Upper lid blepharoplasty is the most common plastic surgery procedure in Asia and has consistently maintained its position as cultural acceptance and techniques have evolved. Asian upper lid blepharoplasty is a complex procedure that requires comprehensive understanding of the anatomy and precise surgical technique. The creation of the supratarsal crease has gone through many evolutions in technique but the principles and goals remain the same: a functional, natural-appearing eyelid crease that brings out the beauty of the Asian eye. Recent advances have improved functional and aesthetic outcomes of Asian upper lid blepharoplasty.
Key points
- •
Asian upper lid blepharoplasty is a common procedure that requires precise technique and understanding of key anatomic differences.
- •
The goal is to create a natural upper lid crease with manipulation of the tarso-levator junction and skin tension around the medial epicanthus.
Introduction
Upper lid blepharoplasty is the most common plastic surgery procedure in Asia and has consistently maintained its position over the past three decades as cultural acceptance and techniques have evolved. Eyelid aesthetics cannot be underestimated because they can exert significant social and economic influence in an extremely homogenous Asian society. A highly competitive culture mixed with modern values for beauty has created a constant demand for this procedure.
Surgical creation of the supratarsal crease has become synonymous with the term “double eyelid” surgery. The premise of the operation is to create a supratarsal crease that creates an eyelid that is more aesthetically pleasing. The term “double eyelid” is a bit of a misnomer, because creation of a supratarsal crease does not actually create another eyelid; it is simply a translation of the Korean term “ssang-cupul” (쌍꺼풀 双眼皮), which has come about from the Chinese character “ssang 双,” which means “double” and the Korean character “cupul 꺼풀,” which means “cover.” It has been estimated that 30% to 50% of East Asians (China, Korea, and Japan) have a natural supratarsal crease. The earliest procedures began in Japan in the early1900s, and have been more recently modified by Korean and Chinese plastic surgeons.
The Asian blepharoplasty procedure has often been called a “westernizing” procedure. This description is a gross oversimplification of its role in function and form. Functionally, patients may request this procedure to address corneal irritation from eyelash inversion, ptosis, or pseudoptosis. In form, patients may request this procedure for purely aesthetic reasons, but the most important principle to remember in Asian blepharoplasty is that is it not a “westernizing” procedure. Patients universally want a natural look that respects their Asian identity. They want a look that naturally “opens the eye” and brings out its inherent shape and beauty ( Fig. 1 ). The tell-tale signs of a poor Asian blepharoplasty are an excessively high and thick supratarsal crease that is overly stylized and contrived. Correction of this disfigurement is fraught with complexities and unpredictable results.
The key elements in Asian blepharoplasty require finesse, precision, and a clear understanding of anatomy. The patient’s goals and priorities must be clearly defined. Despite satisfaction rates that vary widely (50%–90%), Asian upper lid blepharoplasty can be extremely rewarding and can provide a unique opportunity to create an expert niche within an aesthetic eyelid practice (W.S. Yum, personal communication, GAAM Plastic Surgery, Gang Nam Gu, Seoul, Korea, 2008).
Introduction
Upper lid blepharoplasty is the most common plastic surgery procedure in Asia and has consistently maintained its position over the past three decades as cultural acceptance and techniques have evolved. Eyelid aesthetics cannot be underestimated because they can exert significant social and economic influence in an extremely homogenous Asian society. A highly competitive culture mixed with modern values for beauty has created a constant demand for this procedure.
Surgical creation of the supratarsal crease has become synonymous with the term “double eyelid” surgery. The premise of the operation is to create a supratarsal crease that creates an eyelid that is more aesthetically pleasing. The term “double eyelid” is a bit of a misnomer, because creation of a supratarsal crease does not actually create another eyelid; it is simply a translation of the Korean term “ssang-cupul” (쌍꺼풀 双眼皮), which has come about from the Chinese character “ssang 双,” which means “double” and the Korean character “cupul 꺼풀,” which means “cover.” It has been estimated that 30% to 50% of East Asians (China, Korea, and Japan) have a natural supratarsal crease. The earliest procedures began in Japan in the early1900s, and have been more recently modified by Korean and Chinese plastic surgeons.
The Asian blepharoplasty procedure has often been called a “westernizing” procedure. This description is a gross oversimplification of its role in function and form. Functionally, patients may request this procedure to address corneal irritation from eyelash inversion, ptosis, or pseudoptosis. In form, patients may request this procedure for purely aesthetic reasons, but the most important principle to remember in Asian blepharoplasty is that is it not a “westernizing” procedure. Patients universally want a natural look that respects their Asian identity. They want a look that naturally “opens the eye” and brings out its inherent shape and beauty ( Fig. 1 ). The tell-tale signs of a poor Asian blepharoplasty are an excessively high and thick supratarsal crease that is overly stylized and contrived. Correction of this disfigurement is fraught with complexities and unpredictable results.
The key elements in Asian blepharoplasty require finesse, precision, and a clear understanding of anatomy. The patient’s goals and priorities must be clearly defined. Despite satisfaction rates that vary widely (50%–90%), Asian upper lid blepharoplasty can be extremely rewarding and can provide a unique opportunity to create an expert niche within an aesthetic eyelid practice (W.S. Yum, personal communication, GAAM Plastic Surgery, Gang Nam Gu, Seoul, Korea, 2008).
Anatomy of the Asian eyelid
The anatomy of the Asian eyelid has been studied in great detail over the past decades. Despite some controversy, key anatomic differences remain: (1) an absent or short supratarsal crease, (2) a shorter tarsus, (3) descending preaponeurotic fat, and (4) minimal to absent connections between the levator aponeurosis to the upper lid dermis.
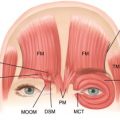
These internal anatomic differences combined with classic outer characteristics create the classic Asian eyelid ( Fig. 2 ). Outer characteristics include an almond-shaped fissure with varying degrees of slant, lash ptosis, and medial epicanthal fold.
With these differences in mind, it is important to recognize functionally that the inferior extension of the orbital septum acts as a barrier between the dermis and the levator that leads to a poorly defined or absent crease. This “inferior extension,” interchangeably known as the “preaponeurotic fat,” descends close to the eyelid margin. This key anatomic difference allows the surgeon to perform the appropriate maneuvers to create or manipulate the supratarsal crease. It also explains why certain techniques have advantages in creation, control, and longevity of the supratarsal crease.
The other anatomically important zone is the medial epicanthal fold, which may have a variable shape, presence, and severity. The epicanthal fold is the skin flap at the medial portion of the upper eyelid that descends along the side of nose and can obscure the medial globe and inner punctum making the pupils seem closer to the midline. In severe cases, the eyes may appear “cross eyed,” with the medial portion of the eye blunted by the web of the eipcanthal fold. Several types of medical epicanthal folds have been described ( Table 1 ). The most common in Asians is types 2 and 3, with either being amenable to epicanthoplasty. Identifying its severity and functional significance is critical in performing a successful Asian upper lid blepharoplasty, which now combines treatment of both areas simultaneously.
These anatomic points can be contrasted to the Caucasian upper eyelid ( Fig. 3 ), where the septum fuses with the levator 5 to 10 mm above the tarsal border. This higher point of fusion allows interdigitations of the levator to the subdermal surface creating the higher supratarsal crease that is characteristic of the white eyelid. The supratarsal crease is typically a semilunar shape with a parallel crease.
Evaluation
A thorough evaluation of the eyelid is performed at the initial consultation. In addition to the standard evaluation, it is critical to understand the patient’s sense of aesthetics regarding the eye and their goals. It is easy to simply “create a fold”; it is much more difficult to create one that is functional and aesthetically pleasing. When a patient brings in photographs demanding that their eyelid look like a specific “movie star,” it is important to caution and emphasize that the fold shape is not necessarily a function of the surgery and technique, but just as much their inherent anatomy and “crease tendency.” The “crease tendency” is a term the authors have used with patients to demonstrate where their supratarsal crease “wants to go” when choosing different fold heights. Showing patients crease shape and height immediately in the mirror during the consultation can address patient expectation dramatically.
Fold Height
In the initial evaluation phase, the first point to address is the patient’s sense of fold height. Most patients already come with some idea of fold height, in the range of low, moderate, and high. The moderate height, the most commonly requested, indicates that the patient is looking for a natural-appearing supratarsal crease. The high fold height is typically requested to attract greater attention to the fold, particularly for ease of makeup application. The low fold height is typically reserved for the male patient who desires a subtle fold ( Fig. 4 ). Measuring the tarsal height by flipping the lid open on the conjuctival side can determine if a high fold is even technically achievable. At this time, it is good to note the degree of lash ptosis, the angle at which eyelashes are pointing from the globe.
Selection of fold height naturally follows to create a crease shape. The shape can be a parallel crease ( Fig. 5 ) or a nasally tapered crease ( Fig. 6 ). In general, a high fold yields a parallel crease, whereas a moderate to low fold yields a nasally tapered crease. Crease heights are measured with key millimeter measurements in mind: 5 to 6 mm is a low crease, 7 to 8 mm is a moderate crease, and 9 to 10 mm is a high crease. These are guidelines and have to be adjusted when skin excision is involved. Measurements are best done with a surgical caliper.
Medial Epicanthus
Next, the medial epicanthus is addressed. The medial epicanthal fold must first be recognized, and then should be addressed based on patient expectation. In general, the stronger the medial epicanthal fold, the more tendency there is to create a nasally tapered crease. If the patient desires a parallel crease or specifically wants the epicanthal fold diminished, the medial epicanthoplasty procedure must be discussed in detail.
Symmetry
Patients may also present with asymmetric or multiple folds ( Fig. 7 ). These elements must be pointed out explaining the greater variability and potential higher degree of difficulty in obtaining exact symmetry. Adding to the complexity is identifying degrees of subclinical ptosis and pseudoptosis. Subclinical ptosis should be suspected when a patient shows significant frontalis strain ( Fig. 8 , left). With the frontalis muscle overcompensating before surgery, the frontalis relaxes after the blepharoplasty (see Fig. 8 , right), which makes the ptosis even more apparent.