Upper eyelid blepharoplasty is one of the most common facial plastic surgeries performed in the United States. Understanding how brow position contributes to the upper eyelid appearance is essential. Consistent and desirable surgical outcomes are best achieved with a detailed knowledge of periorbital anatomy. The surgeon must understand patients’ expectations and ensure that surgical goals are realistic. The potential complications and their management are discussed. The goal of upper eyelid blepharoplasty is to create a sculpted upper lid with a visible pretarsal strip and subtle fullness along the lateral upper lid–brow complex. The trend toward volume preservation is discussed.
Key points
- •
Upper eyelid blepharoplasty is one of the most common facial plastic surgeries performed in the United States.
- •
Understanding how brow position contributes to the upper eyelid appearance is essential.
- •
Consistent and desirable surgical outcomes are best achieved with a detailed knowledge of periorbital anatomy.
- •
The surgeon must take time to understand each patient’s expectations and ensure that the surgical goals are realistic.
- •
Although complications are rare, a frank discussion of operative risks is necessary. The potential complications and their management are discussed.
- •
The goal of upper eyelid blepharoplasty is to create a sculpted upper lid with a visible pretarsal strip and subtle fullness along the lateral upper lid–brow complex. The trend toward volume preservation is discussed.
Introduction
People relate to each other through the eyes. In social interactions, we notice the eyes before any other facial feature. Over time, the eyelids and periorbital complex go through changes that convey the impression of fatigue, even if a person is well rested. These changes are often the first signs of aging noted by a patient, explaining why blepharoplasty is one of the most common facial plastic surgeries performed in the United States.
The eyes are framed in a complex and dynamic bony and soft tissue landscape. This includes the upper and lower lids, brow and forehead, and the midface. Although this article focuses on the upper eyelids, aging and rejuvenation of each of these facial units must be evaluated in the proper context. As will be discussed, in evaluating candidacy for upper eyelid blepharoplasty, the surgeon and patient must critically assess the contribution of the eyebrow to the periorbital appearance.
The importance of upper eyelid rejuvenation is highlighted by its history. The original writings on eyelid surgery are from the Sushruta, a document created by an Indian surgeon 2000 years ago. Over the ensuing centuries, surgeons continued to document their experience with eyelid surgery, with the focus on reduction of excess eyelid skin through either cauterization or resection. Although periorbital fat removal was previously described, it was Costanares in 1951 who described the anatomy of the orbital fat compartments. In the following 3 decades, the predominant surgical wisdom was that removal of fat, orbicularis oculi, and skin was the key to restoring a youthful-appearing upper eyelid. It was not until the 1990s that conservation of volume in the upper eyelid became an essential part of surgical rejuvenation.
The youthful upper eyelid maintains a sharp upper lid crease with visible pretarsal skin. The subcutaneous layers contain sufficient elasticity and volume such that excess eyelid skin is minimized and the preseptal and pretarsal skin remains smooth and fluid as the lid moves. Redundant eyelid skin, upper lid fat protrusion, and lateral orbital hooding are all signs of aging. Similarly, a hollow upper lid can convey an aged appearance or the skeletal look characteristic of an aggressive upper blepharoplasty. The task of the esthetic surgeon is to strike the balance between excess soft tissue and volume depletion. This remains a debated facet of upper eyelid surgery and facial plastic surgery in general. The second ongoing controversy in upper eyelid surgery is incision design, as is discussed.
Introduction
People relate to each other through the eyes. In social interactions, we notice the eyes before any other facial feature. Over time, the eyelids and periorbital complex go through changes that convey the impression of fatigue, even if a person is well rested. These changes are often the first signs of aging noted by a patient, explaining why blepharoplasty is one of the most common facial plastic surgeries performed in the United States.
The eyes are framed in a complex and dynamic bony and soft tissue landscape. This includes the upper and lower lids, brow and forehead, and the midface. Although this article focuses on the upper eyelids, aging and rejuvenation of each of these facial units must be evaluated in the proper context. As will be discussed, in evaluating candidacy for upper eyelid blepharoplasty, the surgeon and patient must critically assess the contribution of the eyebrow to the periorbital appearance.
The importance of upper eyelid rejuvenation is highlighted by its history. The original writings on eyelid surgery are from the Sushruta, a document created by an Indian surgeon 2000 years ago. Over the ensuing centuries, surgeons continued to document their experience with eyelid surgery, with the focus on reduction of excess eyelid skin through either cauterization or resection. Although periorbital fat removal was previously described, it was Costanares in 1951 who described the anatomy of the orbital fat compartments. In the following 3 decades, the predominant surgical wisdom was that removal of fat, orbicularis oculi, and skin was the key to restoring a youthful-appearing upper eyelid. It was not until the 1990s that conservation of volume in the upper eyelid became an essential part of surgical rejuvenation.
The youthful upper eyelid maintains a sharp upper lid crease with visible pretarsal skin. The subcutaneous layers contain sufficient elasticity and volume such that excess eyelid skin is minimized and the preseptal and pretarsal skin remains smooth and fluid as the lid moves. Redundant eyelid skin, upper lid fat protrusion, and lateral orbital hooding are all signs of aging. Similarly, a hollow upper lid can convey an aged appearance or the skeletal look characteristic of an aggressive upper blepharoplasty. The task of the esthetic surgeon is to strike the balance between excess soft tissue and volume depletion. This remains a debated facet of upper eyelid surgery and facial plastic surgery in general. The second ongoing controversy in upper eyelid surgery is incision design, as is discussed.
Anatomy
Brow and Eyelid Topography
When assessing upper eyelid appearance, the brow position and shape must be evaluated. Brow ptosis can be the primary reason for an aged appearance of the upper lid complex. In women, a youthful brow starts at the orbital rim in the same axis as the alar-facial crease. The brow arches superiorly with the highest point over the lateral canthus, approximately 1 cm from the bony rim ( Fig. 1 ). Laterally, the brow descends but remains above the orbital rim. In men, the brow maintains a straight course along the bony orbital rim.
The upper lid crease is formed by the condensation of the levator aponeurosis with the orbital septum and orbicularis fascia and its insertion into the skin. In white women, the crease is typically 10 to 12 mm above the lash line. In men, it ranges from 7 to 8 mm. The Asian upper lid crease is lower or absent because of a more inferior insertion of the distal aponeurosis into the orbital septum and variation in the aponeurosis insertion into the skin.
The palpebral fissure is typically 28 to 30 mm wide and 9 to 10 mm high. The visible portion of the globe is almond shaped with the lateral canthal angle set on average 2 mm higher than the medial canthal angle. Although the inferior lid runs across the inferior limbus, the superior lid sits 2 mm inferior to the superior limbus. The most superior point of the upper eyelid is just nasal to the vertical midpupillary line (see Fig. 1 ).
Surgical Anatomy
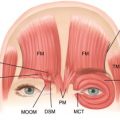
The upper eyelid is divided into anterior and posterior lamellae ( Fig. 2 ). The anterior lamella consists of the thin lid skin, a subcutaneous layer, absent in the pretarsal area, and the orbicularis oculi muscle. The orbicularis is divided into 3 regions: the orbital portion, which interdigitates with the corrugators superiorly, the preseptal portion, and the pretarsal portion.
The posterior lamella consists of the conjunctiva, the tarsal plate, Muller muscle, and the levator aponeurosis. The conjunctiva is the epithelial mucous membrane lining the lid. The tarsal plate of the upper lid is a dense fibrous structure ranging from 10 to 12 mm in vertical height. Muller muscle is a smooth muscle innervated by the sympathetic nervous system that lies deep to the levator aponeurosis. It inserts on the superior border of the tarsal plate. The levator aponeurosis is the fibrous extension of the levator palpebrae superioris and is the main upper lid retractor, controlled by the third cranial nerve. The aponeurosis inserts along the anterior aspect of the superior tarsus and fuses with the orbital septum, orbicularis, and skin at a variable point superior to the tarsus, forming the supratarsal crease.
The orbital septum, sometimes referred to as the middle lamella, begins along the arcus marginalis. It serves as a fibrous barrier between the anterior and posterior lamellae. Posterior to the septum, above the tarsal plate, is the orbital fat. Weakening of the septum causes bulging of the fat, a stigmata of the aging upper eyelid.
The orbital fat lies posterior to the septum and anterior to the levator aponeurosis, superior to the tarsal plate. There are 2 fat compartments: the central and medial fat pads ( Fig. 3 ). These are separated by the trochlea of the superior oblique muscle. The central, or preaponeurotic, fat pad is larger and less vascular, with a more yellow appearance. The medial, or nasal fat pad is more dense and white in color. The lateral compartment consists of the lacrimal gland and a variable amount of associated fat.
Evaluation for upper eyelid blepharoplasty
Proper evaluation of surgical candidacy for upper eyelid blepharoplasty requires a thorough understanding of the correctable changes of the aged eyelid as well as the patient’s medical, ophthalmologic, and psychological history. Perhaps most important is for the surgeon to pay close attention to the expectations of the patient.
Aging of the upper eyelid begins as early as the late 20s ( Fig. 4 ). The skin thins farther from its already delicate baseline. Dynamic folds develop over the lateral orbicularis, known as crow’s feet. As the elasticity of the subcutaneous tissue decreases, the dermatochalasis, or eyelid skin laxity, progresses, leading to hooding over the fixed pretarsal skin and muscle. Along with skin laxity, the orbicularis oris hypertrophies and relaxes, adding volume to the hooded preseptal tissue. Over time, the orbital septum weakens, allowing pseudoherniation of the medial and central fat pads and visible irregular fullness in these areas, known as steatoblepharon. Fullness in the lateral compartment can be caused by either a ptotic lacrimal gland or occasionally fat pseudoherniation. If a ptotic lacrimal gland is present, a firm nodule can frequently be palpated just deep to the bony margin. If present, the gland can be suspended just under the orbital rim intraoperatively. As the brow descends, the thicker brow skin and soft tissue crowds the upper eyelid and contributes to the bulk of lateral hooding. It is crucial to determine the contribution of the brow to the upper eyelid appearance. For example, in cases of severe brow ptosis, excision of skin inferior to the brow during a blepharoplasty can cause worsening of brow drooping. In these cases, a successful outcome requires a procedure to lift the brow.
Preoperative Photographs
To properly manage a patient’s expectations, standardized preoperative photography must be performed. In addition, close-up pictures of the eyes from front and profile views in primary and up gaze must be obtained. Photographs should be reviewed with the patient to allow a discussion about preoperative asymmetry. Unless prompted, patients will frequently not recognize baseline facial, eyelid, and brow asymmetry until they are analyzing their appearance critically in the postoperative period. This is especially true of asymmetric palpebral fissures, which frequently are noticed by the patient only after eyelid surgery. A frank preoperative discussion will guide a patient’s postoperative analysis of results. Reviewing photographs also facilitates the patient’s understanding of how the brow is contributing to the upper eyelid appearance.
Ophthalmologic History
A detailed ophthalmologic history is essential before proceeding with upper eyelid blepharoplasty. A patient’s history of dry-eye symptoms, ocular infections, visual disturbances, blink function, and prior surgical history is elicited. A standard vision test and extraocular muscle examination should be performed as part of the preoperative physical. Additionally, the senior author (VCQ) refers all blepharoplasty patients to an ophthalmologist for baseline visual acuity testing, Schirmer tear testing, and visual field testing for patients with possible compromise.
Baseline Ptosis
Recognizing baseline unilateral or bilateral ptosis is paramount. Ptosis should be documented to the nearest 0.5 mm and is best described using the margin-to-reflex distance-1 (MRD1), or distance from the pupillary light reflex to the upper lid margin. Additionally, levator excursion should be noted. This is the lid mobility in millimeters from extreme upgaze to downgaze with the brow immobilized. Good excursion is 10 mm or greater, whereas moderate mobility is 5 to 9 mm and poor function is less than 4 mm. Patients with impaired levator excursion and documented ptosis should be counseled and provided a workup for ptosis correction, which is beyond the scope of this article.
Medical Comorbidities
Medical comorbidities must be assessed preoperatively to achieve safe and reliable results. A history of bleeding dyscrasias or conditions requiring anticoagulation, hypertension, and diabetes are elicited. Anticoagulation, including dietary supplements that disrupt the clotting cascade, must be stopped 2 weeks preoperatively. Patients with known thyroid disease may have ophthalmologic issues caused by their condition. Any condition that could contribute to dry-eye symptoms, including autoimmune and global inflammatory disease processes, should be explored. If there is a predisposing factor for dry-eye pathology, the Schirmer test is performed. This is done via the standard ophthalmology referral in this center.
Patient Psychological Status
Finally, an assessment of the patient’s psychological status is a key component of the preoperative evaluation. The surgeon must determine whether a patient’s motivations for surgery are realistic and are aligned with a healthy psychological profile. Communicating honestly about a patient’s preoperative expectations, about what is achievable, and about baseline asymmetries that may be accentuated postoperatively help to establish an honest dialogue. If there is concern on the surgeon’s side regarding a patient’s desires and expectations, or even the patient’s psychological well-being, it is prudent to delay or cancel the surgical procedure and assist the patient in finding appropriate support.
Related posts:
 Advances in Esthetic Surgery from Four Specialties
Brow and Upper Lid Aesthetics and Rejuvenation: Views from Four Disciplines
Advances in Esthetic Surgery from Four Specialties
Brow and Upper Lid Aesthetics and Rejuvenation: Views from Four Disciplines
 Contemporary Concepts in Brow and Eyelid Aging
Technical Considerations in Endoscopic Brow Lift
Adjunctive Fat Grafting to the Upper Lid and Brow
Asian Upper Lid Blepharoplasty Surgery
Contemporary Concepts in Brow and Eyelid Aging
Technical Considerations in Endoscopic Brow Lift
Adjunctive Fat Grafting to the Upper Lid and Brow
Asian Upper Lid Blepharoplasty Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


