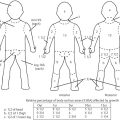
14 Back and Trunk Reconstruction Abstract This chapter will review back and trunk reconstruction for defects cause by trauma and tumor resection. The reader will be able to outline a management plan, draw incision for local flaps, and present alternative reconstructions in the case of wound recurrence. Keywords: back reconstruction, myelomeningocele, sternal defect Six Key Points • Back defects can often be covered with local flaps. • Sternal wounds can be covered with pectoralis flaps, rectus abdominis flaps, or omental flaps. • Thoracic defects can be covered with latissimus flaps if the blood supply hasn’t been interrupted. • Infected mesh must be removed. • Infected mesh does not need to be replaced if a capsule has formed. • Free flap coverage is an option if blood supply is interrupted to regional flaps. A Plastic Surgery consult is placed for management of a myelomeningocele in a neonate (Fig. 14.1) 1. What do you see? There is a large sacral wound in a neonate. Other things to note about its appearance are its posture, particularly its flexed position, and it has a difference in color between the upper half and the lower half of the body, similar to a harlequin baby. 2. Why is the color significant? Neonates, and in particular neonates with myelomeningocele, have autonomic dysfunction that may lead to abnormalities in perfusion. This is particularly significant in a child with a myelomeningocele because an inferiorly based flap may have difficulty with perfusion. 3. Why is the posture significant? The posture can signify what the long-term mobility may be. Some patients with myelomeningocele are ambulatory, while some are confined to a wheelchair. In a patient confined to a wheelchair, planning of the operation must balance coverage needs and preservation of functional muscle, including latissimus. 4. Neurosurgery is planning to take the child to the operating room. How do you plan coverage? The first-line coverage that I would use is local flaps. It is important to know how neurosurgery is planning to cover the dura—with a primary repair or with a graft. If there is a graft, there must be vascularized tissue over the defect. 5. What flap do you use? For this defect, bilateral rotational flaps. 6. Draw it. The drawing can be seen in Fig. 14.2. Fig. 14.2 Red dotted lines indicate planned incisions for coverage of a myelomeningocele defect. 7. Do you take fascia or latissimus muscle with the flaps? Because the fascia and the muscle are so thin in a 1-day-old neonate, it is difficult to take fascia. The latissimus muscle is also very thin. In this case, it is best to preserve the latissimus both as a lifeboat in case the flap does not survive and as a functional muscle for mobility in a wheelchair. Paraspinous muscle can be turned over for coverage. 8. What are operative considerations with paraspinous muscle? Paraspinous muscle is also an option for coverage, and in fact in a 15-year review accounted for 40% of dural coverage.1 Elevation and rotation of the paraspinous musculature must be performed in consultation with neurosurgery, as in some cases the nerve roots can have anomalous courses and elevation of the paraspinous musculature must take that into account. 9. What are other options for designs of flap coverage? Other designs include unilateral or bilateral rhomboid flaps, and other rotational flap designs such as a Yin-Yang design (Fig. 14.3). 10. How do you counsel the parents about postoperative complications? Parents are informed of postoperative complications, which can include skin edge separation, flap separation, flap necrosis, cerebrospinal fluid (CSF) leak, pseudomeningocele, hematoma, seroma, and infection. 11. The nurse calls on postoperative day 2 and states that there is a small amount of clear sticky fluid coming out of the wound. What do you do? The first step is to confirm that it is not CSF. After involving neurosurgery, if there is enough of a sample it can be sent for analysis for beta-2 transferrin,2 although that test can take some time. If it is, the patient may be a candidate for a shunt. 12. It is not CSF fluid. What do you do? It is then managed conservatively with local wound care and daily examinations to confirm it is not developing into a seroma. 13. The nurses call you and state there appears to be a wound separation on postoperative day 4. What do you do? The first step is to evaluate the wound. If it is a small separation, additional nylon sutures can be placed at the bedside. If nylon sutures will not hold the tissue together, wet to dry dressing changes can be used or silver sulfadiazine can be used. 14. The nurses call and state that the tip of the left-sided flap looks dusky. What do you do? After observing the extent of the duskiness and evaluating for surrounding cellulitis and fluid collections, it is most appropriate to treat conservatively. 15. The nurses are concerned that the dural repair is showing. The dural repair, if vascularized, can be managed conservatively. Some authors describe placing skin grafts over the dural repair, although without infection or CSF leak, conservative management is appropriate at this time. A Plastic Surgery consult is placed for coverage of the defect shown in Fig. 14.4
Questions
Case 1

Case 2
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine