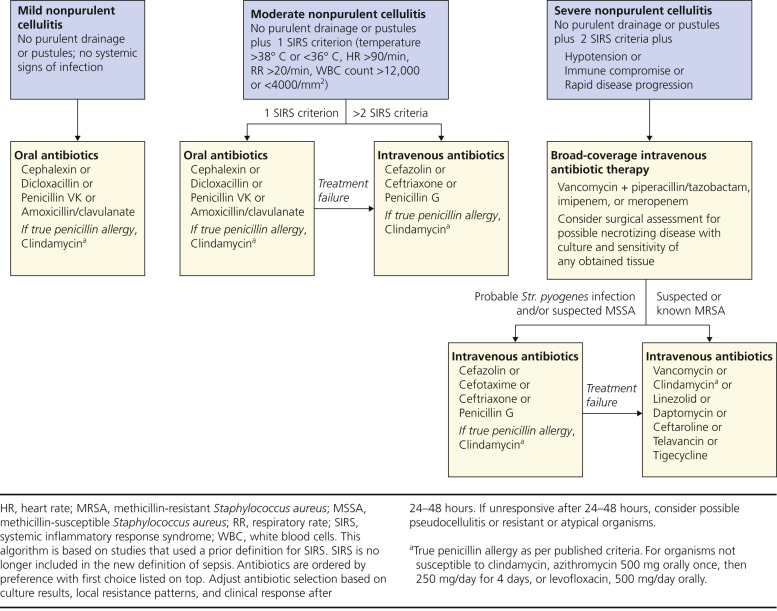
Patients With Nonpurulent Cellulitis.
For outpatients with nonpurulent cellulitis (e.g., cellulitis with no purulent drainage or exudate and no associated abscess), empirical therapy for infection attributable to beta-hemolytic streptococci is recommended (see Tables 9.1 and 9.2 ). The role of CA-MRSA is unknown. Empirical coverage for CA-MRSA is recommended in patients who do not respond to β-lactam therapy and may be considered in those with systemic toxicity. Five to 10 days of therapy is recommended but should be individualized on the basis of the patient’s clinical response.
Elevation of the affected area promotes drainage of the edema and hastens recovery for lower leg infections. Pain can be relieved with cool compresses. Treat underlying conditions that may predispose to the infection, such as tinea pedis, stasis dermatitis, or trauma.
Antibiotics.
Either β-lactam or non-β-lactam antibiotics can be used to treat uncomplicated cellulitis (see Tables 9.1 and 9.2 and Box 9.1 ). The use of empirical β-lactam antibiotics provided several minor advantages. The safety of cephalosporins and the propensity for adverse effects with trimethoprim–sulfamethoxazole (TMP-SMX), clindamycin, and fluoroquinolones are known. Patients with uncomplicated cellulitis are those without ulceration or abscesses, significant immunosuppression, drainage or debridement, or intravenous therapy. These patients can receive oral medications from the start. Macrolide resistance among group A streptococci has increased regionally in the United States.
β-Lactam Therapy
Cephalexin
Other β-lactam therapy
Dicloxacillin
Amoxicillin/clavulanate
Other (cefuroxime, cefpodoxime, penicillin, amoxicillin)
Non-β-Lactam Therapy
Clindamycin
Trimethoprim–sulfamethoxazole
Fluoroquinolone (gatifloxacin, ciprofloxacin)
Macrolides (erythromycin, azithromycin, clarithromycin)
Tetracyclines (tetracycline, doxycycline, minocycline)
Combination therapy (two non-β-lactams)
For empirical coverage of CA-MRSA in outpatients with SSTI, oral antibiotic options include the following: clindamycin, TMP-SMX, a tetracycline (doxycycline or minocycline), and linezolid. If coverage for both beta-hemolytic streptococci and CA-MRSA is desired, options include clindamycin alone or TMP-SMX or a tetracycline in combination with a β-lactam (e.g., amoxicillin) or linezolid alone. The use of rifampin as a single agent or as adjunctive therapy for the treatment of SSTI is not recommended (also see Tables 9.1 and 9.2 and Box 9.1 ).
Hospitalized Patients.
In hospitalized patients with complicated SSTI (cSSTI; defined as patients with deeper soft tissue infections, surgical/traumatic wound infection, major abscesses, cellulitis, and infected ulcers and burns), in addition to surgical debridement and broad-spectrum antibiotics, empirical therapy for MRSA should be considered pending culture data. Options include intravenous (IV) vancomycin, oral or IV linezolid 600 mg twice daily, daptomycin 4 mg/kg/dose IV once daily, telavancin 10 mg/kg/dose IV once daily, and clindamycin 600 mg IV or PO three times a day. A β-lactam antibiotic (e.g., cefazolin) may be considered in hospitalized patients with nonpurulent cellulitis with modification to MRSA-active therapy if there is no clinical response. About 7 to 14 days of therapy is recommended but should be individualized on the basis of the patient’s clinical response.
Cultures.
Cultures from abscesses and other purulent SSTIs are recommended in patients treated with antibiotic therapy, patients with severe local infection or signs of systemic illness, and patients who have not responded adequately to initial treatment, and also if there is concern for a cluster or outbreak.
Preventing Recurrent Cellulitis
Each attack of cellulitis causes lymphatic inflammation and possibly some permanent damage. Severe or repeated episodes of cellulitis may lead to lymphedema, sometimes substantial enough to cause elephantiasis. Measures to reduce recurrences of cellulitis include treating interdigital maceration, keeping the skin well hydrated with emollients to avoid dryness and cracking, and reducing any underlying edema by such methods as elevation of the extremity, use of compressive stockings or pneumatic pressure pumps, and, if appropriate, implementation of diuretic therapy.
Prophylactic Antibiotics to Prevent Recurrence.
Prolonged antimicrobial prophylaxis is effective and safe in preventing recurrent episodes of soft tissue infections and may be continued for months or years. Streptococci cause most cases of recurrent cellulitis. Treatment options include monthly intramuscular benzathine penicillin injections of 1.2 milliunits in adults or oral therapy with twice-daily doses of either 250 mg of erythromycin or 1 g of penicillin V. An alternative is to provide oral antibiotics to initiate therapy as soon as symptoms of infection begin. Low-dose oral clindamycin has been advocated for the prevention of recurrent staphylococcal skin infections and might also be useful for the prevention of recurrent cellulitis.
A large trial provides evidence that patients with two or more episodes of leg cellulitis who are given prophylactic penicillin (250 mg twice daily) for 12 months have fewer recurrences. Patients with a high body mass index (BMI), preexisting edema, or at least three episodes of previous cellulitis were less likely to have a response to prophylaxis than other patients. It was unclear how long prophylaxis should be continued. Patients with a high BMI might benefit from a higher dose of penicillin.
Children.
H. influenzae cellulitis is now rare since the introduction of H. influenzae type b (Hib) vaccine. The vaccine is now used in the routine immunization schedule of more than 100 countries.
Cellulitis of Specific Areas
Cellulitis and Erysipelas of the Extremities
Cellulitis of the extremities is most often caused by group A beta-hemolytic streptococci and is characterized by an expanding, red, swollen, tender-to-painful plaque with an indefinite border that may cover a small or wide area (see Figs. 9.17 and 9.18 ). Chills and fever occur as the red plaque spreads rapidly, becomes edematous, and sometimes develops bullae or suppurates. Less acute forms detected around a stasis leg ulcer spread slowly and may appear as an area of erythema with no swelling or fever. Erysipelas of the lower extremity is now more common than facial erysipelas. Group G streptococci may be a common pathogen, especially in patients older than 50 years. Red, sometimes painful, streaks of lymphangitis may extend toward regional lymph nodes. Repeated attacks can cause impairment of lymphatic drainage, which predisposes the patient to more infection and permanent swelling. This series of events takes place most commonly in the lower legs of patients with venous stasis and ulceration. The end stage, which includes dermal fibrosis, lymphedema, and epidermal thickening on the lower leg, is called elephantiasis nostras.
Treatment.
Treatment with oral or IV antibiotics should be started immediately and, if appropriate, altered according to laboratory results (see Table 9.1 , Figs. 9.21 and 9.22 ). The mean time for healing after treatment is initiated is 12 days, with a range of 5 to 25 days. See the Treatment of Cellulitis section for more details.
Facial Erysipelas and Cellulitis in Adults
Erysipelas.
The archaic term St. Anthony’s Fire accurately describes the intensity of this eruption. Erysipelas is a superficial cellulitis with lymphatic involvement. Isolated cases are the rule; epidemic forms are rare. Facial sites have become rare but erysipelas of the legs is common. It may originate in a traumatic or surgical wound, but no portal of entry can be found in most cases. In the preantibiotic era, erysipelas was a feared disease with a significant mortality, particularly in infants. Most contemporary cases are of moderate intensity and have a benign course. In the majority of cases, group A streptococci are the responsible organisms. The second most frequent causative organism is group G streptococci.
After prodromal symptoms that last from 4 to 48 hours and consist of malaise, chills, fever (101 to 104° F), and occasionally anorexia and vomiting, one or more red, tender, firm spots appear at the site of infection. These spots rapidly increase in size, forming a tense, red, hot, uniformly elevated, shining patch with an irregular outline and a sharply defined, raised border (see Fig. 9.19 ). As the process develops, the color becomes a dark, fiery red and vesicles appear at the advancing border and over the surface. Symptoms of itching, burning, tenderness, and pain may be moderate to severe. Without treatment, the rash reaches its height in approximately 1 week and subsides slowly over the next 1 or 2 weeks.
Recurrence.
Recurrence after antibiotic treatment occurs in 18% to 30% of cases. In particularly susceptible people, erysipelas may recur frequently for a long period and, by obstruction of the lymphatics, cause permanent thickening of the skin (lymphedema). Subsequent attacks may be initiated by the slightest trauma or may occur spontaneously to cause further irreversible skin thickening. The pinna and lower legs are particularly susceptible to this recurrent pattern (see Fig. 9.20 ).
Treatment.
Treatment is the same as that for streptococcal cellulitis (see Table 9.1 ). Recurrent cases may require long-term prophylactic treatment with low-dose penicillin or erythromycin. If other organisms are found on culture, a different agent is needed. See the Treatment of Cellulitis section for more details.
Perianal Cellulitis
Cellulitis (group A beta-hemolytic streptococcus) around the anal orifice is often misdiagnosed as candidiasis. It occurs more frequently in children than in adults. Bright, perianal erythema extends from the anal verge approximately 2 to 3 cm onto the surrounding perianal skin ( Figs. 9.23 and 9.24 ). Boys are affected more than girls. Symptoms include painful defecation (52%), tenderness, soilage from oozing, and, sometimes, blood-streaked stool and perianal itching (78%). These children are not systemically ill. Pharyngitis may precede the infection. The differential diagnosis includes Candida intertrigo, psoriasis, pinworm infection, inflammatory bowel disease, a behavioral problem, and child abuse. Culture results confirm the diagnosis.


Initial treatment consists of a 10- to 14-day course of penicillin, amoxicillin–clavulanic acid, erythromycin, or other macrolides. Relapses occurred in 39% of the patients. After treatment, a new culture specimen should be taken to check for recurrence. The topical antibiotic mupirocin may also provide rapid relief of symptoms, but systemic therapy is also required because it will treat any persistent oropharyngeal focus of streptococcal infection.
Necrotizing Skin and Soft Tissue Infections
Necrotizing SSTIs are often deep and devastating. They may involve the fascial and/or muscle compartments and can cause destruction of tissue and be fatal. They are often secondary infections that develop from a break in the skin from trauma or surgery. They are usually caused by streptococci or mixed bacterial flora. Features that suggest that deeper tissues are involved are shown in Box 9.2 .
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


