CHAPTER 35 Autologous contouring the lower face
Physical evaluation
1. Midface evaluation
Malar fat pad
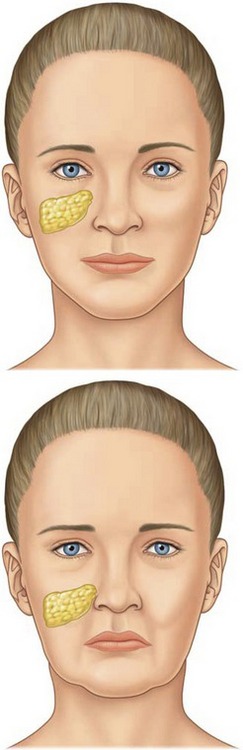
In a youthful midface, the superior border of the triangular shaped malar fat pad lies along the orbital rim and extends laterally to the zygomas (Fig. 35.1). The lateral border can be identified by drawing a line from the lateral canthus to the lateral commissure. The malar fat pad is located beneath the skin and subcutaneous fat, but it is superficial to the superficial muscular aponeurotic system (SMAS). It is fibrous and fatty, and it is readily distinguishable from the overlying subcutaneous fat. With advancing age, the malar fat pad descends inferiorly and medially. Ptosis of the malar fat pad empties the midface and accentuates tear-trough and nasolabial folds. To a lesser extent, this displacement also results in the formation of labiomandibular folds (marionette lines) and jowls.
Nasolabial fold
The cutaneous insertion of the zygomaticus major/minor and levator labii superioris muscles determines the nasolabial fold. In a sense, the nasolabial fold may be considered a fasciocutaneous ligament necessary for lip elevating muscles to initiate a smile. Laxity of this fasciocutaneous ligament causes the malar fat pad to travel inferomedially over the crease to deepen the nasolabial fold.
2. Lip evaluation
Labiomental fold
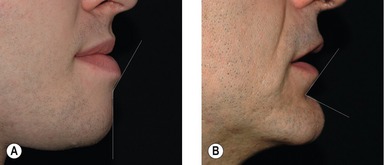
The position of the labiomental fold contributes to the appearance of the vertical height of the chin. A high labiomental fold will make the chin appear larger, and a low labiomental fold will make the chin appear smaller and more defined. A shallow or indistinct labiomental fold makes the chin appear larger because the demarcation between the lower lip and the chin pad is less well defined. The surgeon can also imagine the labiomental fold in profile as an angle (Fig. 35.2). A shallow fold has an obtuse angle and a deep fold has a more acute angle. Viewing the labiomental fold as an angle can be helpful when planning chin surgery. For example, performing an augmentation genioplasty on a patient with a low, deep labiomental fold will make the fold angle more acute and the fold will appear too deep.
3. Occlusion
Dental occlusion also affects the appearance of the lower-third of the face. For example, a deep bite may contribute to lower lip eversion with an oblique inclination as well as an acute angle at the labiomental fold. It is important to assess dental occlusion and inquire about prior orthodontic or orthognathic treatment. The treatment of patients with Angle Class II or Class III malocclusion is beyond the scope of this chapter.
4. Chin evaluation
Chin pad thickness
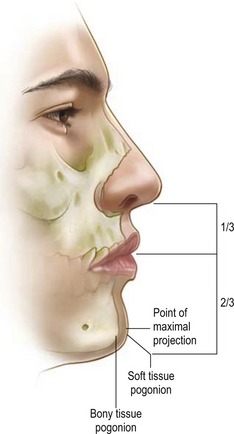
The chin pad is assessed by palpation. Chin pad soft tissue projection should be maximally at the level of the pogonion (Fig. 35.3). Static chin pad position should be noted. A chin pad cleft represents a cleft in the mentalis muscle as well as a deficiency of the chin pad soft tissue.
Orientation of deficiency or excess
The vertical, anteroposterior, and transverse dimensions of the dysmorphic chin should be analyzed.









